Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_038
The Magic of Drug-Coated Balloon-Only Strategy in a Large Proximal LAD CTO: A Story of Simplicity Winning Over Complexity in a Case-Based Insight
By Doreen Sumpat, Wan Azman Wan Ahmad, Imran Zainal Abidin, Faiz Mashood
Presenter
Doreen Sumpat
Authors
Doreen Sumpat1, Wan Azman Wan Ahmad2, Imran Zainal Abidin2, Faiz Mashood2
Affiliation
Universiti Malaysia Sabah, Sabah, Malaysia1, Universiti Malaya Medical Centre, Universiti Malaya, Kuala Lumpur, Malaysia2
View Study Report
CASE20251107_038
Coronary - DES/BRS/DCB
The Magic of Drug-Coated Balloon-Only Strategy in a Large Proximal LAD CTO: A Story of Simplicity Winning Over Complexity in a Case-Based Insight
Doreen Sumpat1, Wan Azman Wan Ahmad2, Imran Zainal Abidin2, Faiz Mashood2
Universiti Malaysia Sabah, Sabah, Malaysia1, Universiti Malaya Medical Centre, Universiti Malaya, Kuala Lumpur, Malaysia2
Clinical Information
Relevant Clinical History and Physical Exam
A 45-year-old man with underlying diabetes mellitus, hypertension and dyslipidemia, was also diagnosed with retroviral disease (RVD) eight years ago, for which he has been on highly active antiretroviral therapy (HAART). He presented with left-sided, compressive chest pain radiating to left arm, which had persisted for two days prior to presentation. The pain was exertional in nature and worsened acutely early in the morning, awakening him from sleep. This prompted him to come to hospital.
