Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251108_002
Breaking the Wall Along the Tunnel: To Drill or Pulse
By Syed Saleh Syed Sheikh, M.Azlan Aseri, M.Aizuddin M.Zulastri, R.A.Wafy R.M.Rooshdi, L.Kee Wei, A.Syadi M.Zuhdi, Chee.K Han
Presenter
Syed Saleh Syed Sheikh
Authors
Syed Saleh Syed Sheikh1, M.Azlan Aseri1, M.Aizuddin M.Zulastri1, R.A.Wafy R.M.Rooshdi2, L.Kee Wei1, A.Syadi M.Zuhdi1, Chee.K Han1
Affiliation
University Malaya Medical Centre, Malaysia1, University Putra Malaysia, Malaysia2
View Study Report
CASE20251108_002
Coronary - Complex PCI - Calcified Lesion
Breaking the Wall Along the Tunnel: To Drill or Pulse
Syed Saleh Syed Sheikh1, M.Azlan Aseri1, M.Aizuddin M.Zulastri1, R.A.Wafy R.M.Rooshdi2, L.Kee Wei1, A.Syadi M.Zuhdi1, Chee.K Han1
University Malaya Medical Centre, Malaysia1, University Putra Malaysia, Malaysia2
Clinical Information
Relevant Clinical History and Physical Exam
