Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_028
The Hidden Giant: Late Discovery of a Giant Right Coronary Artery Aneurysm Following Drug-Eluting Stent Implantation
By Afifah Suhailah Awang Soh, Muhammad Farid Mohd Fauad, Dhani Darshan Francis, Selva Kumar Sivan, Mohd Firdaus Ab Rahman, Faisal Ismail, Muizzuddin Roslan, Mubarak Mohd Yusof, Noordini Mohamed Dani, Siti Khairani Zainal Abidin, Anwar Irawan Ruhani
Presenter
Afifah Suhailah Awang Soh
Authors
Afifah Suhailah Awang Soh1, Muhammad Farid Mohd Fauad1, Dhani Darshan Francis1, Selva Kumar Sivan1, Mohd Firdaus Ab Rahman1, Faisal Ismail1, Muizzuddin Roslan1, Mubarak Mohd Yusof1, Noordini Mohamed Dani1, Siti Khairani Zainal Abidin1, Anwar Irawan Ruhani1
Affiliation
Hospital Tengku Ampuan Afzan, Kuantan, Malaysia1
View Study Report
CASE20251107_028
Coronary - Surgical Therapy (Coronary)
The Hidden Giant: Late Discovery of a Giant Right Coronary Artery Aneurysm Following Drug-Eluting Stent Implantation
Afifah Suhailah Awang Soh1, Muhammad Farid Mohd Fauad1, Dhani Darshan Francis1, Selva Kumar Sivan1, Mohd Firdaus Ab Rahman1, Faisal Ismail1, Muizzuddin Roslan1, Mubarak Mohd Yusof1, Noordini Mohamed Dani1, Siti Khairani Zainal Abidin1, Anwar Irawan Ruhani1
Hospital Tengku Ampuan Afzan, Kuantan, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 54-year-old man with hypertension, dyslipidaemia, and prior PCI with DES to the proximal RCA in 2018 presented with six months of exertional angina (CCS II) despite adherence to medical therapy. He was alert and hemodynamically stable (BP 136/76 mmHg, PR 78 bpm). Physical examination was unremarkable. No signs of heart failure or ischemia were noted.
Relevant Test Results Prior to Catheterization
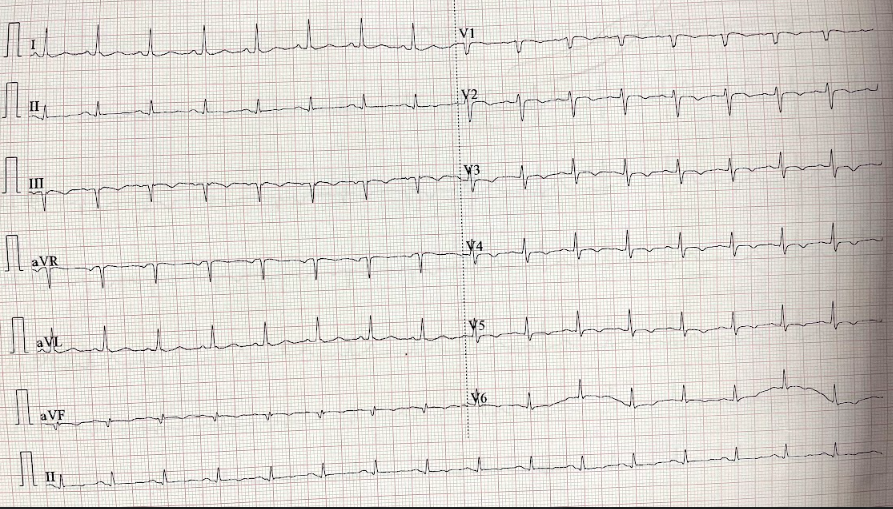
Hb 14 g/dL, platelet 267 × 10⁹/L, urea 7 mmol/L, creatinine 82 µmol/L.ECG showed T-wave inversion in leads V2–V5 and inferior leads.Chest radiograph was normal.Transthoracic echocardiography revealed LVEF 45–50% with inferior wall hypokinesia.

