Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_035
Contrastless, Not Clueless: Navigate Through Complex Lesion in Chronic Kidney Disease With Minimal Dye
By Dwisetyo Gusti Arilaksono, Arwin Saleh Mangkuanom, Nanda Iryuza, Amir Aziz Alkatiri, Doni Firman
Presenter
Dwisetyo Gusti Arilaksono
Authors
Dwisetyo Gusti Arilaksono1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Amir Aziz Alkatiri1, Doni Firman1
Affiliation
National Cardiovascular Center Harapan Kita, Indonesia1
View Study Report
CASE20251107_035
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Contrastless, Not Clueless: Navigate Through Complex Lesion in Chronic Kidney Disease With Minimal Dye
Dwisetyo Gusti Arilaksono1, Arwin Saleh Mangkuanom1, Nanda Iryuza1, Amir Aziz Alkatiri1, Doni Firman1
National Cardiovascular Center Harapan Kita, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 70-year old female was referred from regional general hospital with history of ST-elevated myocardial infarction 2 months prior. Currently, she complained chest discomfort during moderate daily activities. Comorbidities include hypertension, dyslipidemia, and chronic kidney disease. Physical examination findings were within normal limits.
Relevant Test Results Prior to Catheterization
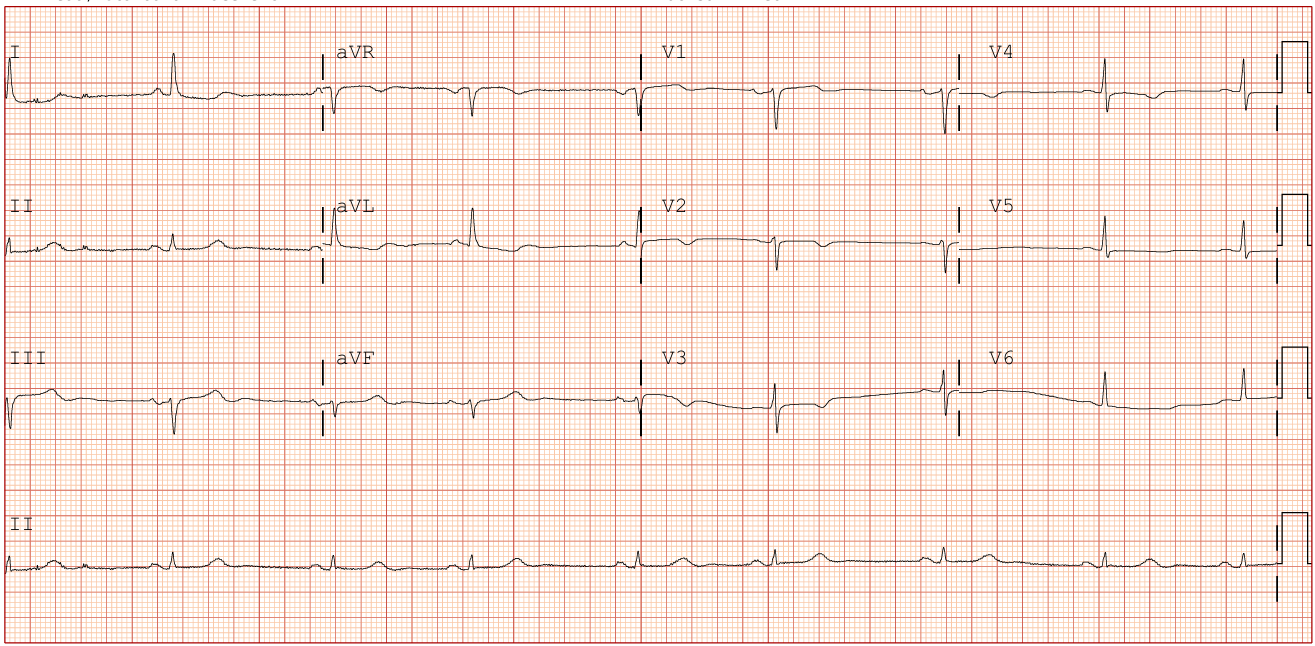
Resting ECG was sinus rhythm with T inverted at V2-V6 and I, aVL leads. Coronary angiography reports from previous hospital concluded CAD3VD. However, intervention was deferred. Lab results of anemia (Hb 9.8) and chronic renal insufficiency (Cr 2.80, eGFR 17) suggested patient’s vulnerability to both risk of bleeding and worsening renal function after PCI, which determined our strategy for the procedure.
