Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_039
The One-Two Punch: Rota-Cut Strategy for Managing Napkin-Ring Calcified Lesion
By Rika Yandriani, Muhammad Syukri
Presenter
Rika Yandriani
Authors
Rika Yandriani1, Muhammad Syukri1
Affiliation
Dr M Djamil General Hospital, Indonesia1
View Study Report
CASE20251107_039
Coronary - Complex PCI - Calcified Lesion
The One-Two Punch: Rota-Cut Strategy for Managing Napkin-Ring Calcified Lesion
Rika Yandriani1, Muhammad Syukri1
Dr M Djamil General Hospital, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A60-year-old female, admitted from outpatient clinic with CCS class III stableangina pectoris for 1 month. Her cardiovascular risk factors were hypertensionand diabetes. This patient had a successful PCI at RCA and LCx 2 months beforeadmission. Her vital signs upon arrival were blood pressure of 140/80 mmHg andheart rate of 70 bpm. There were abnormal lung sounds and her peripheralperfusion was normal.
Relevant Test Results Prior to Catheterization
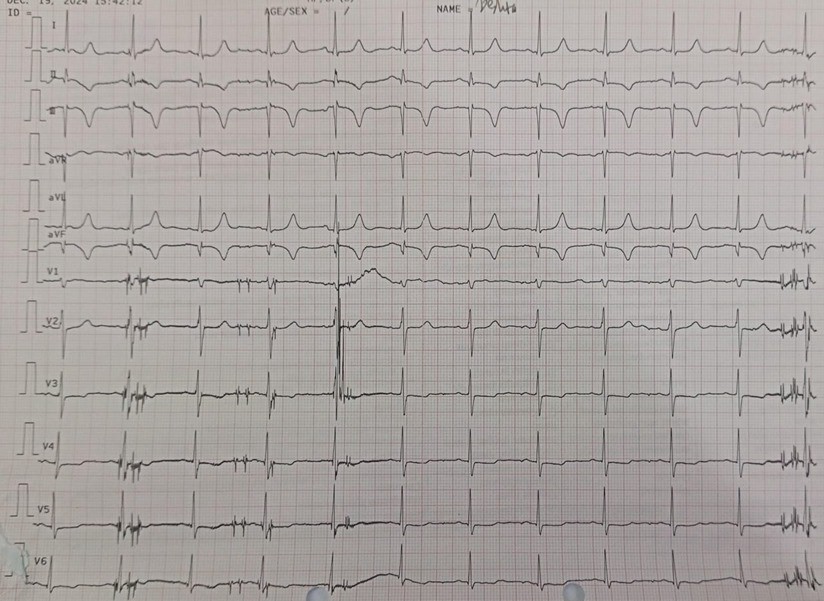
Her ECGshowed normal sinus rhytm with Q path and T inverted at inferior lead and Tinverted at anterior lead. Her echocardiography showed reduced LV systolicfunction with LV ejection fraction of 33%, hypokinetic at apicoinferior, hypokinetic atbasal-mid inferolateral, basal-mid inferoseptal, basal-mid anterolateral andapicoseptal. Her notable laboratory findings were fasting glucose levels of 180mg/dL and and serum creatinine 0,8 (eGFR 65 mL/min).
Relevant Catheterization Findings
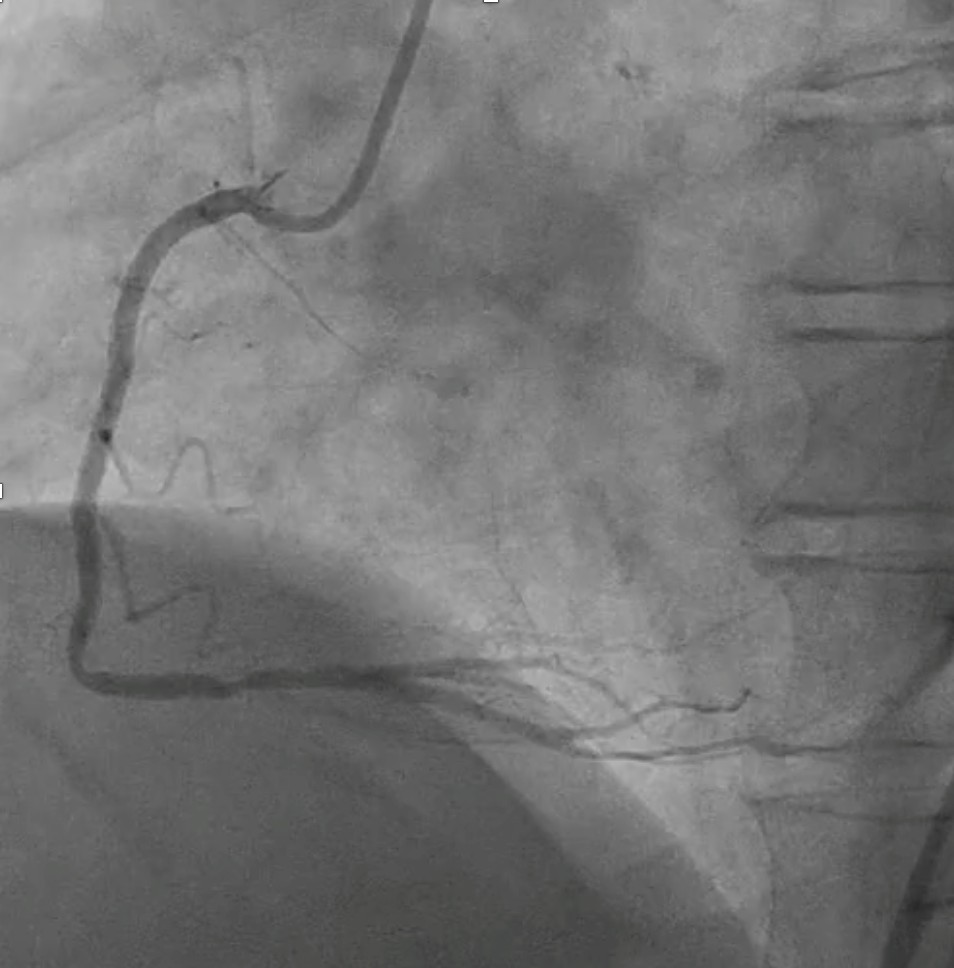
Initial angiography at our facility revealed patent stent at osteal to mid RCA.Left coronary angiography showed patent stent at proximal to distal LCx anddiffuse, severe and heavy calcified stenosis at proximal to distal LAD.


