Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_034
From Hemodynamic Collapse to Recovery: Life-Saving TEVAR in Ruptured Type B Aortic Dissection Managed With a Hybrid Approach
By Rendra Mahardhika Putra, Johanes Eko Nugroho Putranto, Raden Mohammad Budiarto, Nadya Luthfah, Kevin Francio, Wynne Widiarti, Nadhifa Tanesha Aufazhafarin
Presenter
Rendra Mahardhika Putra
Authors
Rendra Mahardhika Putra1, Johanes Eko Nugroho Putranto1, Raden Mohammad Budiarto1, Nadya Luthfah1, Kevin Francio1, Wynne Widiarti2, Nadhifa Tanesha Aufazhafarin2
Affiliation
Department of Cardiology and Vascular Medicine, Dr. Soetomo General Academic Hospital, Surabaya, Indonesia1, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia2
View Study Report
CASE20251107_034
Endovascular - Thoracic & Abdominal Aortic Interventions
From Hemodynamic Collapse to Recovery: Life-Saving TEVAR in Ruptured Type B Aortic Dissection Managed With a Hybrid Approach
Rendra Mahardhika Putra1, Johanes Eko Nugroho Putranto1, Raden Mohammad Budiarto1, Nadya Luthfah1, Kevin Francio1, Wynne Widiarti2, Nadhifa Tanesha Aufazhafarin2
Department of Cardiology and Vascular Medicine, Dr. Soetomo General Academic Hospital, Surabaya, Indonesia1, Faculty of Medicine, Universitas Airlangga, Surabaya, Indonesia2
Clinical Information
Relevant Clinical History and Physical Exam
A 50-year-old man presented with sudden-onset chest pain and progressive dyspnea for one day. He appeared pale, hypotensive (78/57 mm Hg), and tachycardic (156 bpm). Breath sounds were markedly diminished over the left hemithorax. Echocardiography revealed a double lumen in the aortic arch with preserved left ventricular ejection fraction (35%) and no pericardial effusion.
Relevant Test Results Prior to Catheterization
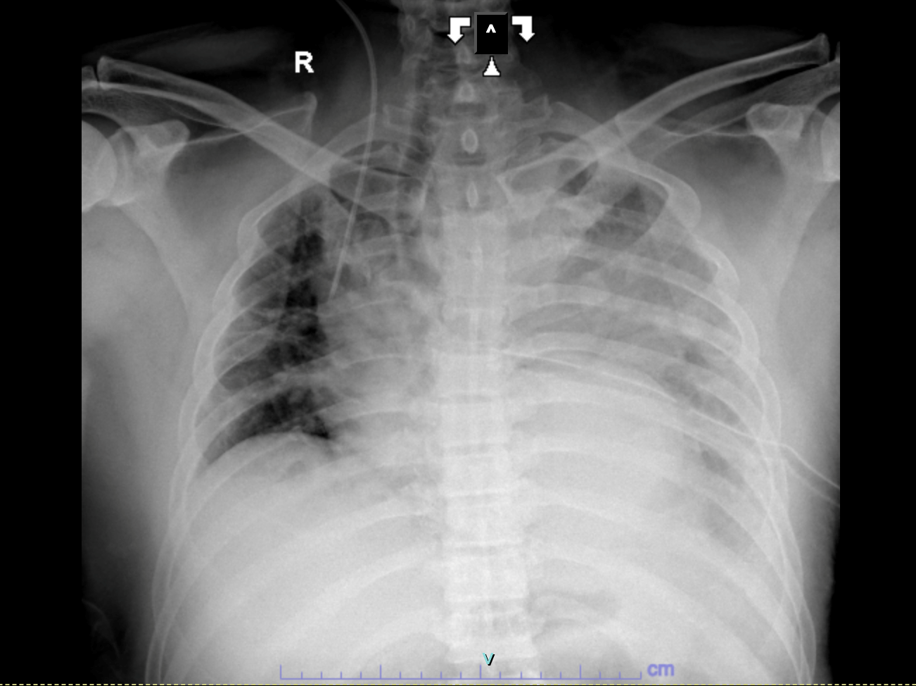
Chest X-ray showed total opacification of the left hemithorax with mediastinal shift. Non-contrast CT revealed a massive pleural collection obscuring the aortic contour, suggesting hematothorax. After stabilization and VATS decompression, CT angiography demonstrated a DeBakey type III (Stanford B) dissection from the arch to the left iliac artery with aneurysmal dilation and impending rupture distal to the left subclavian artery.
