Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_026
PCI in Calcified Left Main: Balancing Risk, Flow, and Strategy
By Yen-Tuan Huang
Presenter
Yen-Tuan Huang
Authors
Yen-Tuan Huang1
Affiliation
Taichung Veterans General Hospital, Taiwan1
View Study Report
CASE20251107_026
Coronary - Complex PCI - Left Main
PCI in Calcified Left Main: Balancing Risk, Flow, and Strategy
Yen-Tuan Huang1
Taichung Veterans General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
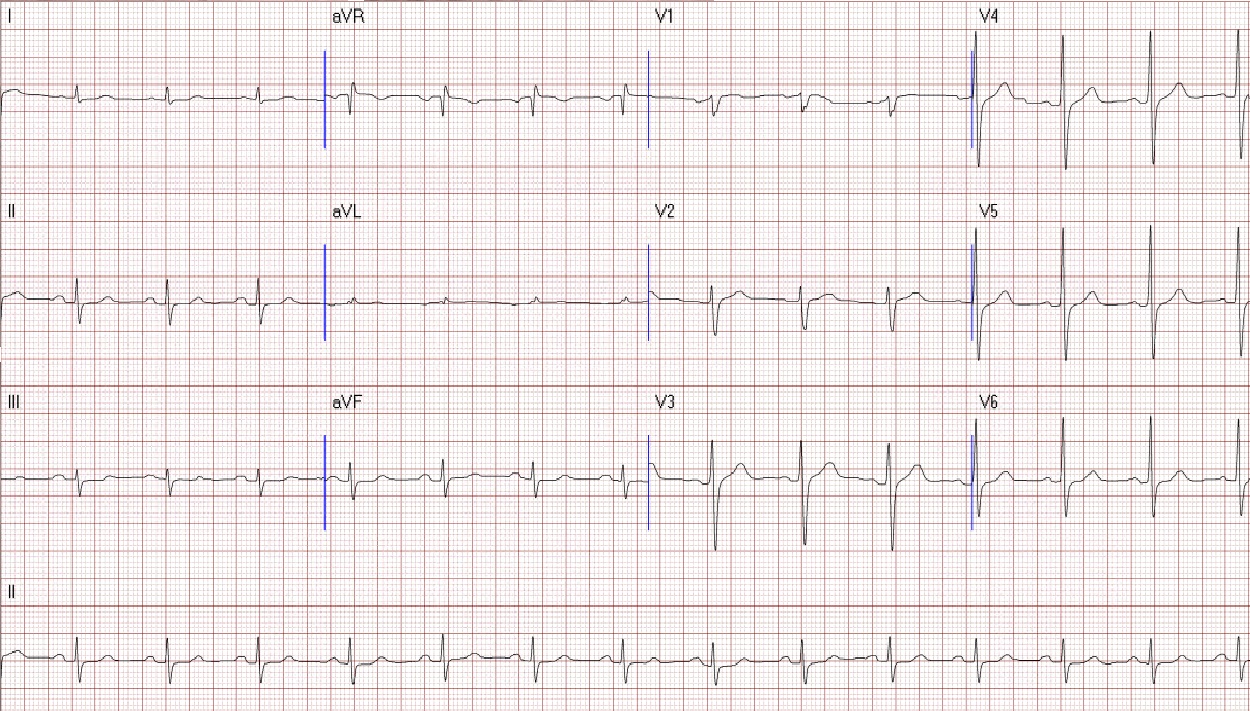
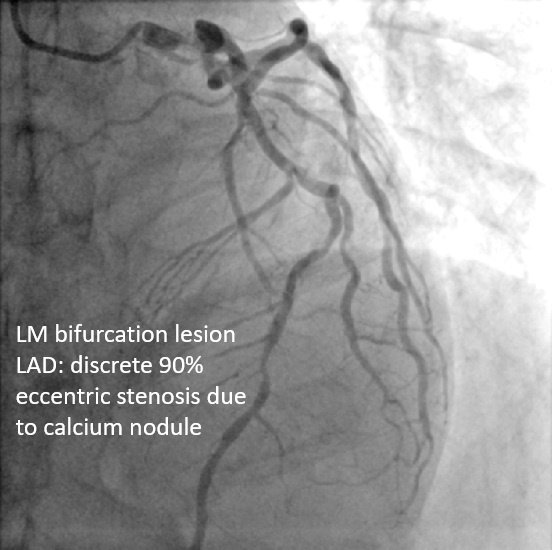
A 64-year-old male with chest pain and tightness during exertion for 2 months, relieved by rest. Past history: type 2 diabetes, hypertension. No smoking or family history. Sinus rhythm EKG. Clear lungs, no cardiomegaly on chest x-ray. Angiography: LM bifurcation (Medina 1,1,1), diffuse LAD, severe LCX AS, 95% eccentric LAD, long RCA CTO. Syntax score 25, EuroScore II 0.84%. CABG advised, patient sought second opinion here.

