Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_032
Recovery of the Stolen Pulse: Successful IVUS-Guided Drug-Coated Balloon Angioplasty for Subclavian Steal Syndrome – 6 Months Follow-Up
By Achmad Hafiedz Azis Kartamihardja, Salma Raudhatusabrina Basuki, Syarief Hidayat
Presenter
Achmad Hafiedz Azis Kartamihardja
Authors
Achmad Hafiedz Azis Kartamihardja1, Salma Raudhatusabrina Basuki2, Syarief Hidayat1
Affiliation
Hasan Sadikin General Hospital, Indonesia1, Melinda Cardio Vascular Center, Indonesia2
View Study Report
CASE20251107_032
Endovascular - Other Endovascular Interventions
Recovery of the Stolen Pulse: Successful IVUS-Guided Drug-Coated Balloon Angioplasty for Subclavian Steal Syndrome – 6 Months Follow-Up
Achmad Hafiedz Azis Kartamihardja1, Salma Raudhatusabrina Basuki2, Syarief Hidayat1
Hasan Sadikin General Hospital, Indonesia1, Melinda Cardio Vascular Center, Indonesia2
Clinical Information
Relevant Clinical History and Physical Exam
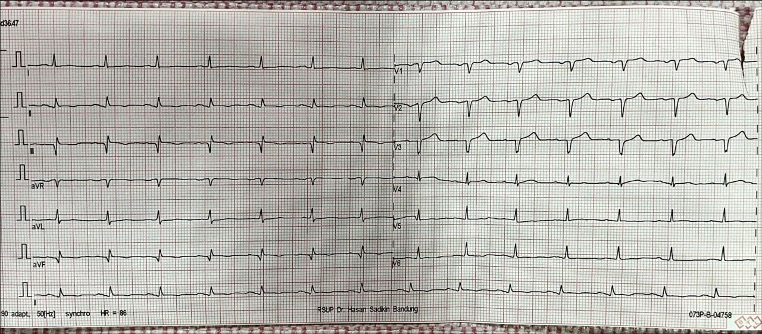
A 53 year old male was admitted to the hospital with claudication and weakness in left arm since 1 year ago. He also experienced couple episodes of unexplained dizziness. The patient was an active smoker with a known history of type 2 diabetes mellitus and hypertension. On physical examination, blood pressure at the left and right arm was 90/60 mmHg and 140/80 mmHg respectively. Brachial, radial, and ulnar pulses were faintly palpable. Neurological exam was unremarkable. ECG showed old MI inferior
Relevant Test Results Prior to Catheterization
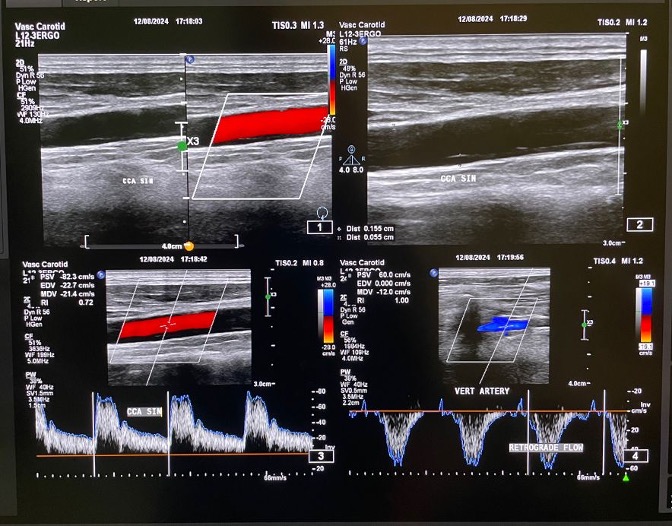
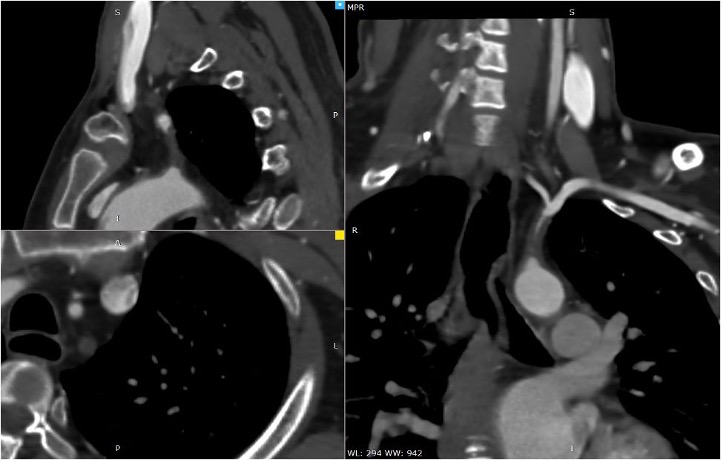
Duplex ultrasonography showed monophasic waveform in the left axillary, brachial, radial, and ulnar arteries. Retrograde flow was observed at the left vertebral artery, findings consistent with left subclavian steal syndrome. Computed Tomography Angiography (CTA) showed non calcified plaque with total occlusion from ostial left subclavian artery up to just before the origin of vertebral artery, with a tapered distal segment, and approximately 25–26 mm in length.