Relevant Catheterization Findings
Dominant RCA with osteo-proximal tubular 70% stenosis; Normal LM; Diffuse LAD stenosis from ostial to distal with 90% stenosis at proximal; and tubular osteo-proximal 80% stenosis on LCx.
Interventional Management
Procedural Step
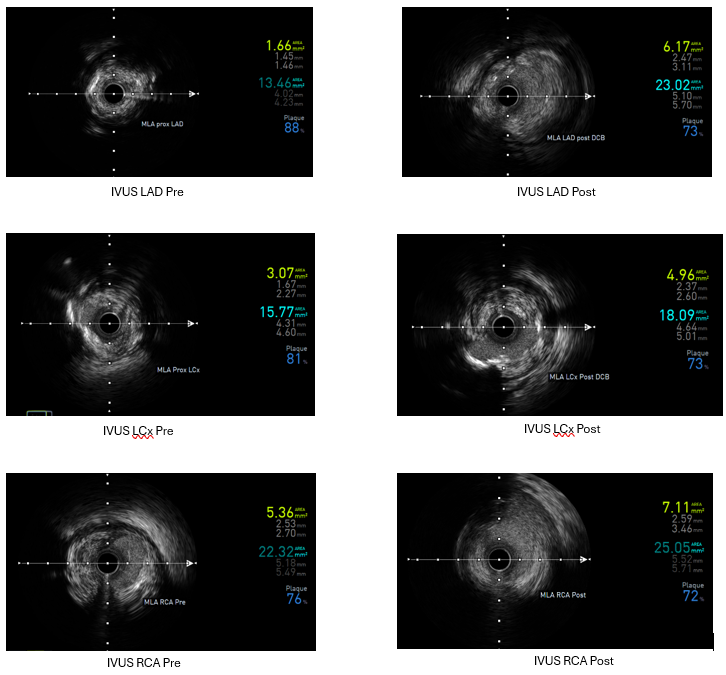
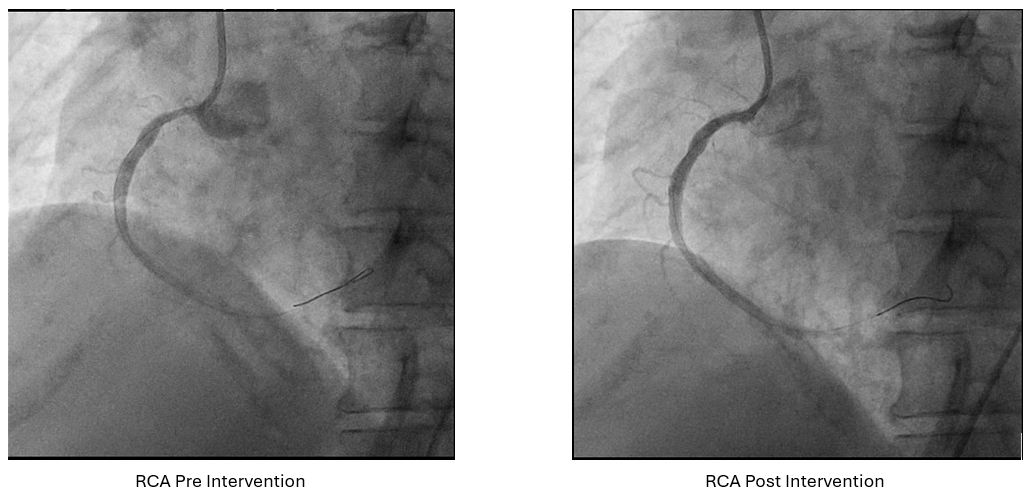
Angiography : LCA and RCA cannulation was confirmed by saline injection with ECG changes monitoring. 2 cc of contrast was pushed by 8 cc of saline for each view, with as minimal but optimal views as possible. Angiography roadmap was recorded. PCI LCA: Two workhorse wires was advanced to distal LAD and LCx using roadmap guidance. IVUS was inserted to evaluate morphology and length of LAD and LCx lesion as well as vessel size. The LAD IVUS results showed osteal-proximal fibrocalcified 90-180° with MLA of 1.66 mm2, while LCx IVUS also showed osteal-proximal fibrocalcified 180-270°with MLA of 3.07 mm2. Osteal-proximal LAD and LCX was then predilated with scoring balloon of 3.0x15 mm and 2.5x15 mm respectively, using guidewires as geometry guidance. IVUS evaluation suggested calcium crack, plaque dissection