Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_033
Dancing Through the Curves: Percutaneous Coronary Intervention in Tortuosity Calcified Coronary Lesion
By Agung Rizka Pratama, Muhammad Syukri
Presenter
Agung Rizka Pratama
Authors
Agung Rizka Pratama1, Muhammad Syukri1
Affiliation
Dr M Djamil General Hospital, Indonesia1
View Study Report
CASE20251107_033
Coronary - Complex PCI - Calcified Lesion
Dancing Through the Curves: Percutaneous Coronary Intervention in Tortuosity Calcified Coronary Lesion
Agung Rizka Pratama1, Muhammad Syukri1
Dr M Djamil General Hospital, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 64-year-old male, admitted fromoutpatient clinic with CCS class III, patient had history chest pain since 2weeks ago, his cardiovascular risk factors were smoker. Patient had succesfullperfomed for percutaneous coronary intervention 2 months ago in left circumflexand incomplete in left anterior descending vessel, the LAD are tortuous withcalcified lession. The vital signs were blood pressure of 136/60 mmHg, heart rate of 74 beats perminutes, There were no abnormal lung and heart sounds.
Relevant Test Results Prior to Catheterization
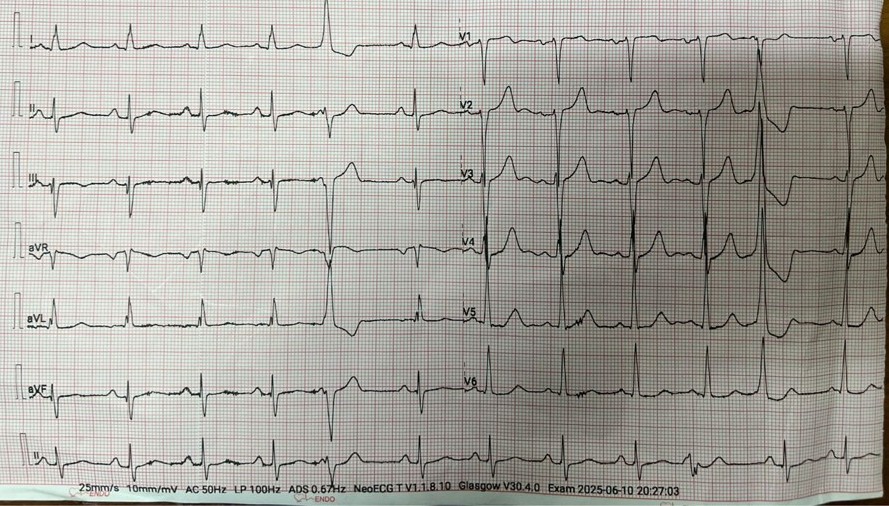
