Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_036
A Case of Stent Mounting Balloon Rupture Resulting in Stent Underexpansion
By Keitaro Mizuta, Hirohiko Ando, Tetsuya Amano
Presenter
Keitaro Mizuta
Authors
Keitaro Mizuta1, Hirohiko Ando1, Tetsuya Amano1
Affiliation
Aichi Medical University, Japan1
View Study Report
CASE20251107_036
Coronary - Complication Management
A Case of Stent Mounting Balloon Rupture Resulting in Stent Underexpansion
Keitaro Mizuta1, Hirohiko Ando1, Tetsuya Amano1
Aichi Medical University, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
A 67-year-old woman with a history of myocardial infarction presented with recurrent angina. Physical examination and vital signs were stable. Electrocardiogram showed nonspecific ST-T changes. Laboratory tests revealed no elevation of cardiac enzymes. She was diagnosed with stable angina and scheduled for coronary angiography and possible PCI.
Relevant Test Results Prior to Catheterization
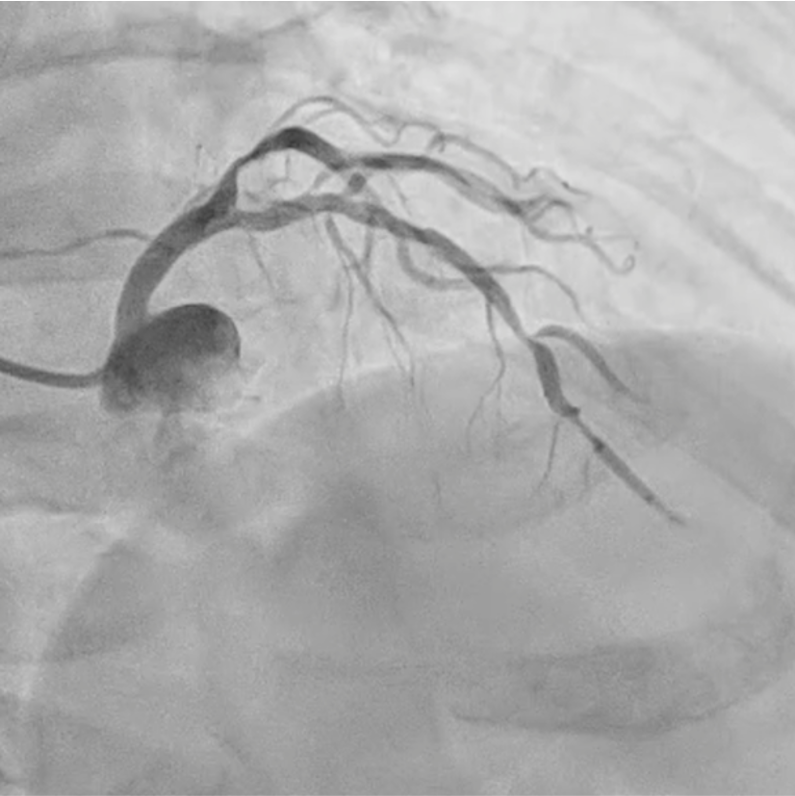
Coronary angiography and optical frequency domain imaging (OFDI) revealed a severe, focal, non-calcified stenosis in the mid-left anterior descending artery (LAD). Left ventricular systolic function was preserved without regional wall motion abnormalities.