Relevant Test Results Prior to Catheterization
Labs: Hb 15.8, PLT 139k, Cr 1.25, LDL 88, HbA1c 7.7.
Relevant Catheterization Findings
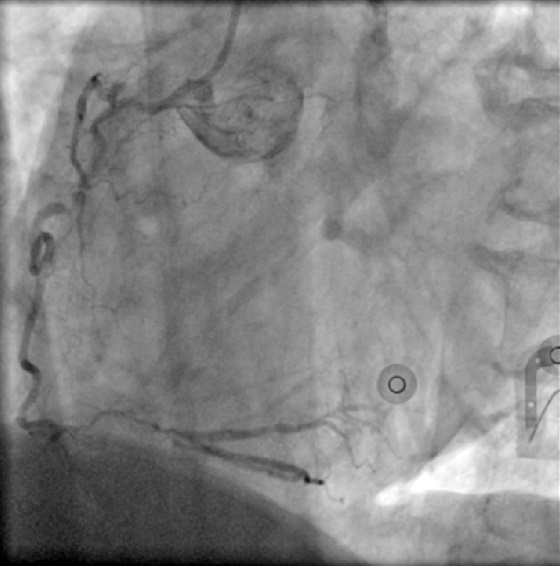
Cath report from referring hospital-LM:bifurcation lesions (1,1,1 type; 90%, 90%, 30% stenosis)-LAD:Diffuse lesions with acute bends-LCX:Severe AS changes with discrete 95% due to eccentric plaque at proximal LAD-RCA:Long CTO lesion
 LM外院片.avi
LM外院片.avi
LM外院片-2.avi
RCA外院片.avi
Interventional Management
Procedural Step
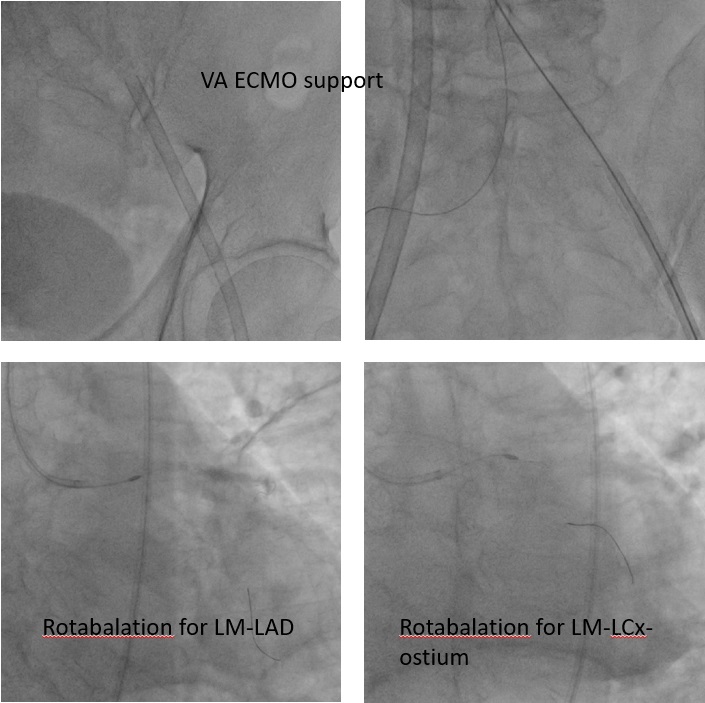
PCI was performed via a right femoral 7 Fr EBU 3.0 guide. LCX wiring was extremely challenging due to a large ostial aneurysm and discrete stenosis; reverse wiring failed, so the LAD was treated first. Using a Caravel microcatheter, an extra-support Rotawire was advanced, and sequential 1.25 mm and 1.75 mm burr atherectomy was done for LAD and LM–LAD segments. A 2.0 mm burr was avoided due to iliac angulation. After adequate LAD preparation, LCX wiring succeeded with a Suoh 03 wire, exchanged for a Rota Extra Support wire via Caravel. LM–LCX ostium was ablated with 1.25 and 1.75 mm burrs, though the burr could not enter LCX proper.