His ECG showed normal sinus rhytmwith poor R wave progression in anterior lead . Before procedure 2 months agothe echocardiography showed reduced LV systolic function with LV ejectionfraction of 32%, recently the ejection fraction was increased to be 46% withregional wall motion abnormalities in LAD teritory. His notable laboratoryfindings were random blood glucose levels of 105 mg/dL, LdL cholesterol 134mg/dL, Creatinine 1.0 mg/dL
Relevant Catheterization Findings
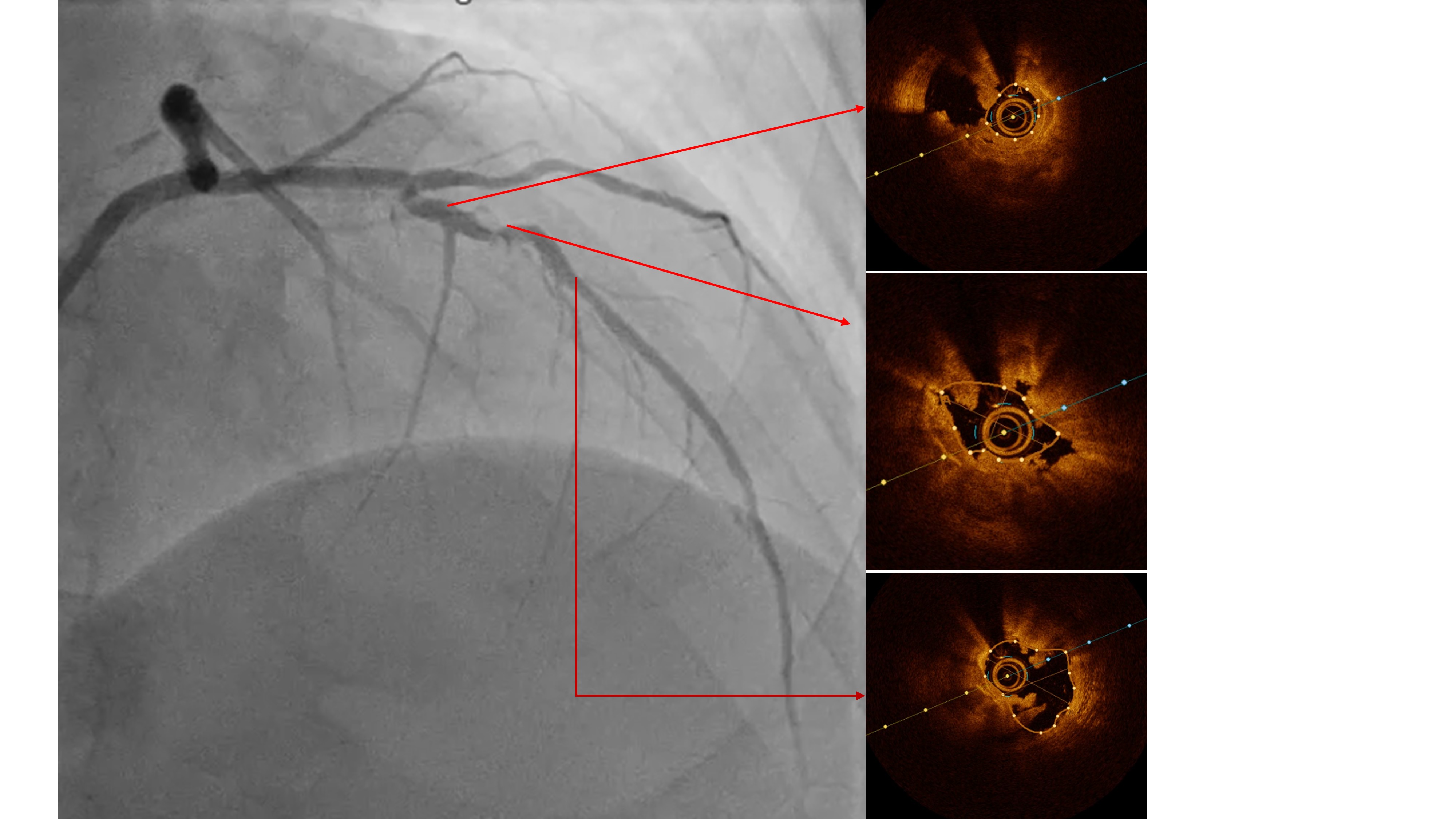
Coronary angiography examinationresults, we found patient with severe stenosis in proximal-mid LAD with tortuous andradiopacities seen before contrast injection in the arterial wall (tram-trackappearance) looks like calcifed lession and patent stent from Left main to LCx, non signifikan lession in right coronary artery.


Interventional Management
Procedural Step
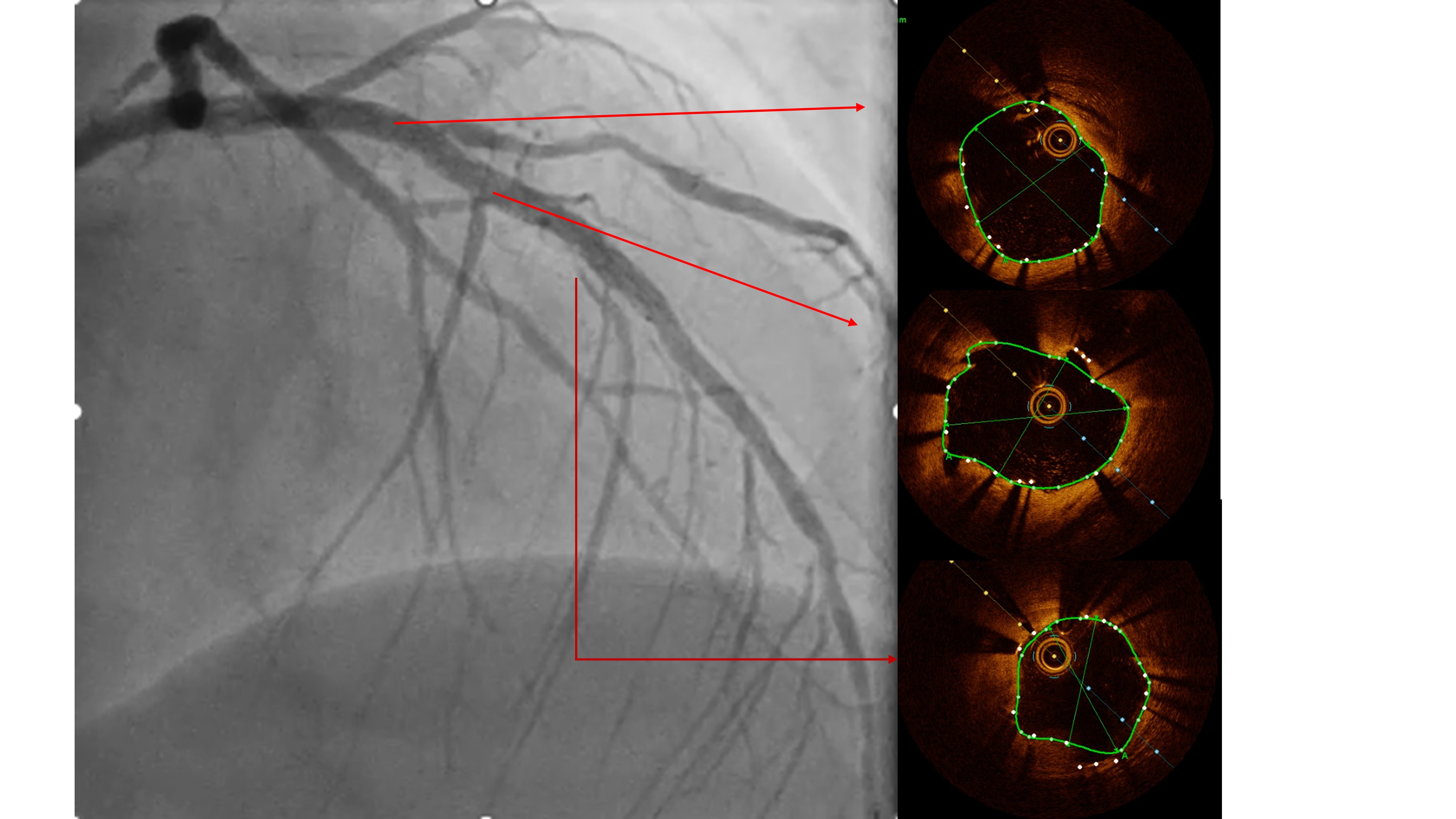
Two months ago, PCI of the LAD wasattempted. The guidewire successfully crossed to the distal LAD, but a 2.5 mmscoring balloon could not cross the mid lesion and showed a “dog-bone”appearance upon inflation, so the procedure was stopped, and PCI of the LCx wasperformed instead. We reattempted PCI of the LAD using a Mach CLS 7 Fr guidingcatheter. A Fielder XT wire crossed to the distal LAD, but the OCT cathetercould not cross the lesion. Lesion preparation with a 2.0 mm scoring balloon athigh pressure and a 2.0 mm Wolverine cutting balloon enabled OCT passage. OCTimaging revealed fibrous and nodular calcification in the mid LAD, with aminimal lumen area of 1.71 mm and reference