71 years old lady with background of end stage kidney disease on hemodialysis and hypertension presented with central gripping chest pain associated with diaphoresis for 2 days. The condition was made worse by intradialytic hypotension and angina which required premature cessation of the hemodialysis. On presentation, clinical examination demonstrated the presence of fine crackles on lower zones of both lungs. Other systemic examinations were unremarkable.
Relevant Test Results Prior to Catheterization
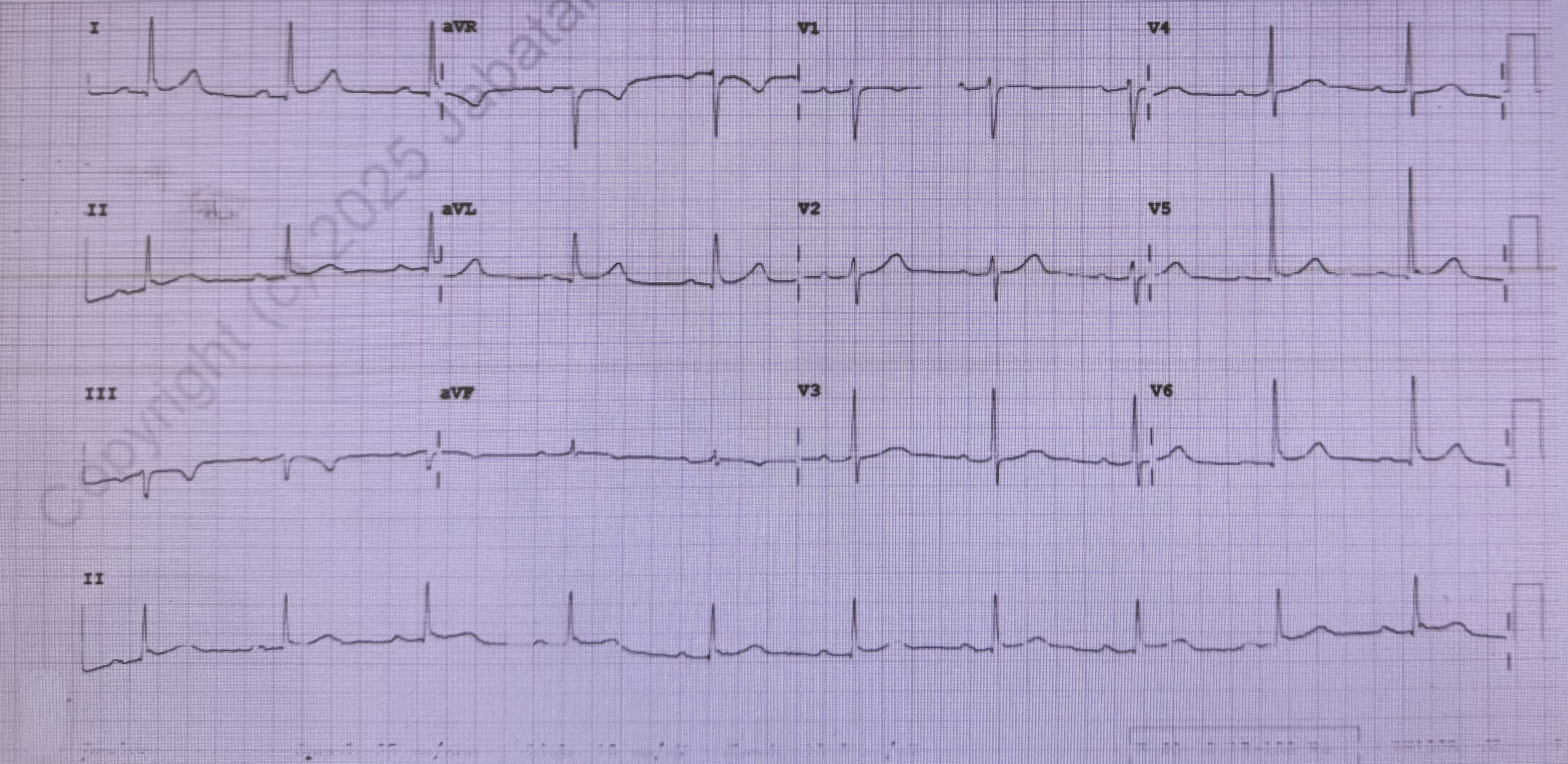
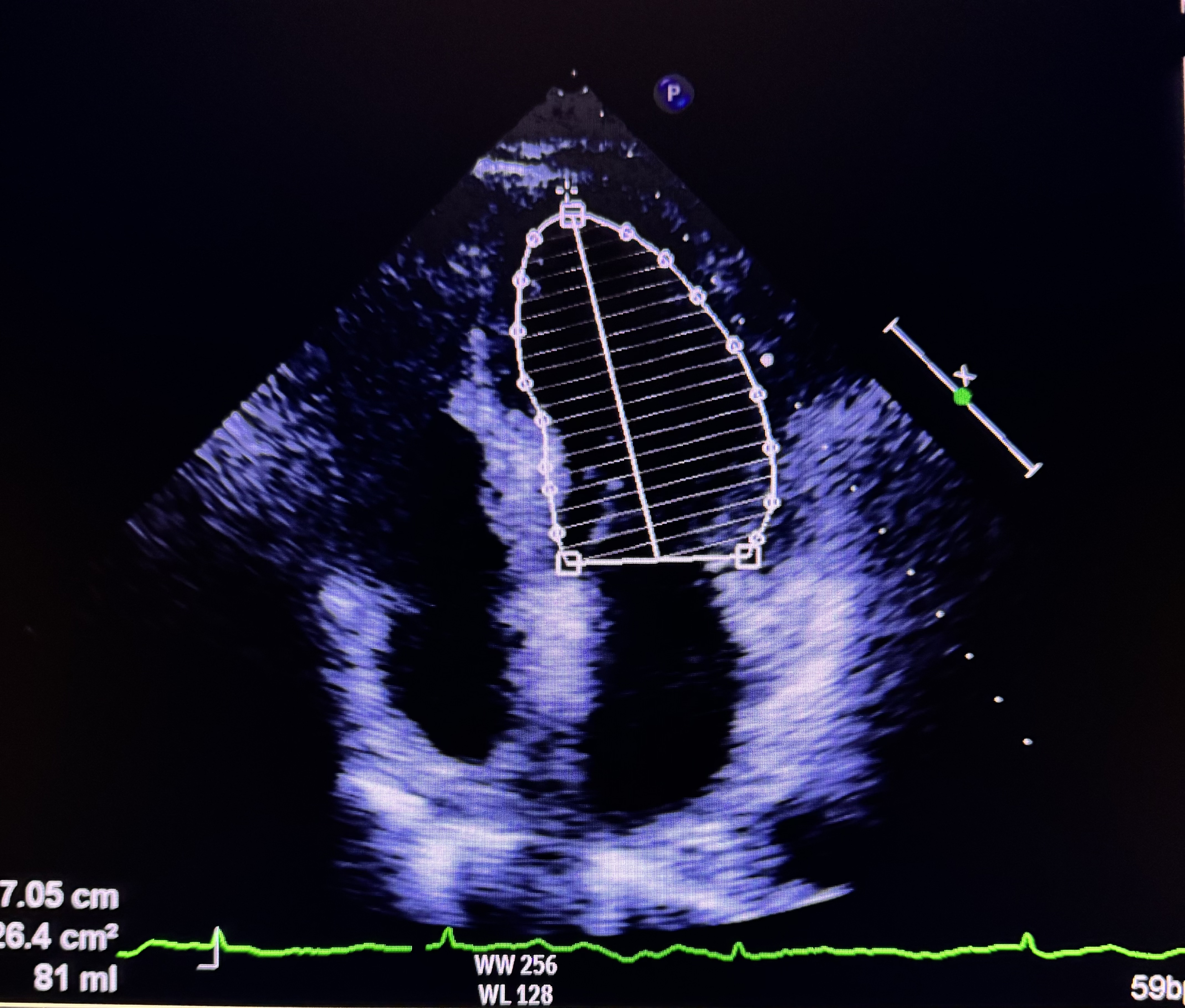
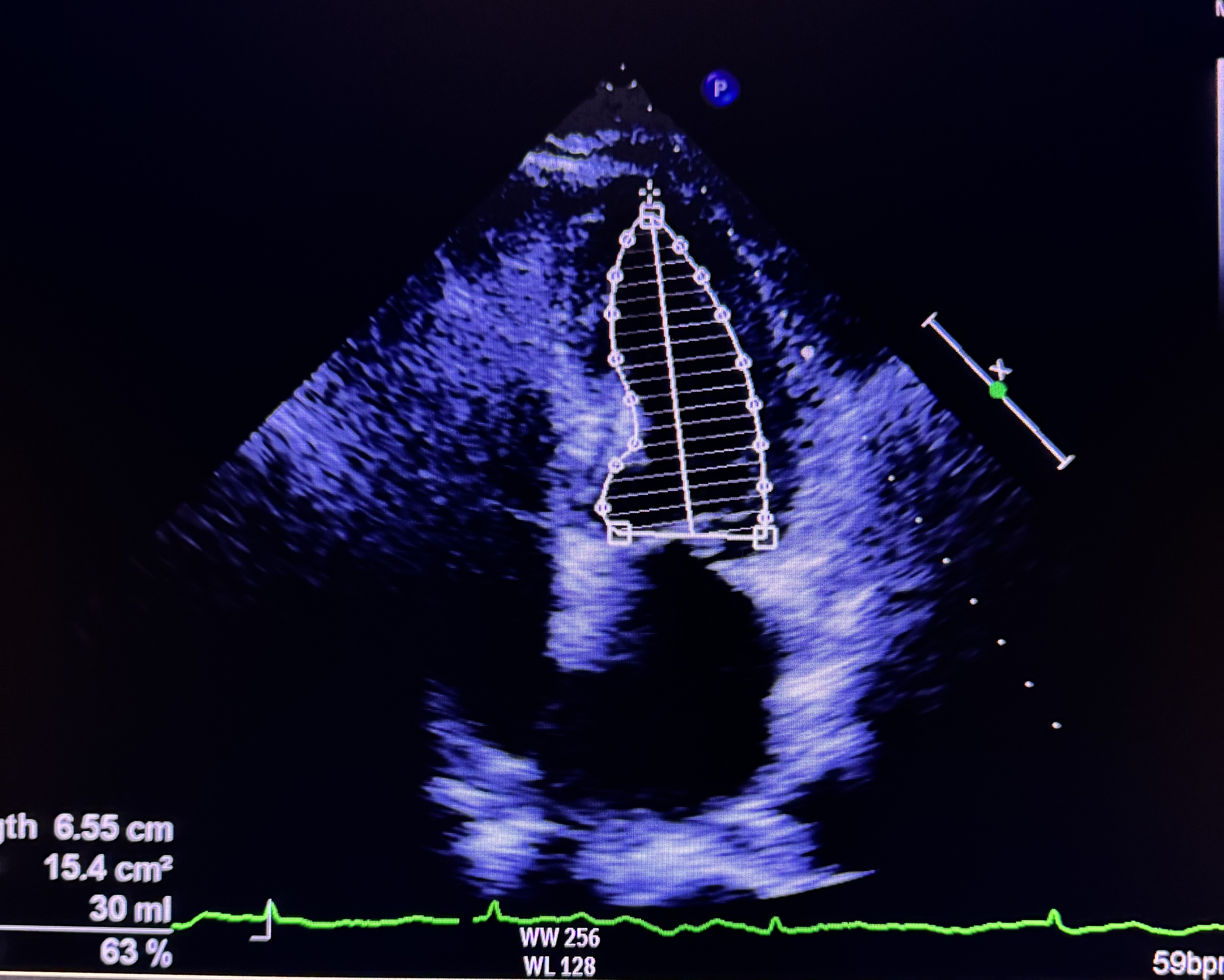
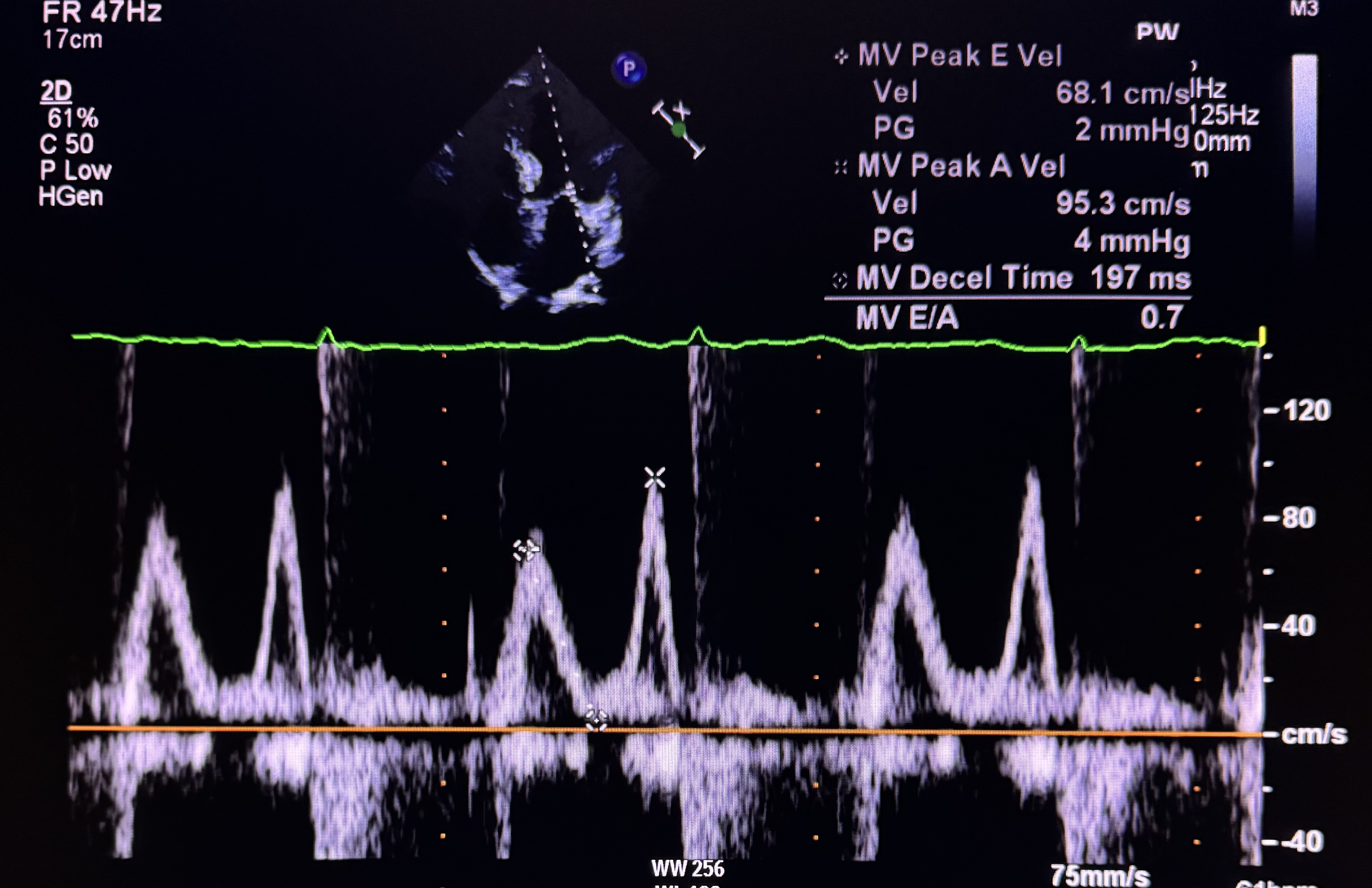
Cardiac Hs troponin was normal (20.4). Electrocardiogram demonstrated sinus rhythm 65 beats/min with isolated T inversion on lead IIIEchocardiogram demonstrated normal left ventricular systolic function with ejection fraction of 70%. Diastolic