 CTA.mp4
CTA.mp4
Relevant Catheterization Findings
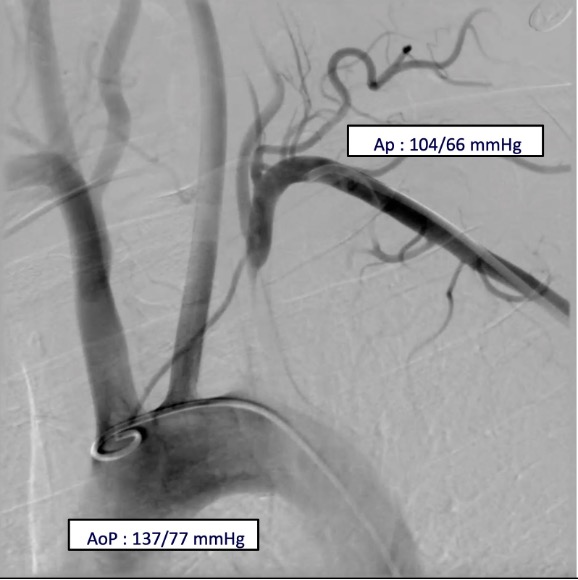
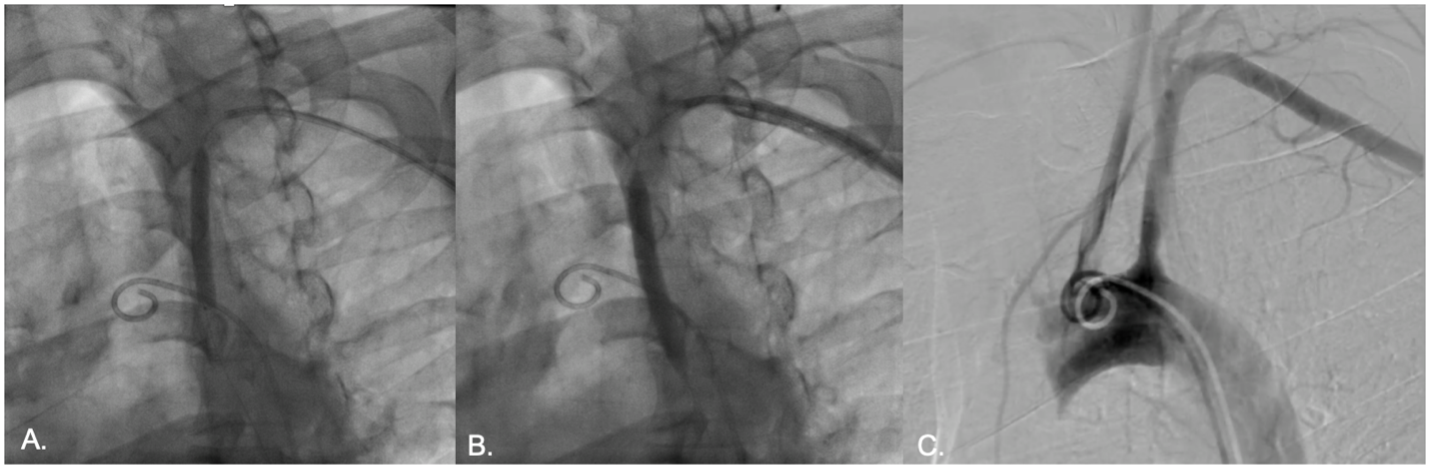
Vascular access was obtained via ultrasound-guided puncture of the left femoral and radial arteries. A 7 Fr radial GlideSheath and a 6 Fr femoral sheath were inserted. Double contrast injection using 5Fr pigtail in the aortic arch and JR 7Fr in the mid left subclavian atery, demonstrated total occlusion of the proximal left subclavian artery with retrograde flow in the left vertebral artery. The aortic pressure was 137/77 mmHg while the left subclavian artery was 104/66 mmHg.
