Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_040
Double Trouble, Double Triumph: Managing Dual LAD With DCB
By Norhaliza Am Haris
Presenter
Norhaliza Am Haris
Authors
Norhaliza Am Haris1
Affiliation
National Heart Institute, Malaysia1
View Study Report
CASE20251107_040
Coronary - Complex PCI - Bifurcation
Double Trouble, Double Triumph: Managing Dual LAD With DCB
Norhaliza Am Haris1
National Heart Institute, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 43-year-old lady with history of hypertension and dyslipidemia presented in August 2025 with an inferior ST-elevation myocardial infarction for which she underwent successful revascularization of the mid-segment of the right coronary artery with deployment of a drug-eluting stent. Angiographic assessment also revealed a dual LAD anatomy with residual severe stenosis. She was electively admitted in October 2025 for a staged percutaneous coronary intervention to the LAD lesions.
Relevant Test Results Prior to Catheterization
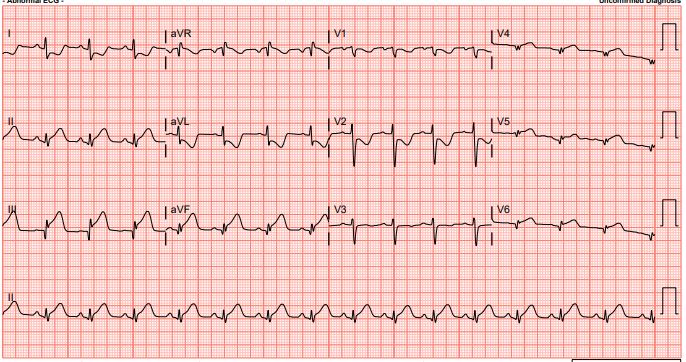
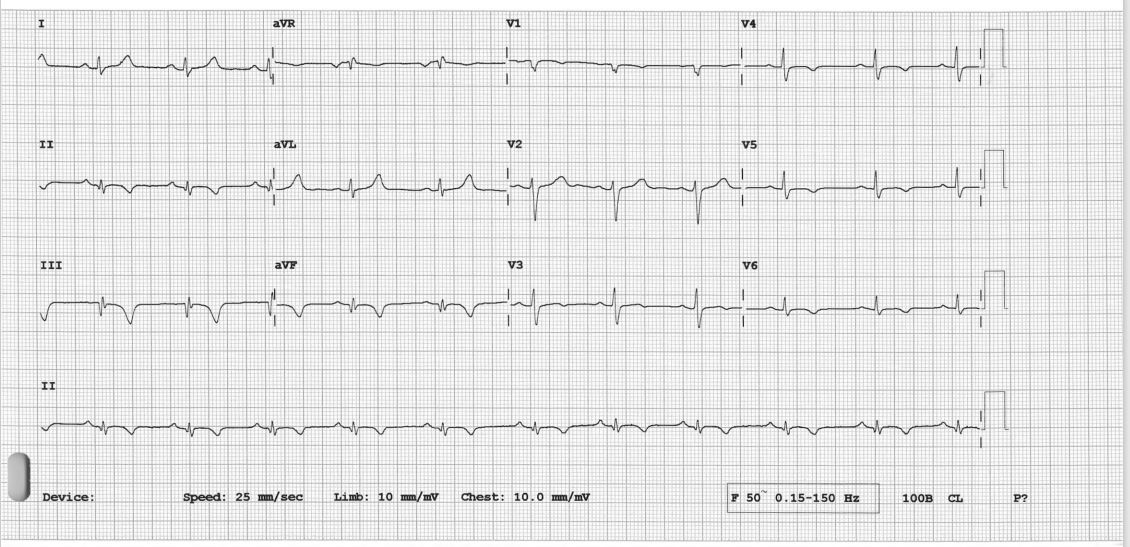
The electrocardiogram (ECG) revealed resolution of ST-segment elevation, with T-wave inversion noted over the inferior and anterolateral leads. The echocardiogram showed reduced left ventricular (LV) function with an ejection fraction (LVEF) of 38%, accompanied by regional wall hypokinesia over the LAD and RCA territories. The cardiac chambers were of normal size, the valves appeared normal, and there was no pericardial effusion.