Relevant Test Results Prior to Catheterization
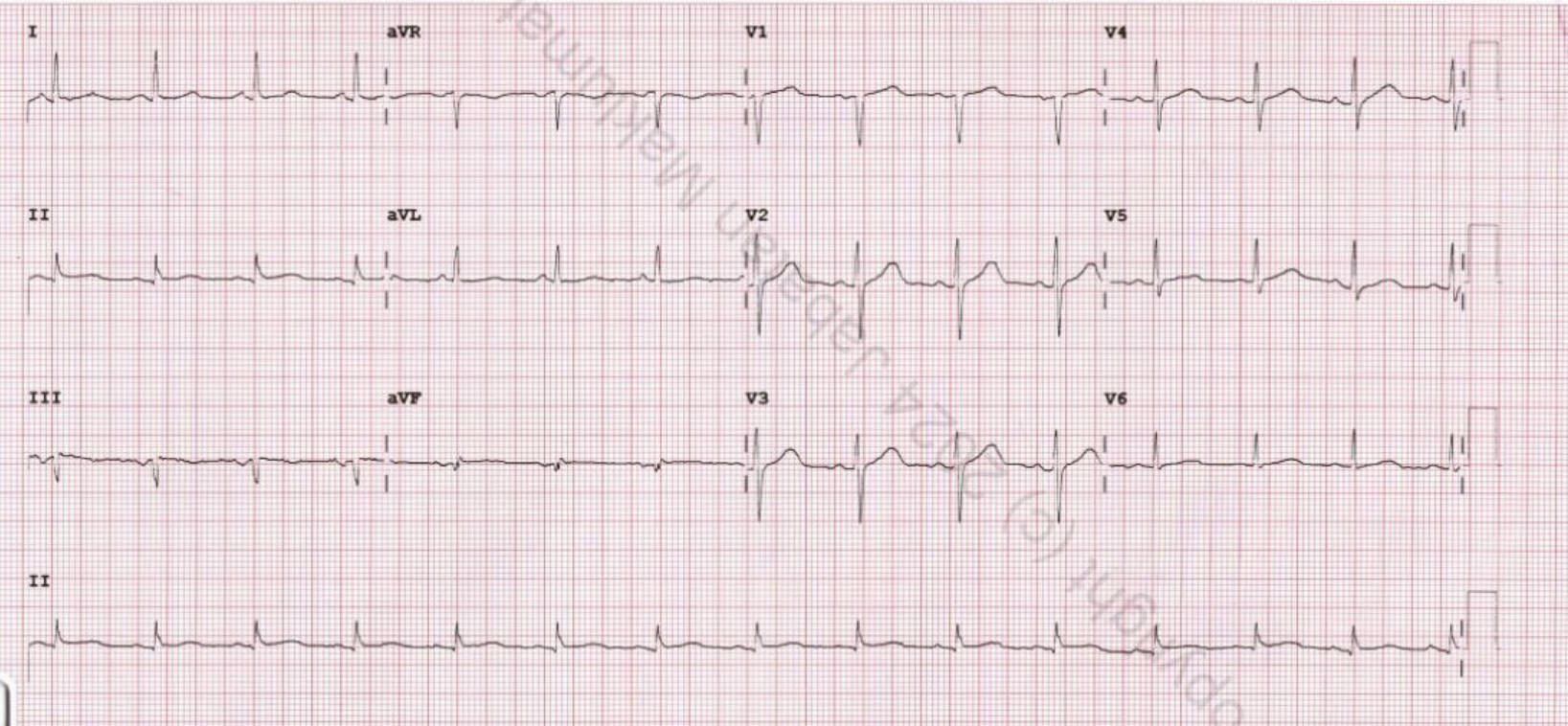
Serial ECG demonstrated Q waves in leads II, III, and V1 without dynamic ST-T changes. High-sensitivity troponin I was elevated at 132 ng/L on admission, rising markedly to 9,345 ng/L after 12 hours. Echocardiography revealed reduced LVEF of 40% with hypokinesia of mid anterior, mid anteroseptal, apical anterior, apical septal, and apical inferior segments, suggestive of LAD territory involvement. Glycemic control was suboptimal, due to poor adherence to medication.

 LAD 1 Diagnostic.mp4
LAD 1 Diagnostic.mp4
RCA Diagnostic.mp4
Relevant Catheterization Findings
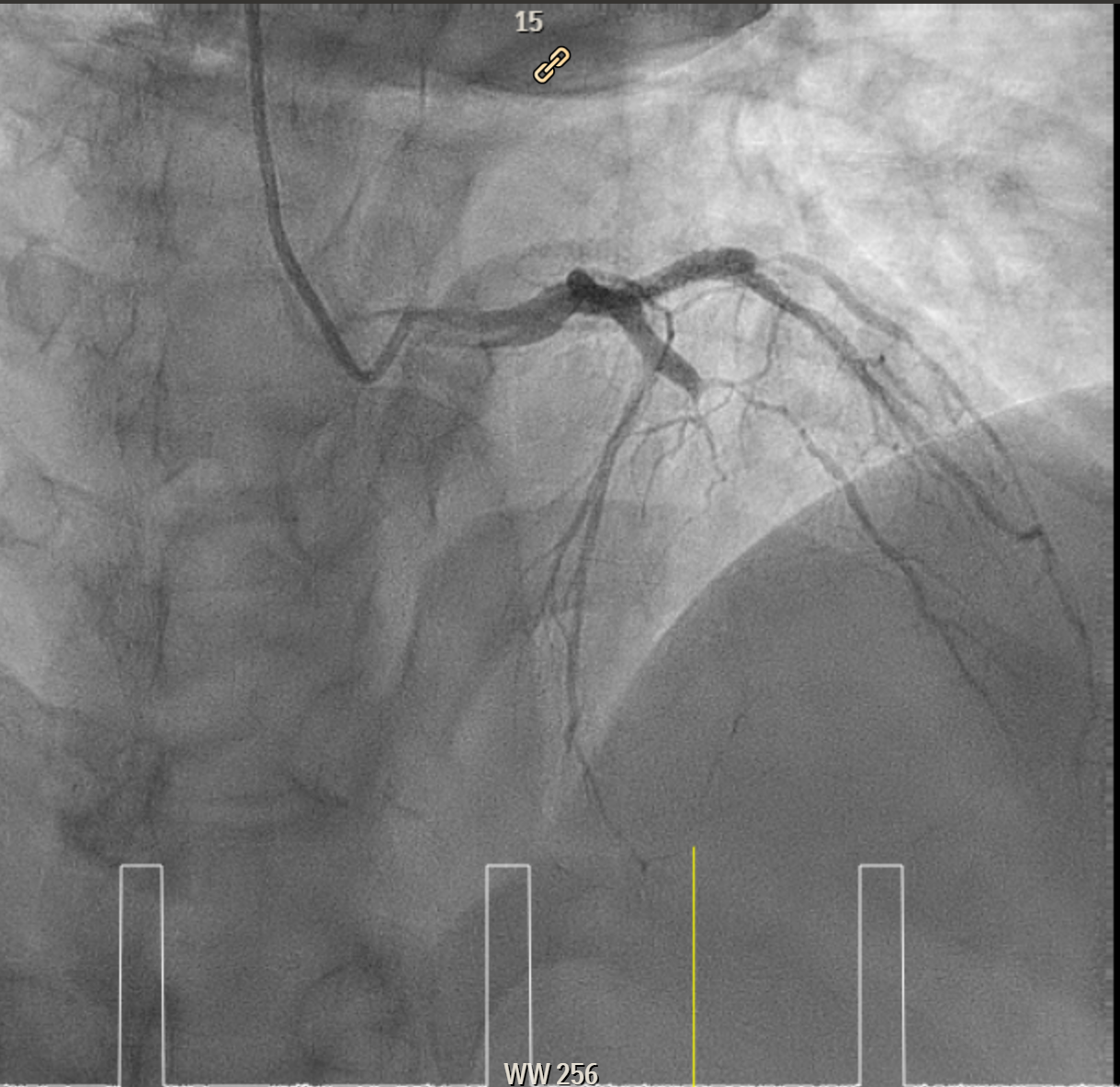
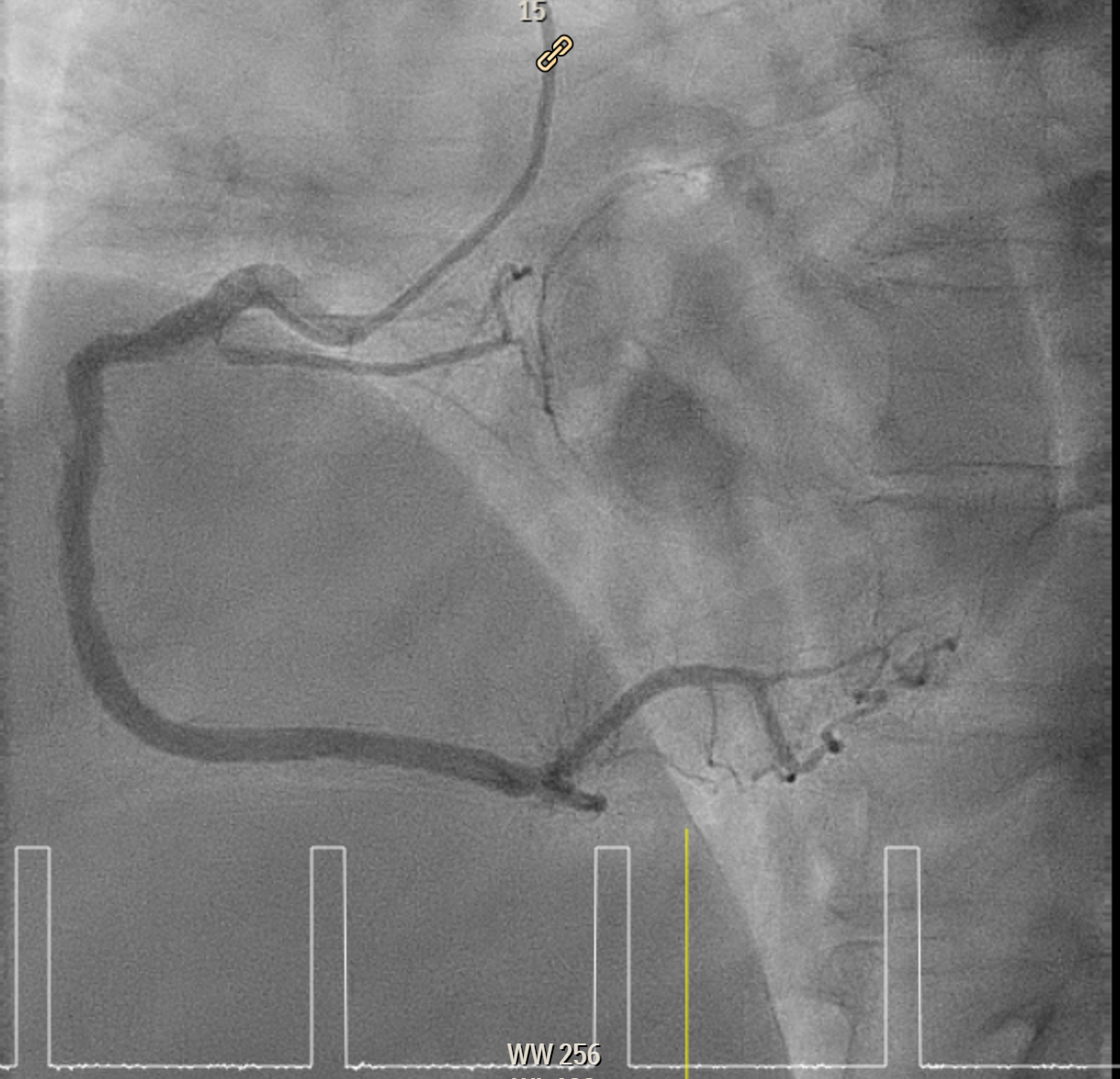