Relevant Catheterization Findings
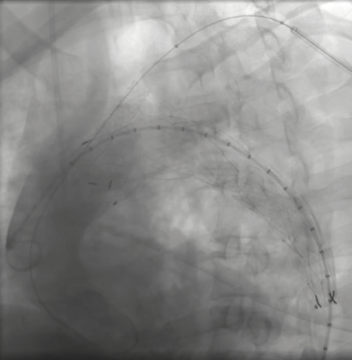
Aortography revealed a descending thoracic aortic dissection with an entry tear just distal to the left subclavian artery. Through right femoral access, a SEAL thoracic stent graft (38×150 mm) was deployed across the rupture site. A Bentley BeGraft chimney stent (10×57 mm) was placed via left brachial access to preserve subclavian perfusion. Final angiography confirmed proper stent apposition and complete exclusion of the rupture without endoleak.
Interventional Management
Procedural Step
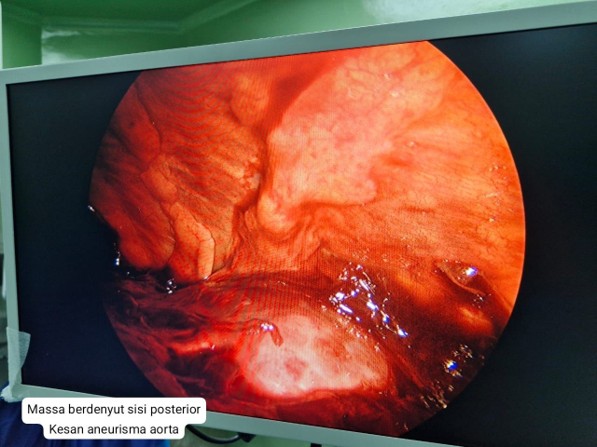
Step 1 – Emergency VATS (Video-Assisted Thoracoscopic Surgery):
Emergency VATS was performed by Cardiothoracic and Vascular Surgery (CTVS) for a massive left hemothorax of initially unknown origin. Approximately one liter of organized clot was evacuated, revealing a pulsatile posterior mediastinal hematoma that raised suspicion of an underlying aortic rupture. A 28 Fr chest tube was inserted, improving ventilation and stabilizing hemodynamics, which allowed subsequent imaging and preparation for definitive endovascular repair.Step 2 – TEVAR (Thoracic Endovascular Aortic Repair):
Following stabilization, a dual-access endovascular approach was performed under general anesthesia with ultrasound-guided puncture of the right femoral (22 Fr, pre-closed with two Proglides) and left brachial (7 Fr) arteries. After systemic heparinization (5,000 IU), aortography delineated an entry tear distal to the left subclavian artery. A SEAL Thoracic Stent Graft (38 × 150 mm) was precisely deployed across the rupture site, and a Bentley BeGraft Chimney Stent (10 × 57 mm) was inserted via the brachial route to maintain left subclavian perfusion. Completion angiography confirmed optimal stent apposition and full exclusion of the pseudoaneurysm without endoleak. Hemodynamics remained stable throughout, and MAP was maintained at 80 mmHg for 48 hours post-procedure. The intervention achieved complete sealing with no complications.

 CT Angio.mp4
CT Angio.mp4
Graft.mp4
Emergency VATS was performed by Cardiothoracic and Vascular Surgery (CTVS) for a massive left hemothorax of initially unknown origin. Approximately one liter of organized clot was evacuated, revealing a pulsatile posterior mediastinal hematoma that raised suspicion of an underlying aortic rupture. A 28 Fr chest tube was inserted, improving ventilation and stabilizing hemodynamics, which allowed subsequent imaging and preparation for definitive endovascular repair.Step 2 – TEVAR (Thoracic Endovascular Aortic Repair):
Following stabilization, a dual-access endovascular approach was performed under general anesthesia with ultrasound-guided puncture of the right femoral (22 Fr, pre-closed with two Proglides) and left brachial (7 Fr) arteries. After systemic heparinization (5,000 IU), aortography delineated an entry tear distal to the left subclavian artery. A SEAL Thoracic Stent Graft (38 × 150 mm) was precisely deployed across the rupture site, and a Bentley BeGraft Chimney Stent (10 × 57 mm) was inserted via the brachial route to maintain left subclavian perfusion. Completion angiography confirmed optimal stent apposition and full exclusion of the pseudoaneurysm without endoleak. Hemodynamics remained stable throughout, and MAP was maintained at 80 mmHg for 48 hours post-procedure. The intervention achieved complete sealing with no complications.
Case Summary
This case demonstrates a successful staged hybrid strategy combining VATS for decompression and TEVAR for definitive repair in ruptured type B aortic dissection with massive hematothorax. The sequence allowed diagnostic clarification, respiratory stabilization, and safe endovascular sealing. The patient achieved full recovery, underscoring the value of multidisciplinary coordination in complex aortic emergencies.