Relevant Catheterization Findings
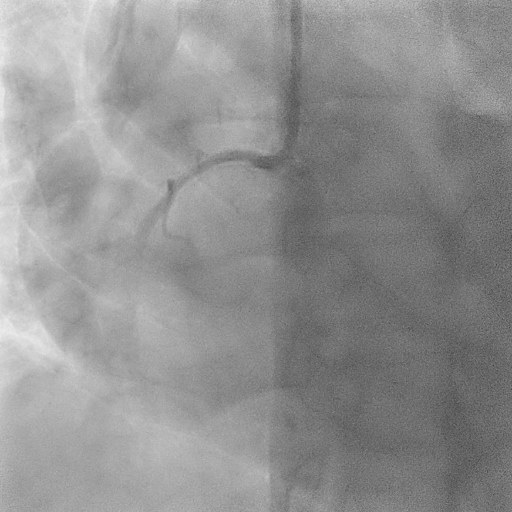
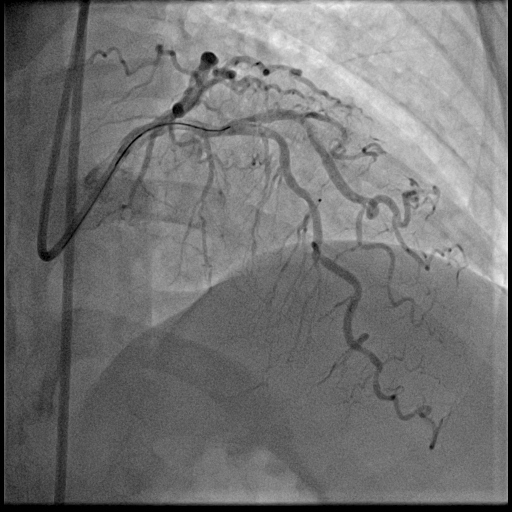
The coronary angiogram showed a right-dominant system. The right coronary artery (RCA) had a patent mid stent with mild diffuse disease and good TIMI 3 flow. The Quantitative Flow Ratio (QFR) was 0.97, indicating preserved physiological flow. A dual LAD anatomy was noted with significant bifurcation lesions (Medina 1,1,1) involving the mid first LAD and the ostial to mid second LAD. The non-dominant left circumflex artery and left main stem were normal.
 Dual LAD pre PCI.mp4
Dual LAD pre PCI.mp4
Interventional Management
Procedural Step
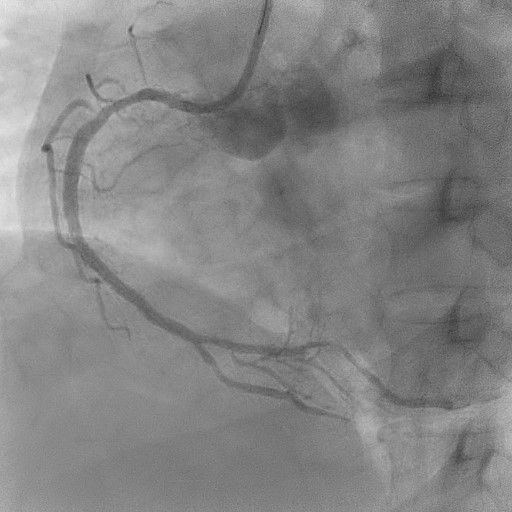
Coronary intervention was performed using an EBU 3.0, 6 Fr guiding catheter via the right radial artery approach. A Runthrough Floppy wire was advanced to the distal first LAD, and a Sion Blue wire to the second LAD. Pre-dilatation of the mid first LAD was performed using a semi-compliant (SC) 2.0 × 15 mm balloon at high pressure. Intravascular ultrasound assessment revealed fibrocalcific plaque in both vessels. The vessel reference diameter of the first LAD measured 2.5 mm distally and 3.0mm proximally, with a minimal lumen area of 5.5–6.0 mm² at the ostial segment. The second LAD had a vessel reference diameter of 2.5 mm distally and 2.75 mm proximally. Pre-dilatation of the second LAD was performed using a SC balloon at nominal pressure. Vessel preparation of the first LAD was then performed using a non-compliant (NC) 2.0 × 10 mm balloon, followed by a scoring balloon(2.5 × 15 mm) inflated at high pressure. The lesion was adequately prepared with minimal recoil and a type B non–flow-limiting dissection observed indicating adequate vessel preparation before DCB angioplasty. Two drug-coated balloons were inflated in the first and second LAD at nominal pressure for 45 seconds each. Similar non–flow-limiting type B dissections were observed in both LADs, with minimal recoil. Final angiographic results were satisfactory showing TIMI 3 flow with no immediate complications. The patient remained asymptomatic and discharged well the following day.

