Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_041
Beating the Calcium Wall: Rotational Atherectomy Saves the Day in Low-EF ACS
By Ankit Gupta
Presenter
Ankit Gupta
Authors
Ankit Gupta1
Affiliation
AIIMS Raebareli, India1
View Study Report
CASE20251107_041
Coronary - Adjunctive Procedures (Thrombectomy, Atherectomy, Special Balloons)
Beating the Calcium Wall: Rotational Atherectomy Saves the Day in Low-EF ACS
Ankit Gupta1
AIIMS Raebareli, India1
Clinical Information
Relevant Clinical History and Physical Exam
66 Yr Old male with Diabetes, HTN , Dyslipidaemia presented with Angina Class III diagnosed as NSTEMI with Acute Decompensated Heart Failure with Moderate LV systolic dysfunction. on the basis of History and investigations patient taken up for coronary angiogram which revealed triple vessel disease

Relevant Test Results Prior to Catheterization
Relevant Catheterization Findings
A temporary pacing lead was placed in view of triple vessel disease and potential for bradyarrhythmias during atherectomy.
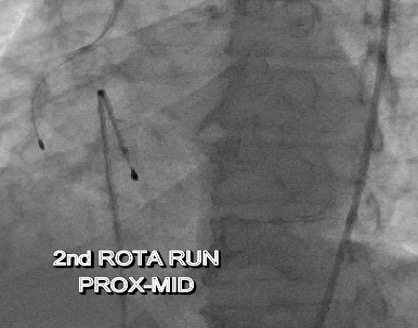
A 6F JR guiding catheter was engaged at the RCA ostium. The lesion was initially crossed using a Sion Blue wire, which was parked distally into the posterior descending artery (PDA).A 0.75 mm CTO balloon was then advanced but failed to cross the heavily calcified lesion. The wire was subsequently exchanged for a RotaWire, and rotational atherectomy was performed in three sequential runs:

 V1.mov
V1.mov
V2.mov
A 6F JR guiding catheter was engaged at the RCA ostium. The lesion was initially crossed using a Sion Blue wire, which was parked distally into the posterior descending artery (PDA).A 0.75 mm CTO balloon was then advanced but failed to cross the heavily calcified lesion. The wire was subsequently exchanged for a RotaWire, and rotational atherectomy was performed in three sequential runs:
- Proximal to mid RCA
- Mid RCA
- Mid to early distal RCA
Interventional Management
Procedural Step
A 6F JR guiding catheter was engaged at the RCA ostium. The lesion was initially crossed using a Sion Blue wire, which was parked distally into the posterior descending artery (PDA).A 0.75 mm CTO balloon was then advanced but failed to cross the heavily calcified lesion. The wire was subsequently exchanged for a RotaWire, and rotational atherectomy was performed in three sequential runs:
- Proximal to mid RCA
- Mid RCA
- Mid to early distal RCA


Case Summary
When even the smallest CTO balloon failed to cross, the burr became the breakthrough. Rotational atherectomy transformed an unyielding, calcified RCA into a successfully revascularized vessel. Guided by IVUS and supported by meticulous technique, the procedure achieved excellent stent expansion, optimal apposition, and restored TIMI III flow — reaffirming that in complex, calcified coronary lesions, Rota ablation remains the key when nothing else can pass