Relevant Catheterization Findings
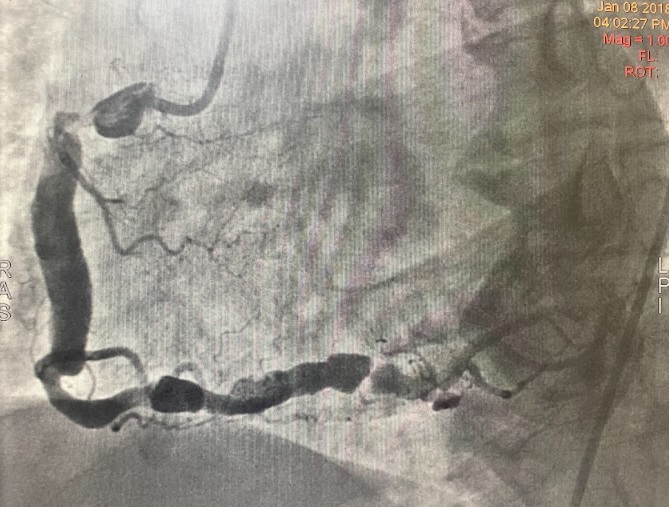
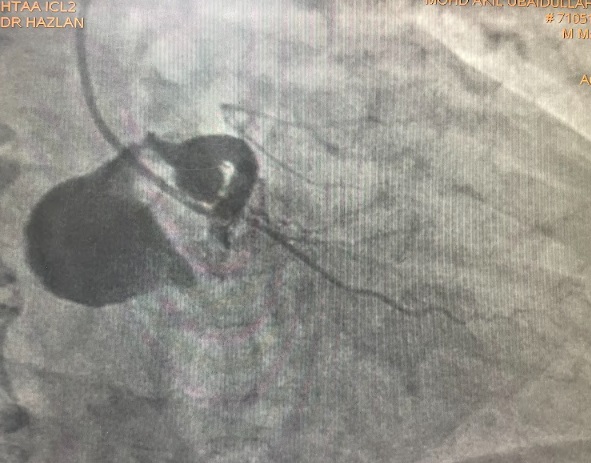
Coronary angiography showed a dominant RCA with a large proximal aneurysm measuring 4.5 × 17 mm, with in-stent restenosis proximal to the aneurysm. Mid-to-distal RCA was ectatic. The LM, LAD, and LCx were also mildly ectatic but without significant stenoses. These findings were consistent with a giant RCA aneurysm, likely related to prior stent implantation.


 RCA COROS video.mov
RCA COROS video.mov
RCA COROS 2 video.mov
RAO CAUDAL video.mov
Interventional Management
Procedural Step
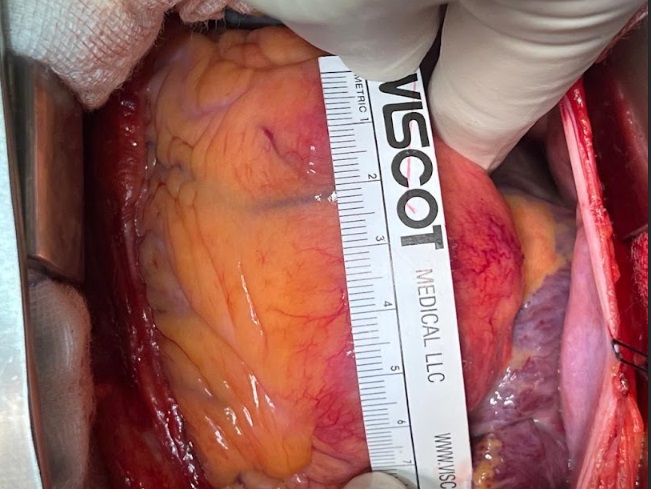
The patient was referred for urgent coronary artery bypass grafting (SVG–RPDA) and surgical repair of the RCA aneurysm. Under general anesthesia, median sternotomy and pericardiotomy were performed. The saphenous vein graft was harvested using endoscopic vein harvesting (EVH). After systemic heparinization, cardiopulmonary bypass was initiated. The aorta was cross-clamped, and cold blood cardioplegia was administered antegrade into the aortic root and retrograde via the coronary sinus to achieve cardiac arrest. On exploration, the aneurysm was located at the proximal RCA corresponding to the previous stent site. The sac was opened, revealing an organized thrombus, which was evacuated. The aneurysm wall was partially excised, and both proximal and distal ends were ligated with pledgeted 4/0 prolene sutures to exclude it from the circulation. The RCA wall was reinforced with a continuous prolene closure. Following exclusion, a saphenous vein graft was anastomosed to the distal RCA (RPDA), followed by proximal grafting to the ascending aorta under a single cross-clamp. The patient was rewarmed and successfully weaned off cardiopulmonary bypass with low-dose adrenaline support. Hemostasis was achieved, and the sternum was closed. He was transferred to CICU for monitoring and recovered uneventfully.


RCA aneurysm video.mp4
RCA incision VIDEO.mp4
RCA inside after removal of thrombus video.mp4
Case Summary
This case illustrates a rare and life-threatening late complication of DES implantation—formation of a giant RCA aneurysm presenting as recurrent angina. Coronary aneurysm should be considered in post-PCI patients with unexplained ischemic symptoms. Early recognition via angiography and multidisciplinary management are essential to prevent rupture or thrombosis. Surgical exclusion with distal grafting remains the optimal treatment for large, symptomatic aneurysms. This case highlights the need for long-term vigilance and imaging surveillance following PCI, as even routine follow-up angiography can reveal critical, unexpected findings.