Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_029
Double Jeopardy: Fixing Late Restenosis of a Hybrid LM Bifurcation PCI With Intravascular Lithotripsy and Hybrid DCB and Stenting Complicated by Abluminal Wiring Causing a Double Lumen Stented LM
By Antonio Emmanuel Recto
Presenter
Antonio Emmanuel Recto
Authors
Antonio Emmanuel Recto1
Affiliation
The Medical City, Philippines1
View Study Report
CASE20251107_029
Coronary - Complex PCI - Bifurcation
Double Jeopardy: Fixing Late Restenosis of a Hybrid LM Bifurcation PCI With Intravascular Lithotripsy and Hybrid DCB and Stenting Complicated by Abluminal Wiring Causing a Double Lumen Stented LM
Antonio Emmanuel Recto1
The Medical City, Philippines1
Clinical Information
Relevant Clinical History and Physical Exam
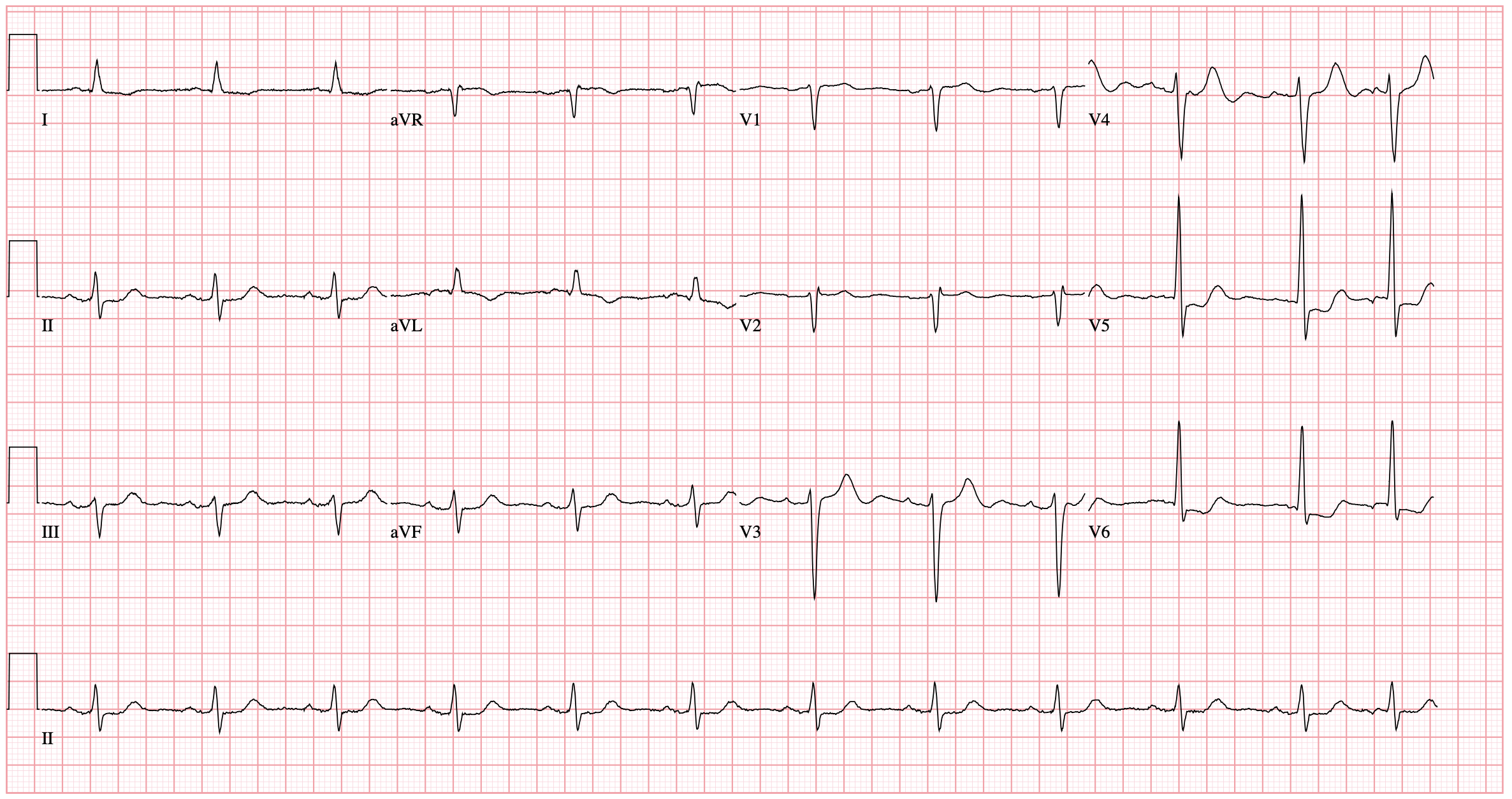
The patient is an 86 year old male hypertensive, dyslipidemic, diabetic, and CAD s/p PCI with Stenting of the LM to LAD and DCB of the proximal LCX last February 2025 presenting with angina. Current medications were Aspirin 80 mg, Clopidogrel 75 mg, Olmesartan 40 mg, Atorvastatin 80 mg, Ezetimibe 10 mg, and Amlodipine 5 mg, each once daily. PE showed BP of 150/70 mmHg, HR 58 bpm, regular rhythm, no murmurs, and clear breath sounds. ECG showed sinus rhythm, PACs, and ST-depression in leads V5-V6.