and lumen optimization. DCB 3.5x40 mm was then deployed at LM-LAD and DCB 3.0x40 mm at LM-LCx. One more view of low contrast angiography showed optimization of proximal LAD and LCx. IVUS evaluation showed MLA improvement from 1.66 to 6.17 mm2 (LAD) and 3.07 to 4.96 mm2(LCx). PCI RCA : Same approach was performed to RCA osteo-proximal lesion, predilatation using scoring balloon 4.0x12 mm followed by DCB 4.0x20 mm implantation, resulting with improvement in both angiography and IVUS evaluation (MLA improved from 5.36 to 7.11 mm2). Throughout of the procedure, only 18 cc of contrast were used.
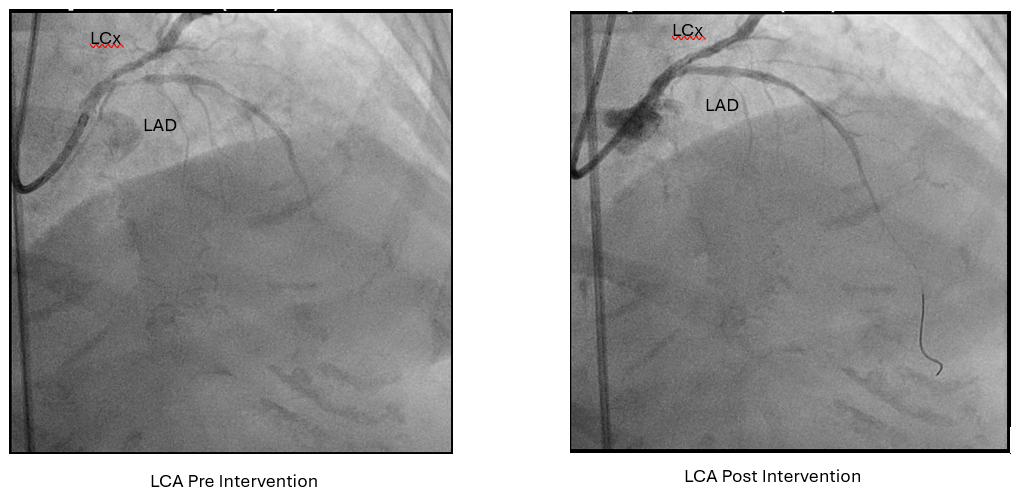
 LCA pre post.mp4
LCA pre post.mp4
RCA pre post.mp4
Case Summary
A high risk patient with renal insufficiency, high bleeding risk and old age, was referred for intervention to three-vessel CAD with osteo-proximal RCA, LAD and LCx lesions. Ultra low contrast approach was performed using combination of angiographic roadmaps, IVUS evaluation and guidewire marker to navigate the DCB implantation strategy to LAD, LCx and RCA. All target vessels reached acceptable lumen expansion and TIMI 3 flow without complications.