Interventional Management
Procedural Step
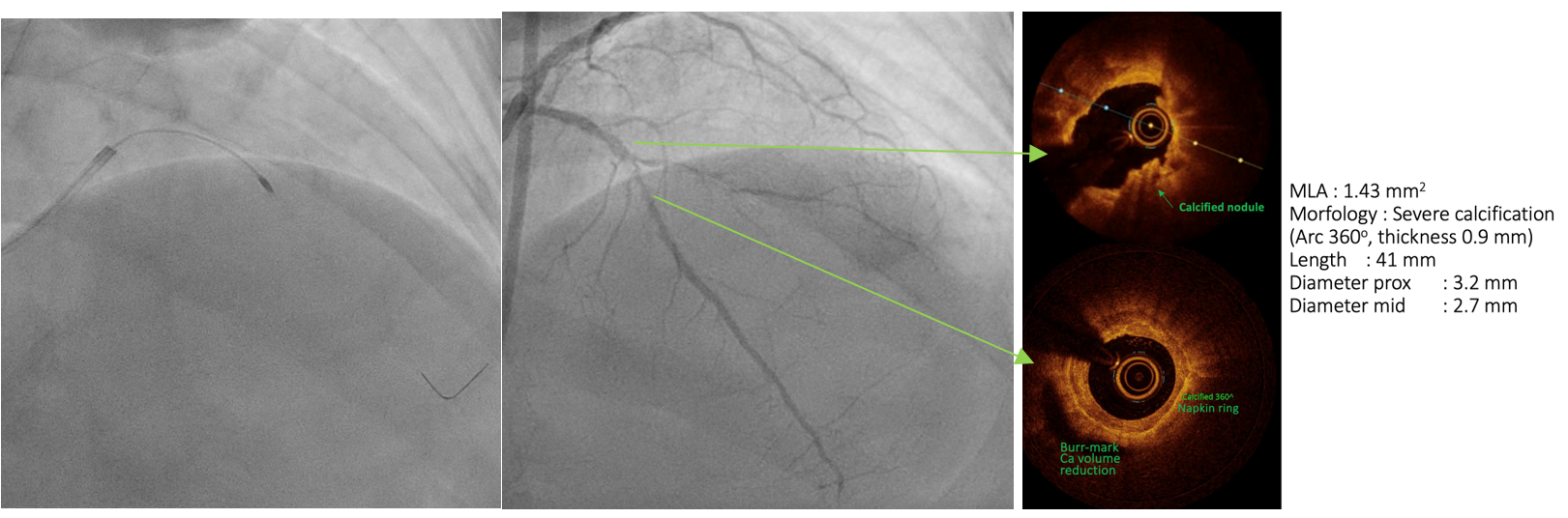
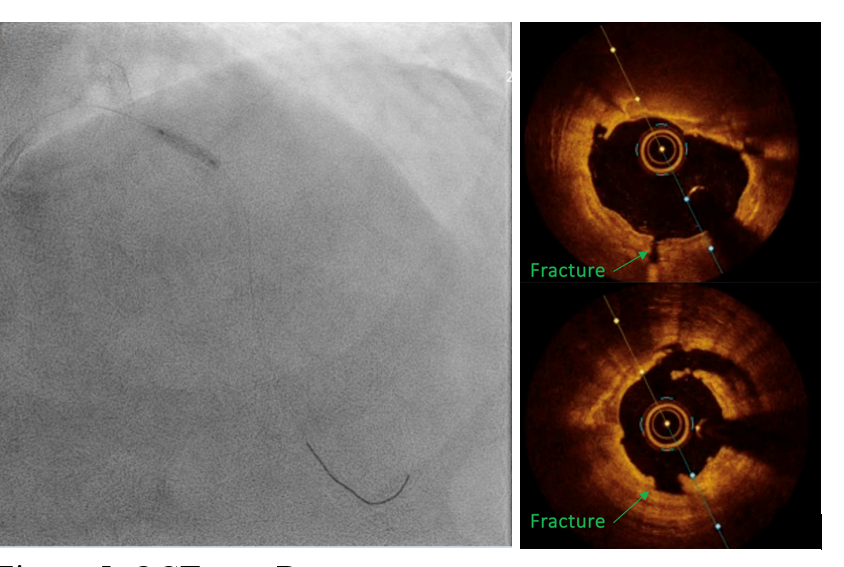
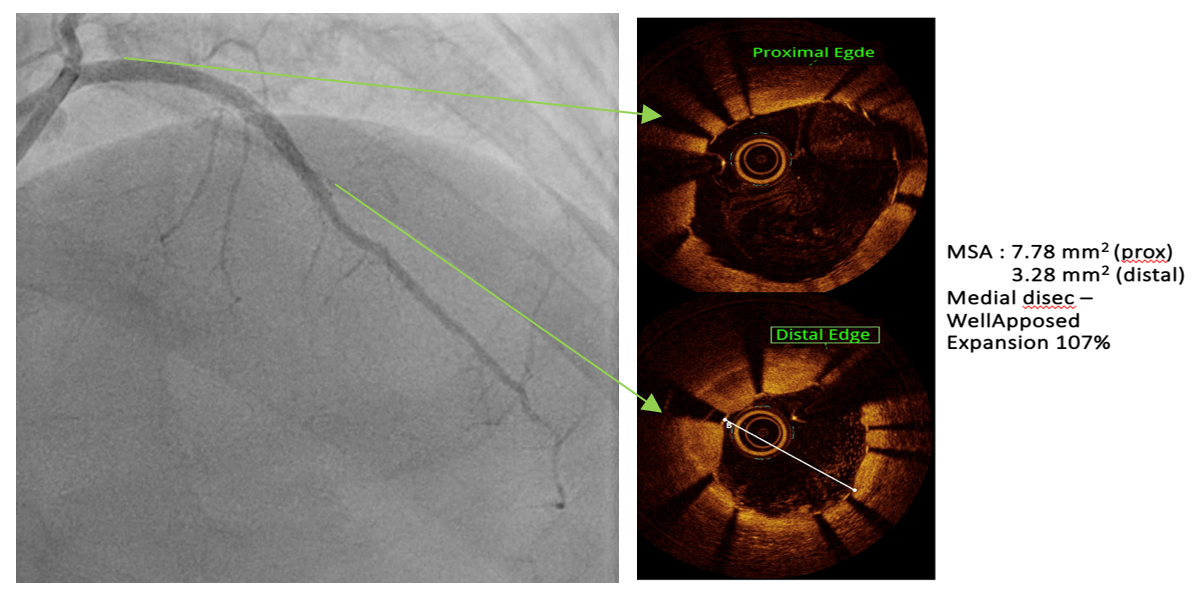
PCIof the LAD was performed via femoral access using a BL 3.5/7F guiding catheter.A Runthrough Hypercoat wire was advanced distally without difficulty. The OCTcatheter failed to cross the lesion, and a 2.5 × 15 mm scoring balloon couldnot pass the mid LAD. A microcatheter was inserted, and the wire was exchangedfor a Rotawire. Rotational atherectomy was performed using a 1.25 mm burr withshort, gentle pecking runs at 180,000 rpm, followed by upsizing to a 1.5 mmburr for three runs at 200,000 (2 times) and 160,000 rpm. The burr advancedsmoothly with improved tactile feedback, suggesting successful plaquemodification. The wire was exchanged back to a Runthrough, and OCT (DragonflyOPTIS) imaging showed an MLA of 1.43 mm² at mid LAD with severe 360° calcification(0.9 mm thick, 41 mm long) and a napkin-ring pattern. A 2.5 × 15 mm cuttingballoon was used with multiple 14–18 atm inflations, producing a visible“crack” in the calcified cap. Angiography and repeat OCT confirmed the calciumfracture. A 3.0 × 46 mm DES was deployed from the ostial to distal LAD at 14atm and post-dilated with a 3.5 mm NC balloon proximally. Final angiographyshowed TIMI 3 flow. OCT demonstrated excellent stent expansion (MSA 7.78 mm²proximal, 3.28 mm² distal) without dissection and with 107% stent expansion.
Case Summary
This case shows the Rota-Cut strategy transforms a high-risk, unpredictable intervention into a controlled and successful one on a severely calcified "napkin ring" coronary lesion that is resistant to standard balloon dilation. Rotational atherectomy will reduced the volume of calcific plaque and cutting balloon will cause calcium fracture to facilitate optimal stent expansion and apposition confirmed on intravascular imaging and prevent stent failure in the future.