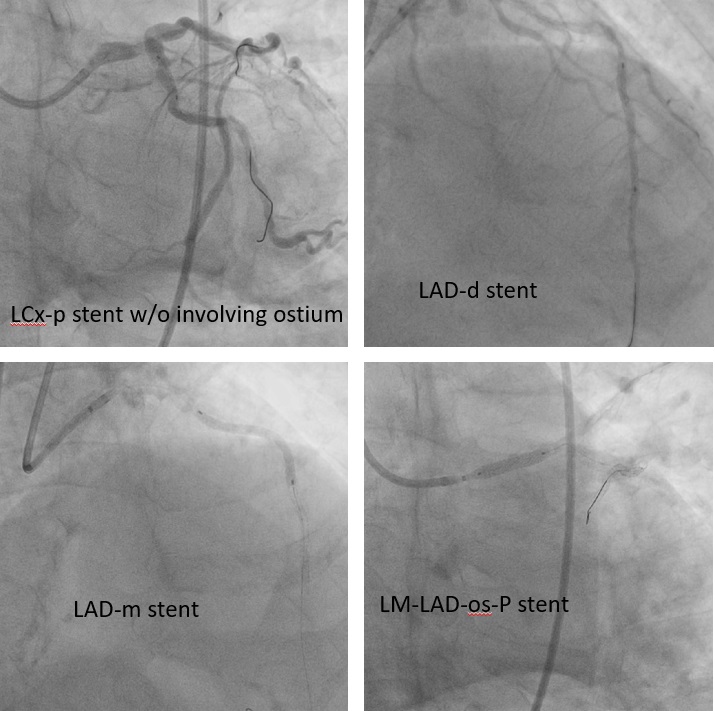
Suboptimal balloon dilation led to implantation of a 2.75 × 8 mm Onyx DES at the LCX ostium. The LAD was predilated and treated with 2.0 × 38 mm and 2.5 × 38 mm Xience Sierra stents plus a 3.5 × 15 mm Megatron for LM–LAD. IVUS confirmed full stent expansion and apposition with no residual stenosis. A minor LAD ostial type II dissection was observed but without flow limitation.
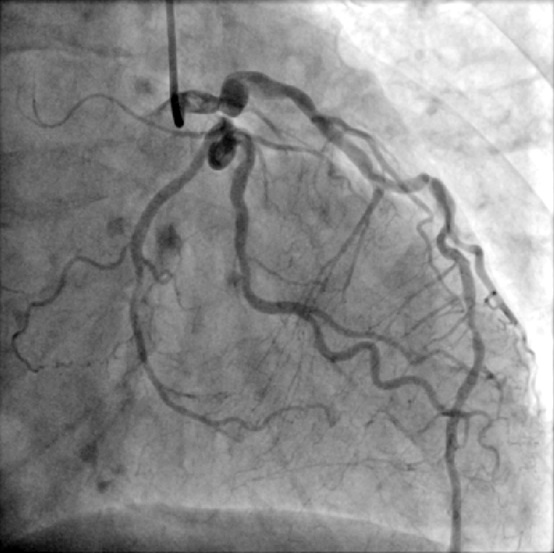
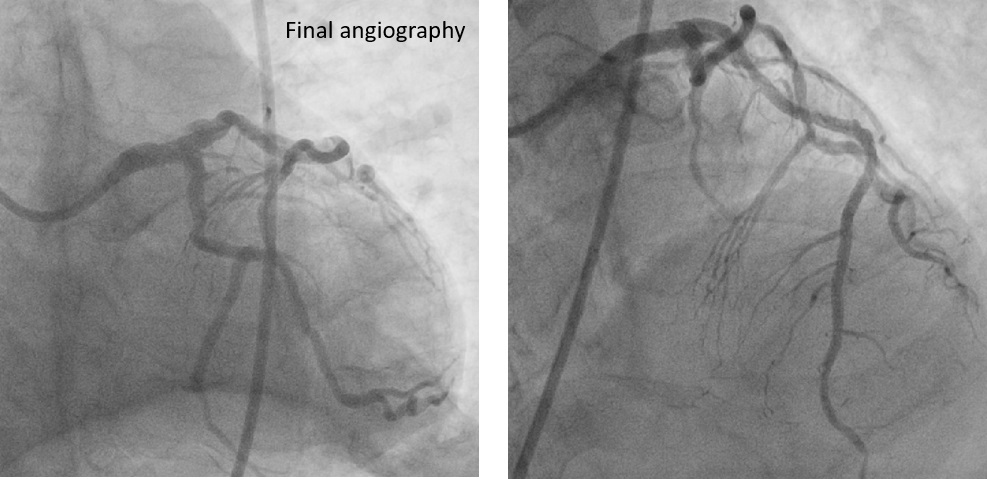
Final angiography showed excellent patency. ECMO was removed uneventfully, and manual hemostasis achieved due to femoral aneurysms precluding device closure.
Case Summary
ECMO-assisted PCI enabled safe revascularization of severe left main and triple-vessel disease with heavy calcification and complex peripheral anatomy. Temporary circulatory support maintained stability during atherectomy and stenting. IVUS confirmed full stent expansion and apposition. Careful planning and coordinated management allowed successful outcome without complications.