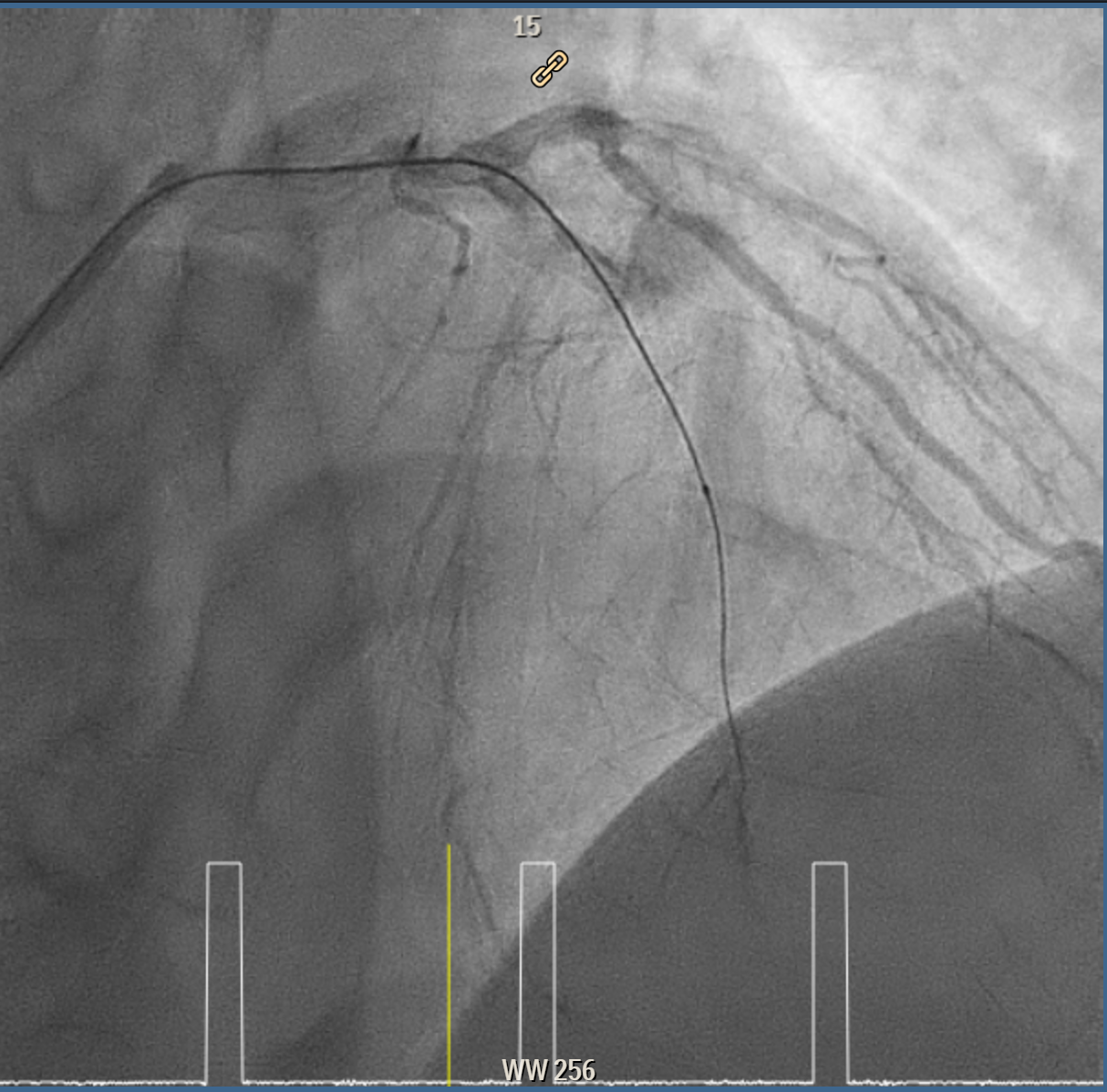
Elective angiogram was performed 3 months later as he declined procedure during index admission. Coronary angiogram showed total occlusion of proximal LAD at bifurcation of first diagonal and first septal branches. It received collateral supply from conus branch and first septal branch (Rentrop 2). J-CTO score was 2, and PROGRESS-CTO score was 1, indicate moderate complexity. Additionally, RCA was huge and dominant, while proximal first OM branch of LCX was 80–90% diseased.
LAD 2 Diagnostic.mp4
LCX 2 Diagnostic.mp4
RCA Diagnostic.mp4
Interventional Management
Procedural Step
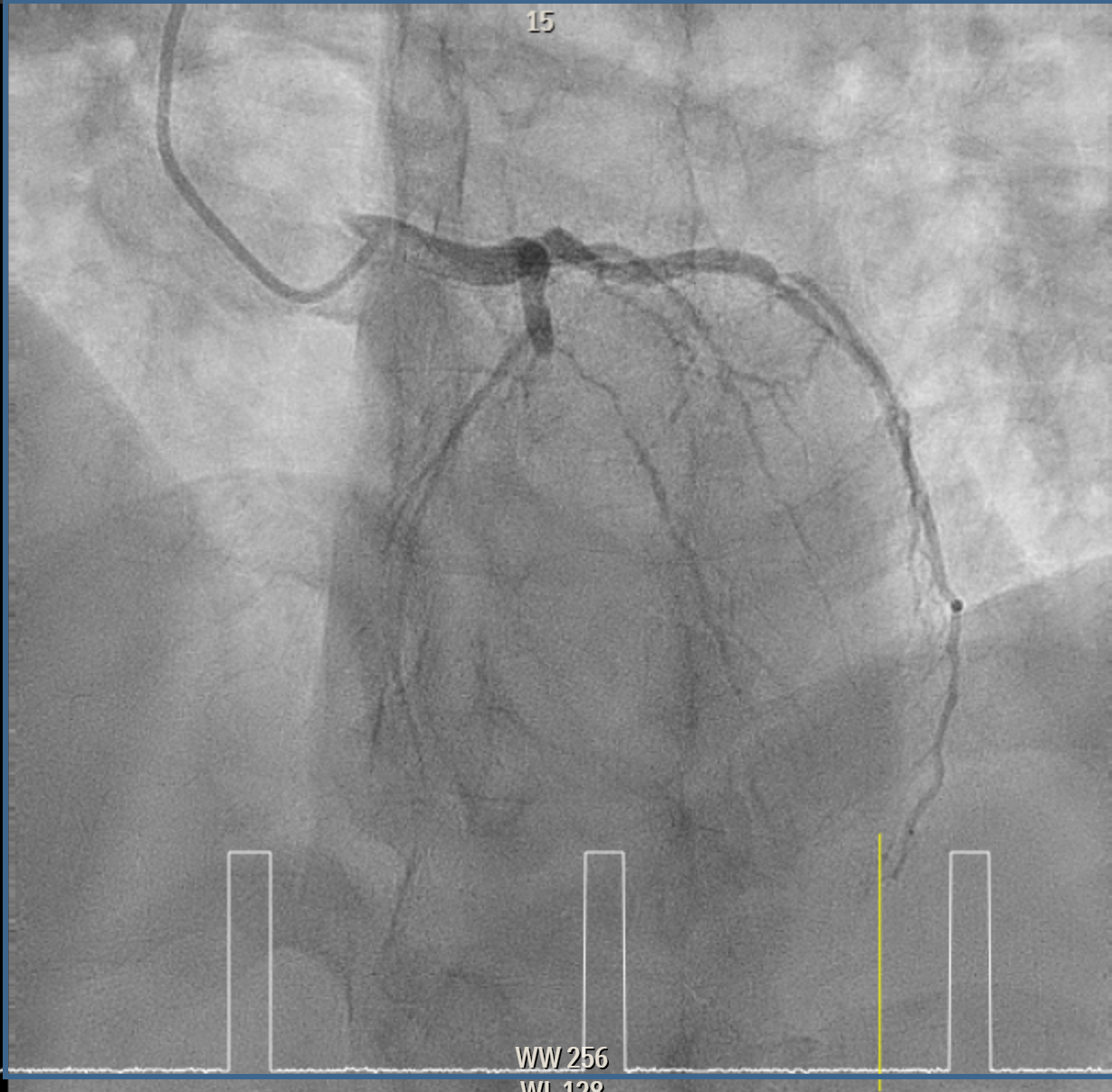
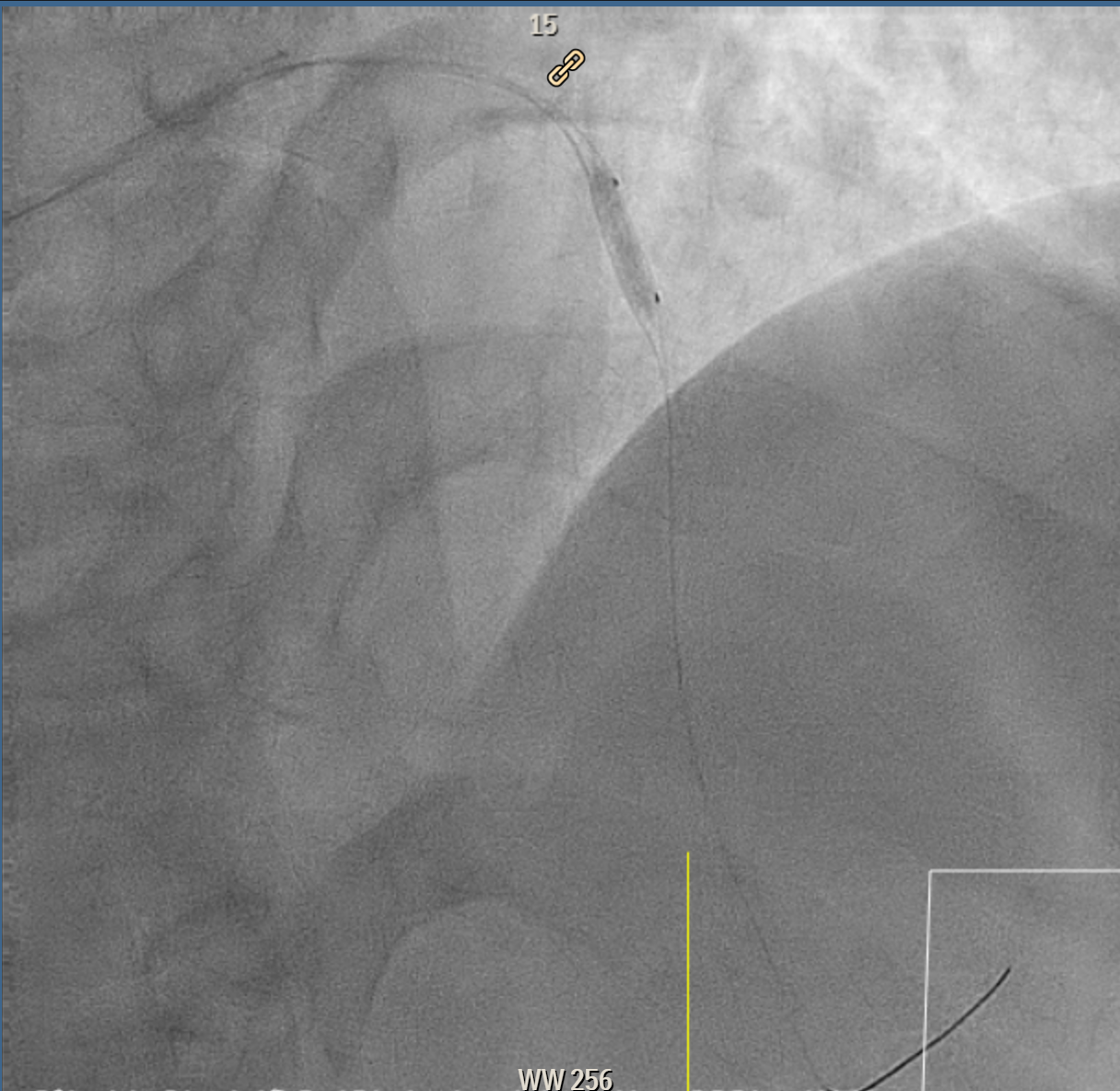