Relevant Catheterization Findings
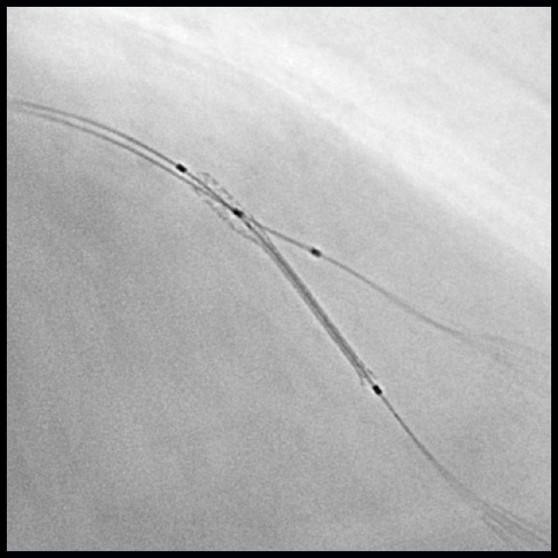
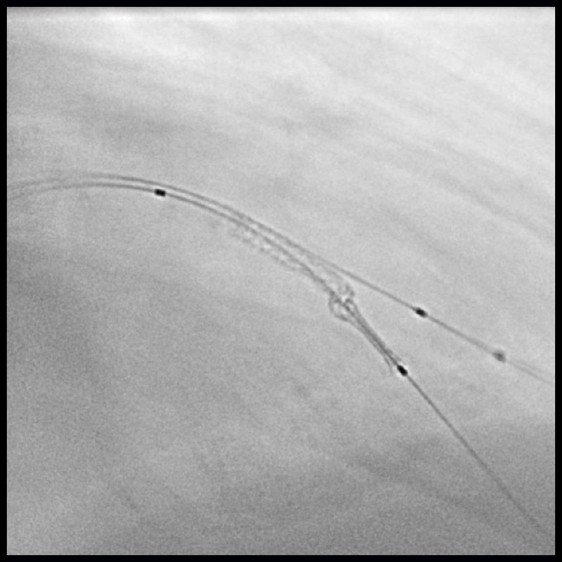
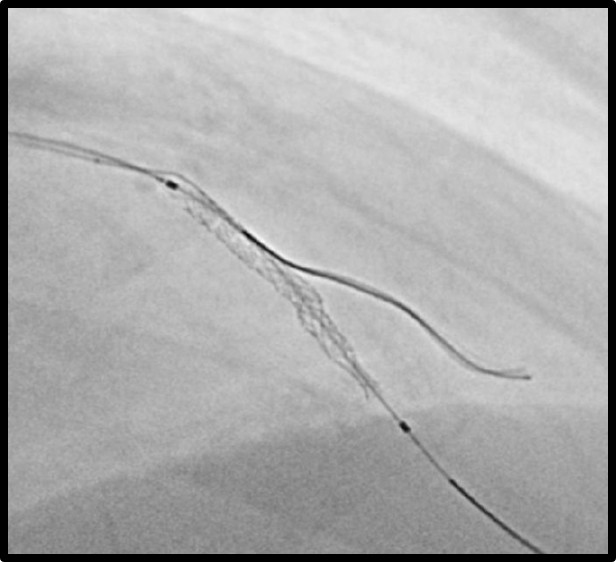
A 6 Fr guiding catheter was engaged in the left coronary ostium, and a 0.014-inch guidewire was advanced into the distal LAD. The first diagonal branch (D1) was protected by the jailed balloon technique, and direct stenting was performed. A drug-eluting stent was positioned at the target lesion; however, during balloon inflation, a pinhole rupture occurred in the stent-mounted balloon, resulting in incomplete expansion limited to the proximal segment.
Interventional Management
Procedural Step
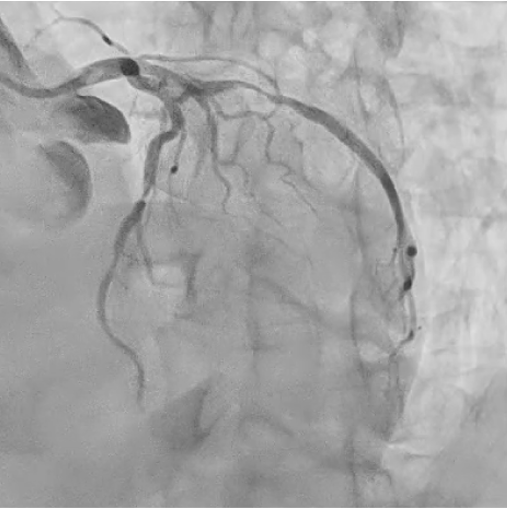
After the rupture, we replaced the inflator with one filled with undiluted contrast medium to improve pressure transmission. The balloon was then inflated at high pressure, which partially expanded the stent. Subsequently, we used a semi-compliant balloon for post-dilatation, achieving complete stent expansion without angiographic complications. Final angiography confirmed optimal stent deployment and TIMI 3 flow. The patient remained hemodynamically stable throughout the procedure and experienced no post-procedural complications.

Case Summary
This case illustrates incomplete stent expansion caused by a pinhole rupture of the stent-mounted balloon. Although using undiluted contrast medium and applying high pressure can facilitate expansion, this approach carries potential risks such as coronary dissection or intramural hematoma. Careful monitoring and stepwise escalation are essential to achieve successful outcomes.