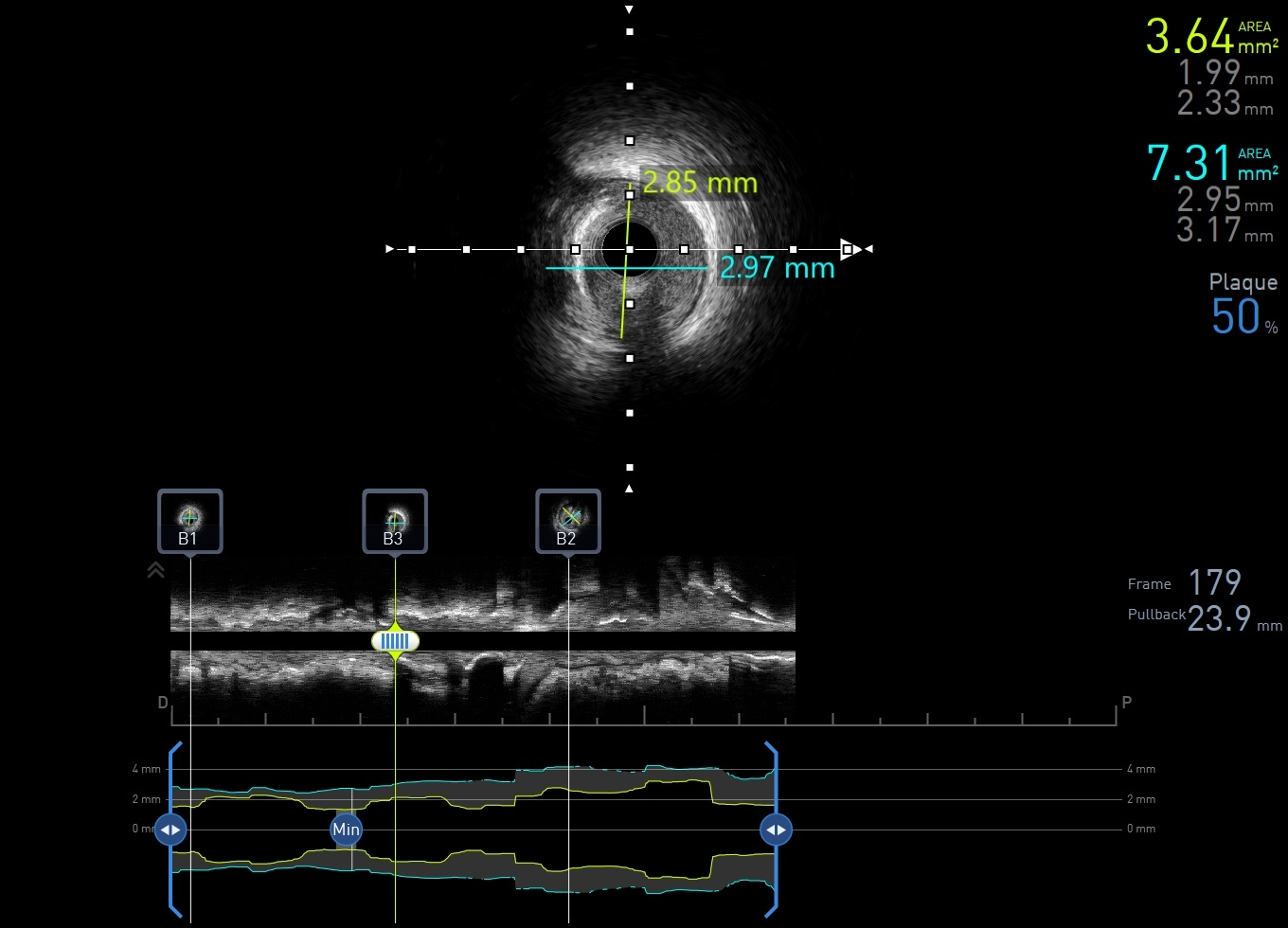
IVUS first LAD.mp4
Dual LAD post PCI.mp4
Case Summary
The favorable results achieved here reaffirm that with appropriate technique, imaging guidance and optimal lesion preparation, DCB-only PCI can serve as a viable and safe alternative to stenting even in anatomically complex scenarios such as dual LAD lesions with fibrocalcific disease. The absence of a permanent metallic scaffold preserves vessel physiology, reduces the risk of late stent thrombosis, and facilitates positive vascular remodeling over time. It reinforces the evolving paradigm shift toward stent-free revascularization in selected patients, particularly where dual vessel preservation and long-term vessel adaptability are desired.