Coronary intervention was performed on a proximal LAD (pLAD) total occlusion via single right radial approach using 6F XB 3.5 guiding catheter. Initial antegrade attempts with RunThrough Floppy and Fielder-XT wires were unsuccessful due to buckling against the proximal cap. Wire strategy was escalated to Gaia Second wire with Finecross microcatheter support, allowing careful penetration of proximal cap and subsequent advancement through distal cap. True lumen position was confirmed with contrast injection through the microcatheter, and wire was then exchanged to a Fielder-XT wire to safely navigate to distal LAD (dLAD) and reduce risk of perforation. Lesion preparation was performed with stepwise predilatation, beginning with Sapphire 0.85 × 5 mm balloon at 10–12 atm in pLAD to dLAD. Further predilatation was performed with Sapphire 2.0 × 15 mm balloon at 12 atm from dLAD to mid LAD (mLAD) and higher pressure up to 16atm at pLAD. Despite multiple inflations, pLAD remained tight, prompting escalation with a Sapphire 2.5 × 15 mm balloon at up to 18 atm and Scoreflex NC 3.0 × 15 mm balloon at 8–12 atm to adequately prepare mildly calcified pLAD segment. Final predilatation achieved optimal luminal caliber. DCB was then performed, with m-dLAD treated using Magic Touch 2.25 × 35 mm and the p-mLAD treated with Magic Touch 3.0 × 40 mm. Both were deployed at 8 atm for 60 seconds. The procedure resulted in excellent luminal gain with no residual stenosis, recoil, or perforation.

LAD Predilate 1.mp4
Result Predilate 1.mp4
Post DCB Result.mp4
Case Summary
DCB angioplasty is a feasible strategy for pLAD CTO when meticulous technique and thorough lesion preparation are performed. Success depends on careful wire escalation, plaque modification, and adequate high-pressure predilatation to achieve optimal luminal gain and TIMI III flow without major dissection. DCB strategy restores vessel patency while avoiding permanent metal, minimise restenosis, preserve side branches and vasomotion, and maintain options for future PCI or CABG. It should be reserved for selected lesions and performed by experienced CTO operators, ideally guided by detailed angiographic evaluation and intravascular imaging to ensure procedural success and durability of results.