function corresponded with grade 1 dysfunction and no wall motion abnormalities. Her left ventricular size was normal with no evidence of mechanical complication of acute coronary syndrome. These informations led to the diagnosis of unstable angina
 IMG_3656.mov
IMG_3656.mov
IMG_3659.mov
IMG_3664.mov
Relevant Catheterization Findings
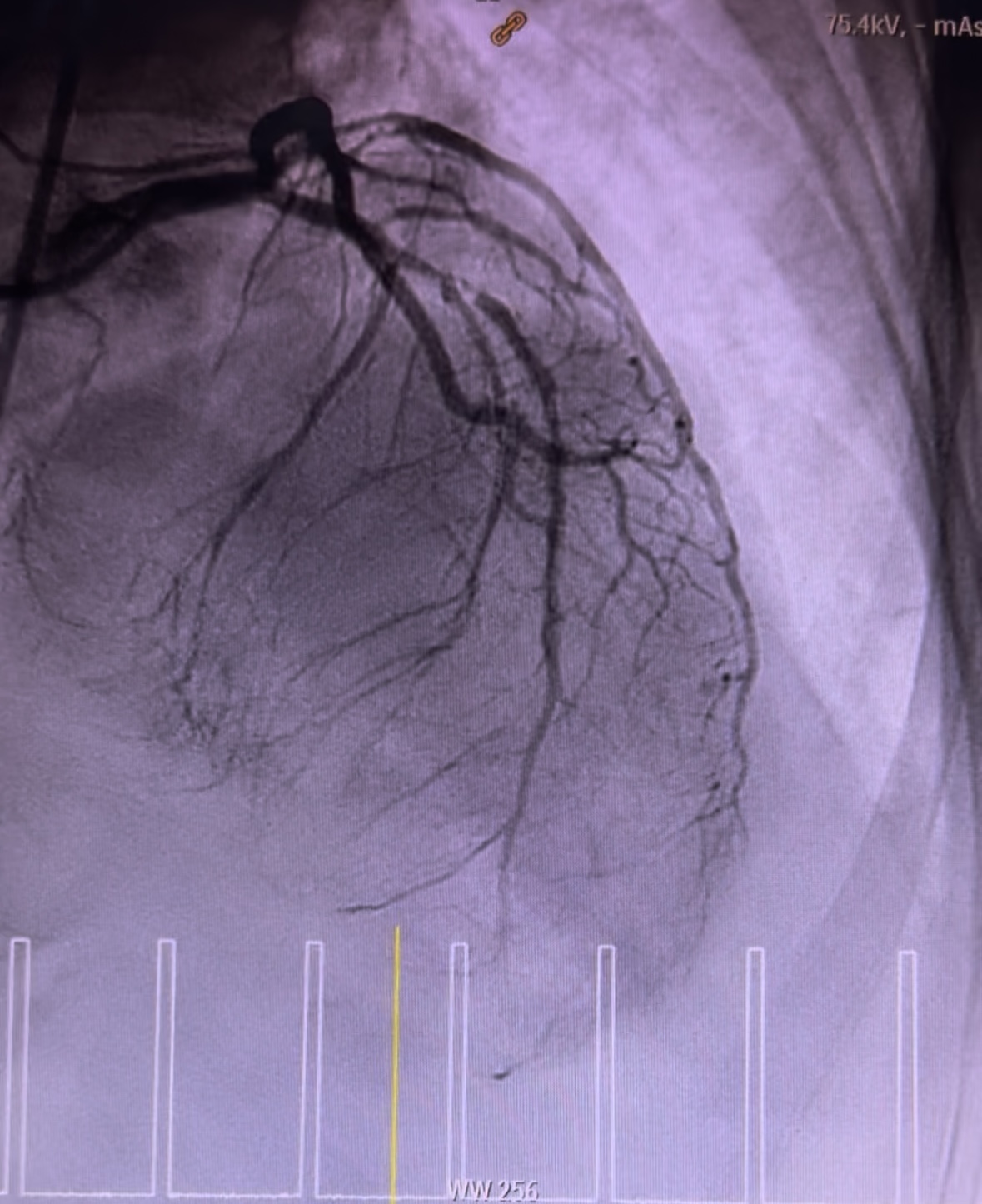
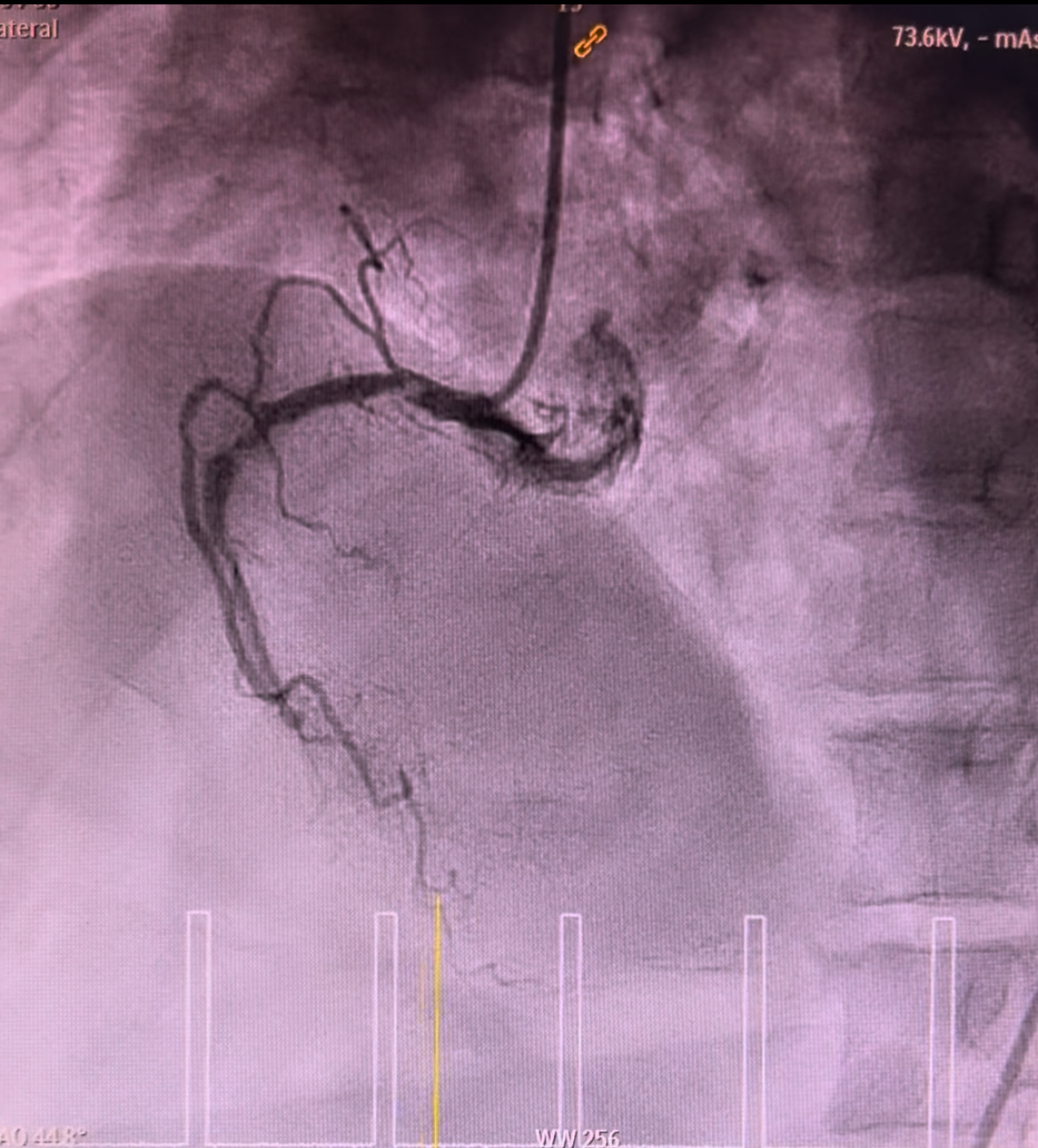
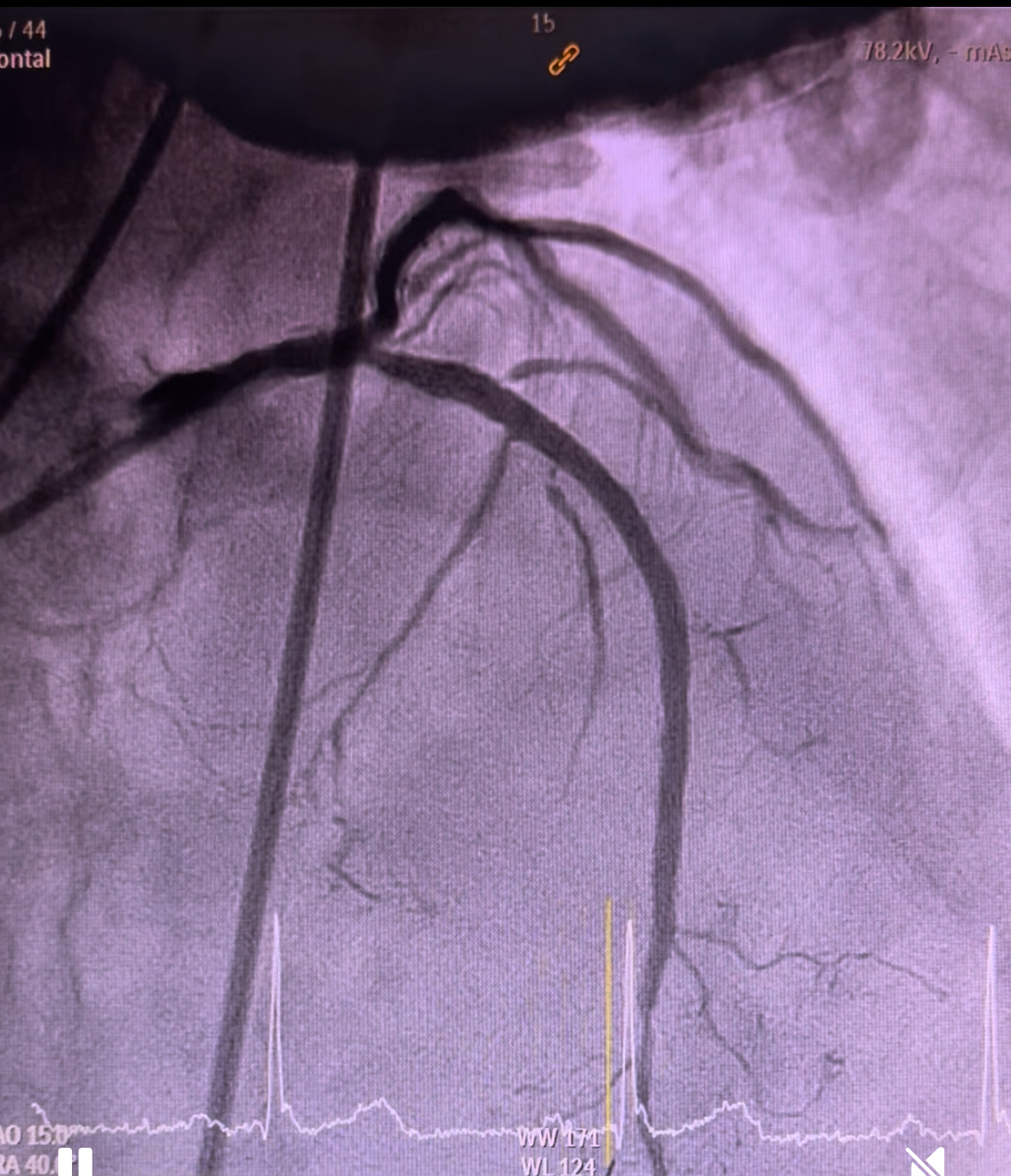
Coronary angiogram demonstrated smooth left main, 90% stenosis in the proximal left circumflex, 99% focal stenosis with severe calcification at mid LAD, followed by mild diffuse plaque until the distal end, and 90% stenosis at ostial D1. Right coronary was calcified with 80% stenosis at the proximal segment, 90% stenosis at the mid segment, and CTO at the distal segment. Discussion was held with cardiothoracic surgeons in which CABG was viewed incompatible.