Relevant Test Results Prior to Catheterization
ECG revealed PACs with ST-depressions in leads V5-V6. Troponin I was elevated at 446. Transthoracic echocardiogram revealed concentric remodeling, mild hypokinesia in the anteroseptal wall at the mid and basal levels, and preserved LV ejection fraction at 69.3%.
 Echo-A4C.mov
Echo-A4C.mov
Echo-PLAX.mov
Relevant Catheterization Findings
Coronary angiogram showed the LM as a good-sized vessel with luminal irregularities. The LAD is a good-sized Type III vessel with a 30% late in-stent restenosis at the proximal to mid segment. The D1 is a fair-sized vessel with a 40% proximal stenosis. The LCX is a good-sized non-dominant vessel with a 99% ostioproximal stenosis. The obtuse marginal branches are fair-sized with luminal irregularities. The RCA is a good-sized dominant vessel with a patent proximal stent and a 30% mid stenosis.

clip-4.mp4
clip-5.mp4
clip-7.mp4
Interventional Management
Procedural Step
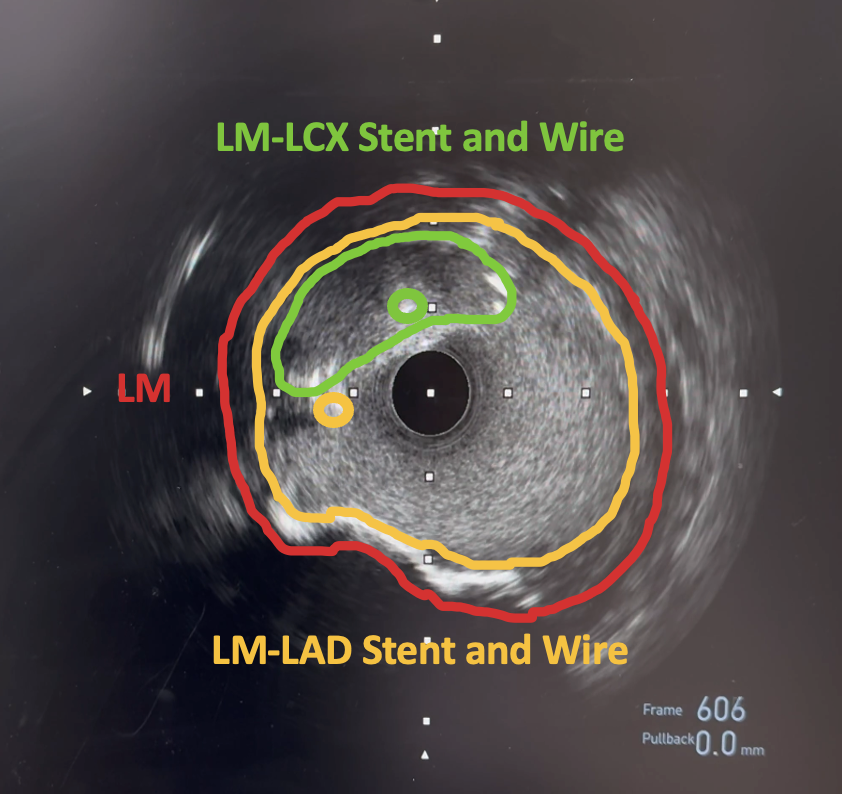
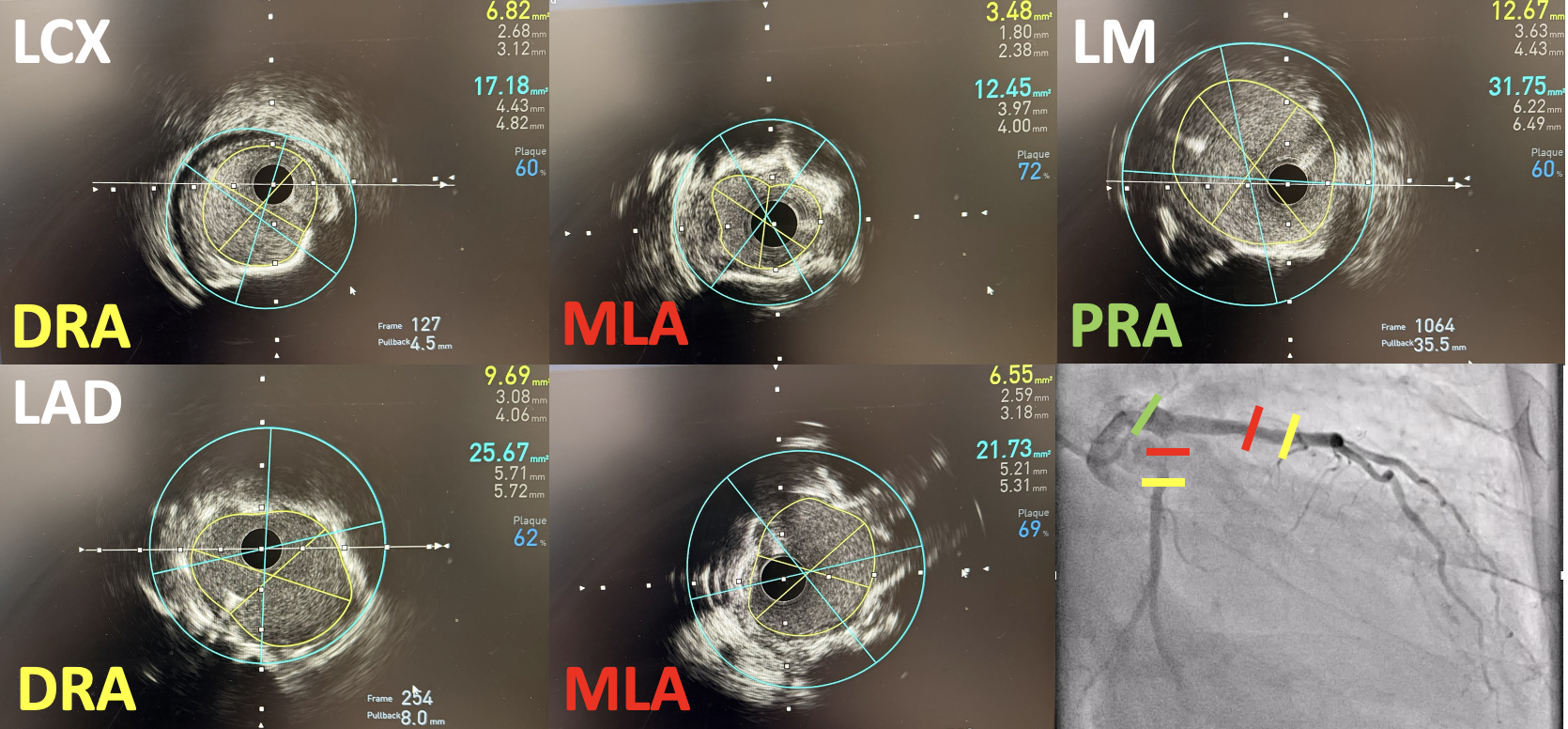
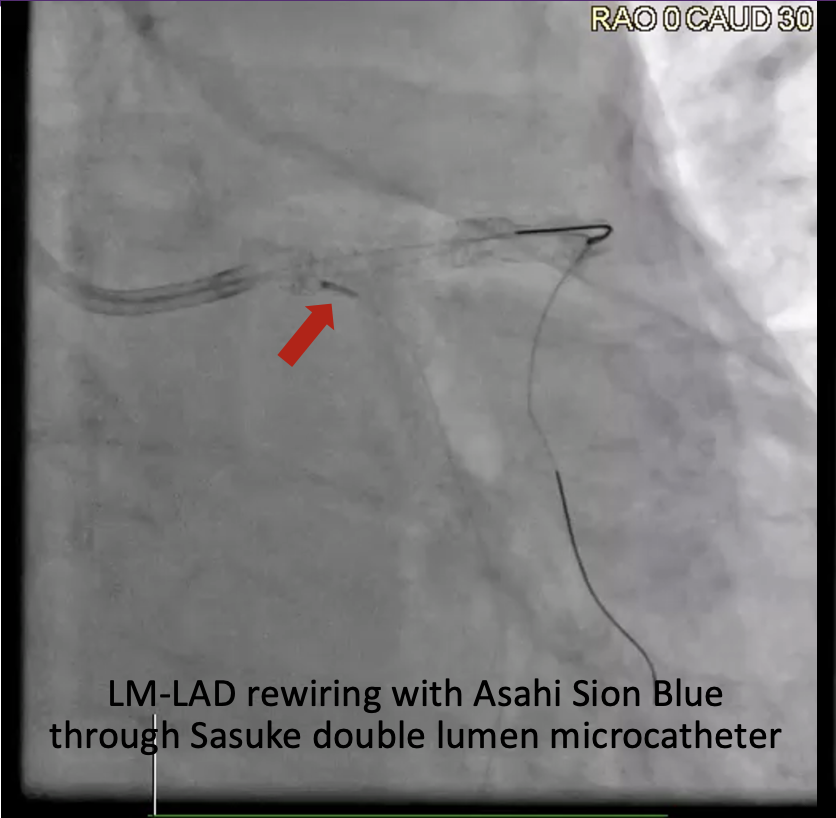
