Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_024
A Challenging Case Report: Novel Strategy Using Crocodile Forceps for Gallbladder to Retrieve Migrating GORE Atrial Septal Defect Occluder
By Shintaro Kuroyanagi, Hiroki Niikura, Waga Sari, Shio Ide, Kenji Makino, Go Hashimoto, Hidehiko Hara
Presenter
Shintaro Kuroyanagi
Authors
Shintaro Kuroyanagi1, Hiroki Niikura1, Waga Sari1, Shio Ide1, Kenji Makino1, Go Hashimoto1, Hidehiko Hara1
Affiliation
Toho University Ohashi Medical Center, Japan1
View Study Report
CASE20251107_024
Structural - Other Structural Interventions
A Challenging Case Report: Novel Strategy Using Crocodile Forceps for Gallbladder to Retrieve Migrating GORE Atrial Septal Defect Occluder
Shintaro Kuroyanagi1, Hiroki Niikura1, Waga Sari1, Shio Ide1, Kenji Makino1, Go Hashimoto1, Hidehiko Hara1
Toho University Ohashi Medical Center, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
Twenty-six years old male with dyspnea on effort was introduced to our center for percutaneous atrial septal defect (ASD) closure. His heart failure symptom was NYHA class 2m. The auscultation revealed systolic ejection murmur 2/6 at the left second sternal border.