diameters of 4.0 mm (proximal) and3.3 mm (distal). Orbital atherectomy using a Diamondback 360 (1.25 mm crown)was performed carefully due to vessel tortuosity, with 10 runs at80,000–120,000 rpm. Post-atherectomy OCT showed reduced calcium burden andincreased lumen area. Further lesion preparation with 2.5 and 2.75 mm scoringballoons showed no “dog-bone” sign, indicating adequate calcium fracture. A 3.0× 46 mm Amphilimus DES was implanted in the proximal–mid LAD and post-dilatedwith a 3.5 mm NC balloon. Final angiography showed TIMI 3 flow withoutdissection. Post-stent OCT showed good apposition, MSA 8.84 mm² proximally and5.73 mm² distally, with 99% expansion. The patient remained hemodynamicallystable and was discharged the following day.

Case Summary
This case demonstrates thecomplexity and challenges of percutaneous coronary intervention in a patientwith a severely tortuous and heavily calcified. Orbital atherectomy provedeffective in treating a severely tortuous and heavily calcified coronary lesionthat was initially uncrossable with a balloon. The technique enabled successfulplaque modification and improved vessel compliance, facilitating optimal stentdelivery. Optical coherence tomography guided the procedure by assessing calcium burden or nodul calcified and confirming adequate calcium fracture, luminal gain andstent expansion, resulting in a safe and successful revascularization.