A 7F EBU 3.5 guide was used and an Asahi Sion Blue (Asahi Intecc, Japan) wire distalized into the LAD and a Sion wire crossed through the previous LM to LAD stent struts and distalized into LCX. After opening the stent struts, kissing balloon inflation (KBI) using a 3.5 mm balloon in the LM to LAD and a 2.5 mm balloon in the LM to LCX was done. IVUS showed LCX MLA of 3.48 mm2 and LAD MLA of 6.55 mm2. IVL in the LCX was done using a 3.0 mm IVL balloon for 8 cycles then in the LAD using a 4.0 mm IVL balloon for 5 cycles. A Xience Sierra (Abbott Vascular, USA) 3.0 mm x 33 mm stent was deployed at the LM to LCX then a POT at the LM. A Sion Blue was crossed through the LM to LCX stent struts and distalized into the LAD. Another KBI was done then a 4.0 mm DCB was deployed at the ostioproximal LAD for 1 minute. There was noted difficulty advancing the IVUS catheter past the proximal stent edge at the LM through the LM to LCX guidewire. IVUS of the LAD showed abluminal rewiring of the LAD stent resulting in an intraluminal jailing of the LCX wire and a stented double lumen LM. To resolve this, a Sion Blue was crossed through the LM to LCX stent struts through an Asahi Sasuke (Asahi Intecc, Japan) double lumen microcatheter and distalized into the LAD. Inflations with a 3.0 mm balloon at the LM to LCX were done followed by another KBI and finally POT at the LM. Final IVUS showed good stent expansion and apposition, LM MSA of 13.20 mm2, LAD MSA of 9.69 mm2, and LCX MSA of 6.23 mm2.
LM-LAD-LCX KBI.mp4
Double Lumen LM.mov
Final.mp4
Case Summary
Final angiography revealed TIMI III flow with no residual stenosis, dissection, or perforation. The patient tolerated the procedure well without hemodynamic instability or other complications. He was transferred to the telemetry unit and completed cardiac rehabilitation prior to discharge. In consideration of the patient's late restenosis only 5 months after his initial PCI, intravascular lithotripsy, stenting of the LM to LCX, and DCB of the LAD were effective treatments to address the restenosis. In addition, utilization of IVUS and a double lumen microcatheter were effective strategies to resolve an abluminal wiring and double lumen stent complication in the LM bifurcation.