IMG_3625.mov
IMG_3623.mov
IMG_3629.mov
Interventional Management
Procedural Step
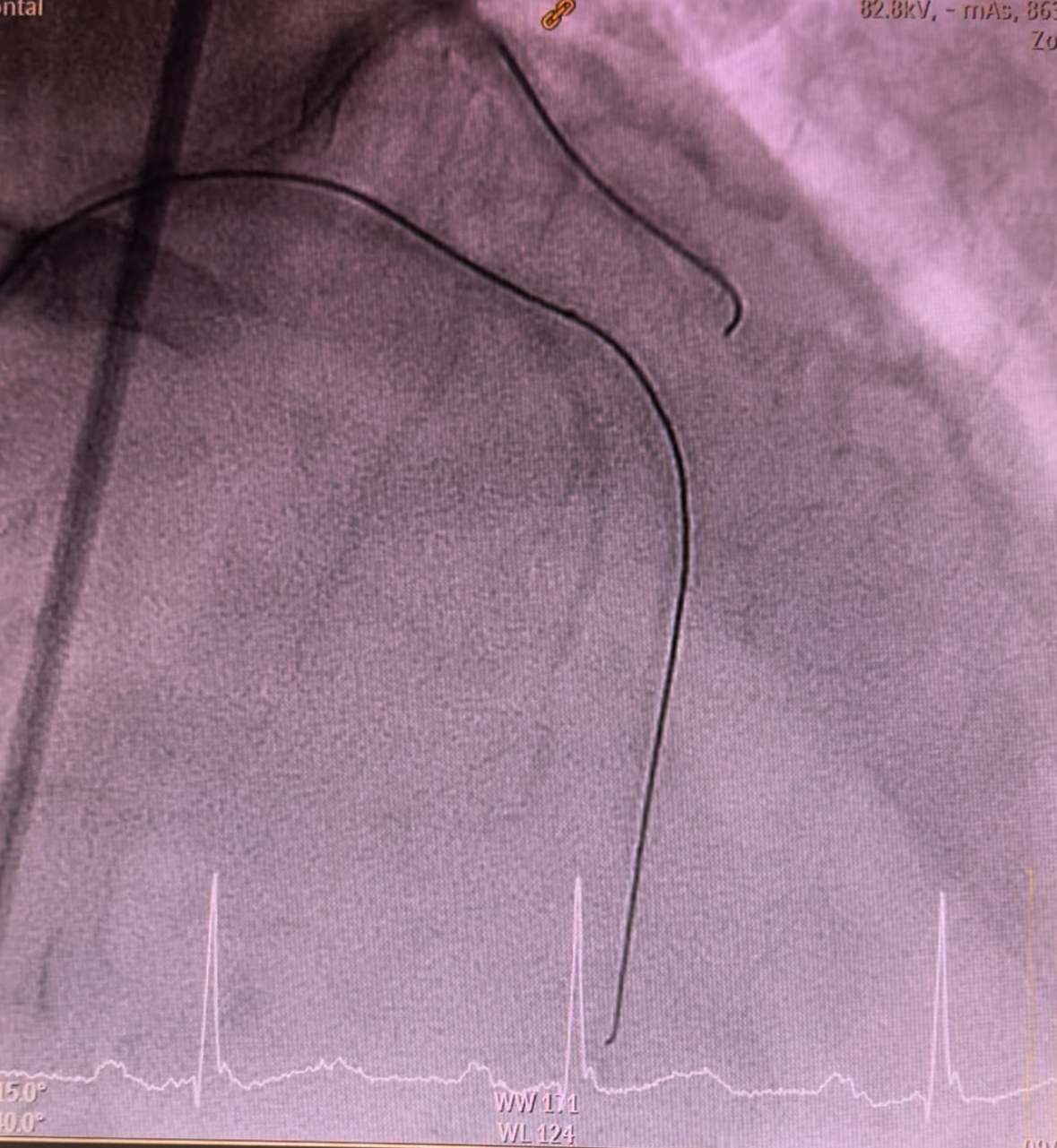
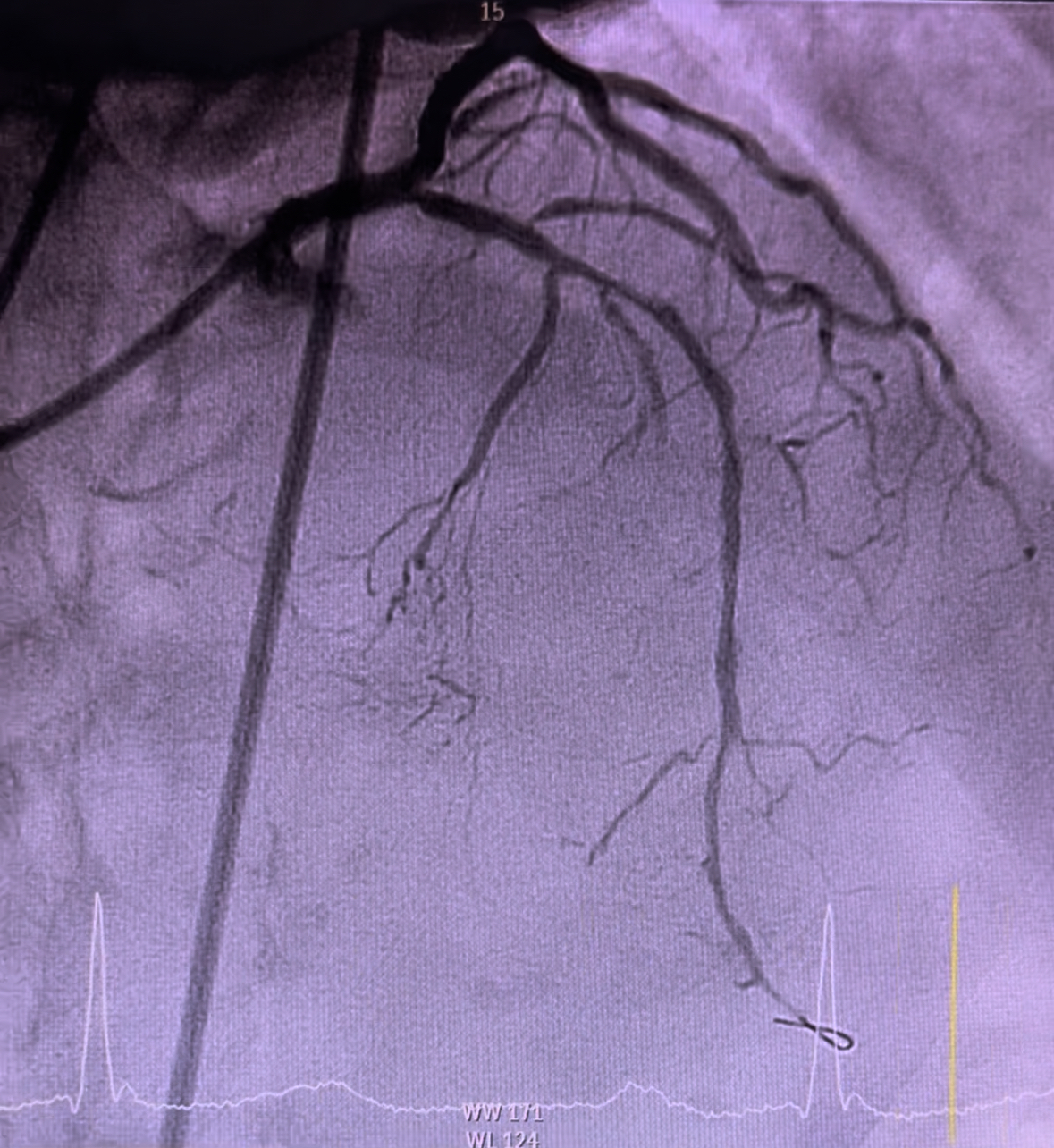
Angioplasty to left circumflex was begun by catheter engagement with XB LAD 3.5 7Fr. Wiring was done with run-through followed by lesion preparation using NC Sapphire 2.5 x 15mm inflated at 12atm. Subsequently, serial upsizing dilation was done with NC Sapphire 3.0 x 15mm inflated at 14atm. A 3.0 x 18mm stent was deployed displaying a good angiographic result. Subsequently, wiring was attempted through the LAD using Runthrough via fine cross microcatheter. Failure to pierce through the calcified stenosis has led to an escalation of guide wire to Gaia second which able to pass through successfully. Fine cross was removed using hydraulic technique with balloon inflator. Initial preparation was done by inflating NC Sapphire 1.0 x 10mm followed by 1.5 x 10mm. Thereafter, the wire was changed to Rota wire extra support via fine cross microcatheter. Rotational atherectomy was performed using 1.5mm burr, rotating at 180,000 rpm with 3 runs back and forth from proximal to mid. Further cracking was performed using intravascular lithotripsy with a 3.0mm balloon inflated at 4atm with total of 25 pulses. Further optimization was done using NC Sapphire 2.5 x 15mm and 3.0 x 15mm expanded in the mid and proximal segments respectively. Two stents sized 3.0 x 38mm and 3.5 x 38mm were respectively deployed at mid and proximal segment via guide extension. Expansion optimisation was done with a 3.5 x 15 NC Sapphire achieving TIMI 3 flow and reestablishing the flow through the side branches.
IMG_3635.mov
IMG_3637.mov
IMG_3641.mov
Case Summary
Debulking of calcified plaque is crucial to ensure an optimal stent expansion. Preparation of complex lesion could be done using multiple methods either solely by balloon preparation, atherectomy, or intravascular lithotripsy, or combination method. This case highlights the application of rotational atherectomy combined with lithotripsy which simultaneously abrade and crack the superficial and deep calcified plaque respectively. It also highlights the intervention performed under limited coronary visualisation which merely based on angiographic evaluation to decide the strategy of lesion preparation in the setting of insufficient financial resource.