diagnostic.mp4
Interventional Management
Procedural Step
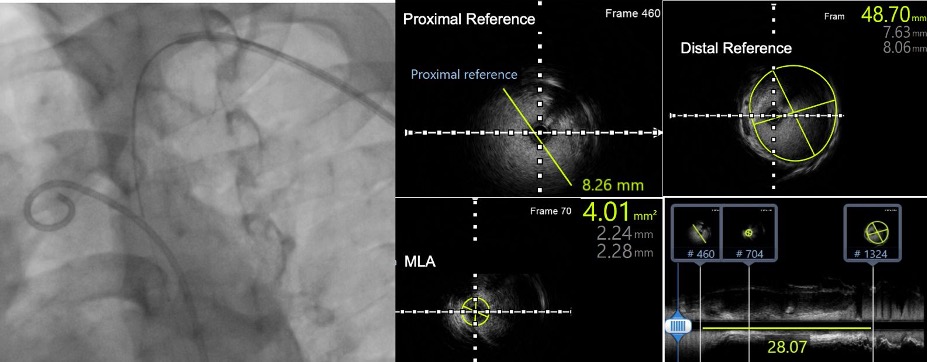
The lesion was crossed using a 0.014-inch guidewire via a retrograde approach from the left subclavian artery. An intravascular ultrasound (IVUS) catheter was advanced, and IVUS evaluation revealed a fibrolipidic plaque with a dominant fibrotic component. The minimal lumen area (MLA) measured 4.01 mm², and the lesion length was 28 mm. The distal vessel diameter ranged from 7.63 to 8.06 mm. Slow and gradual predilation was performed using a 4.0 x 60 mm non-compliant balloon at the proximal segment of the subclavian artery. Subsequent IVUS evaluation demonstrated an eccentric plaque with limited plaque dissection, without evidence of medial dissection or intramural hematoma (IMH). The post-dilation MLA was 22.35 mm² with a diameter of 5.06–5.63 mm. A 7.0 x 60 mm drug-coated balloon (low-dose paclitaxel) was then inflated at the proximal subclavian artery for 180 seconds. Final angiographic evaluation showed minimal residual stenosis without evidence of vessel perforation or dissection. The left vertebral artery remained patent with antegrade flow. No significant pressure gradient was noted between the aorta and the left subclavian artery. At six-month angiographic follow-up, the left subclavian artery remained patent with good antegrade flow.

pre ivus evaluation.mp4
final angiography evaluation.mp4
6 mo angiography evaluation.mp4
Case Summary
This case illustrates the successful IVUS-guided drug-coated balloon angioplasty in treating subclavian steal syndrome caused by total occlusion of the proximal left subclavian artery. IVUS provided precise lesion characterization, accurate vessel sizing, and ensured optimal plaque modification. The use of a drug-coated balloon enabled effective luminal gain while minimizing restenosis risk without the need for stent implantation. The procedure achieved full vessel recanalization without complications. At six-month follow-up, angiography confirmed sustained patency, highlighting the safety and long-term efficacy of this endovascular approach.