Relevant Test Results Prior to Catheterization
The transthoracic echocardiogram showed a secundum ASD with a dilated right heart, and the transesophageal echocardiogram revealed an ASD without an anterior aortic rim at the 30° view, measuring 16.4 × 11.4 mm. The other rims appeared sufficient, and there was a septal malalignment. Therefore, this case was considered a good indication for percutaneous ASD closure, especially using a GORE ASD Occluder, because of the aortic rim defect.
Relevant Catheterization Findings
The patient underwent percutaneous ASD closure with local anesthesia. We confirmed the defect size with intracardiac echo (ICE) and a sizing balloon which showed 15.1mm. Thus, we chose GORE Cardioform ASD (GCA) Occluder 37mm according to the sizing chart.
Interventional Management
Procedural Step
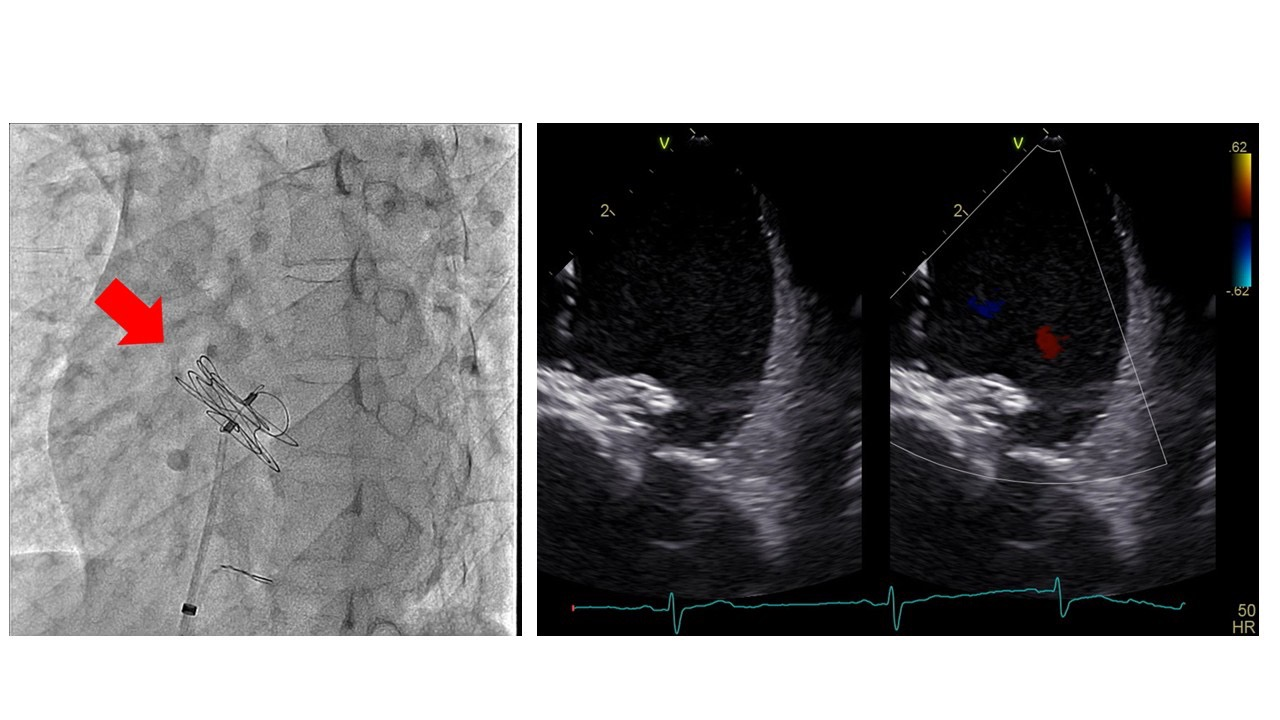
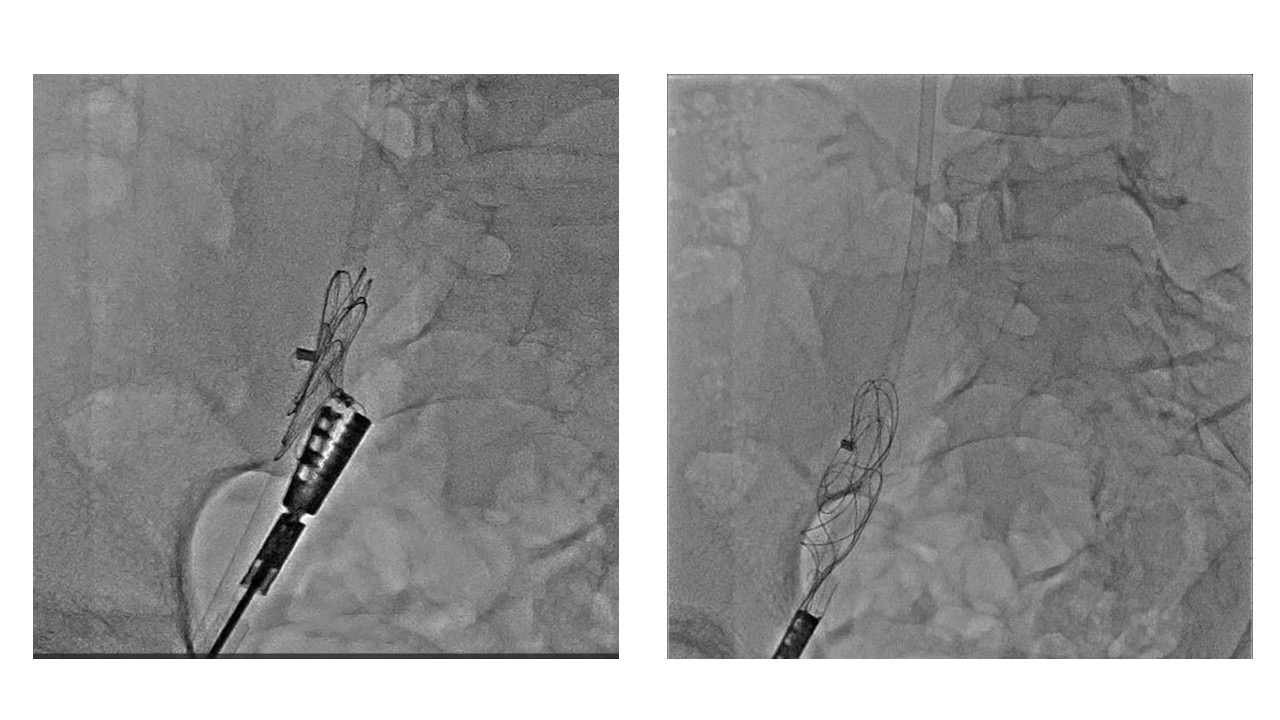
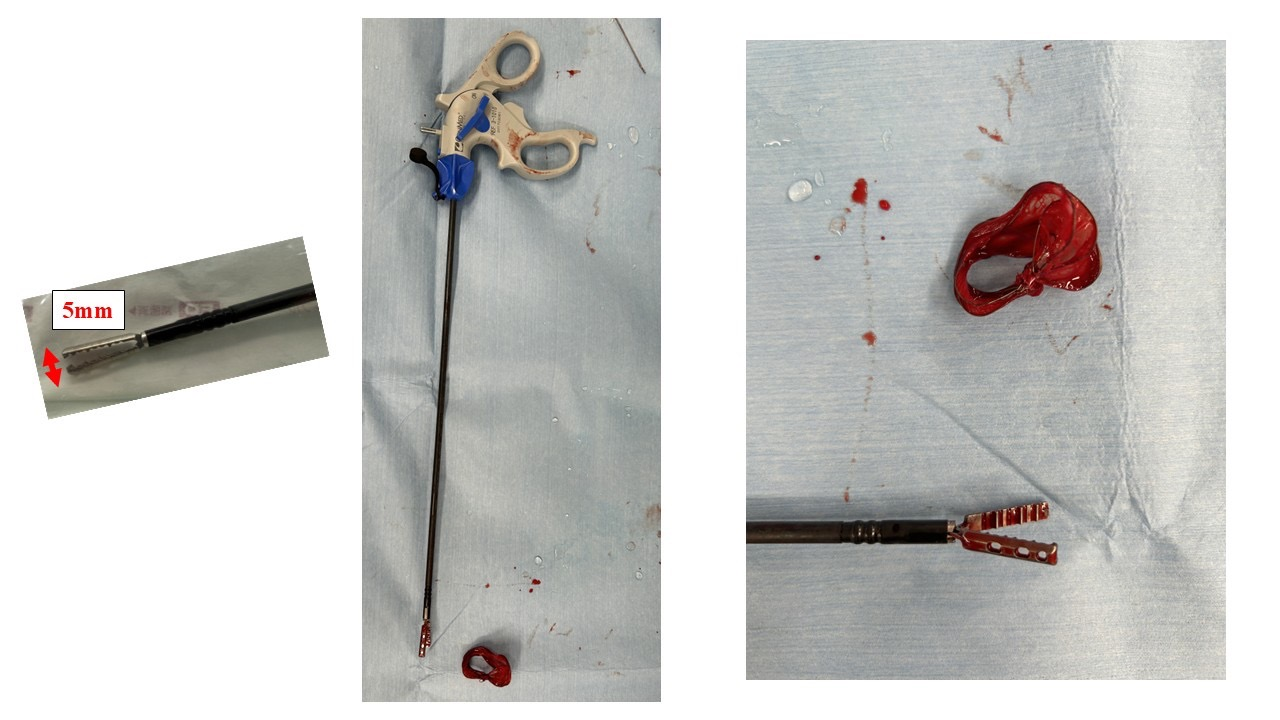
The GCA was deployed as usual with fluoro and ICE images. However, the device gradually began to move inappropriately, and we understood it hadn’t been deployed properly. Thus, we decided to retrieve and change the device. At first, we tried to retrieve it still attaching the atrial septum using standard EN snare, and caught the lock loop to remove from the atrial septum, however it came off the snare catheter because of weak locking loop wire. Next, we caught the floating device in right atrium with biopsy forceps and succeeded to pull it down to the iliac vein. Unfortunately, we could not move the occluder into the sheath, as its slippery designed hub and bulky device body even using combination of snare with biopsy forceps. Finally, we decided to insert 16 Fr. size sheath to use Crocodile Forceps for surgical gallbladder operation like laparoscopic cholecystectomy as its powerful gripping force.
Case Summary
We experienced a very difficult procedure in which ordinary snare and forceps were useless to retrieve the migrating occluder. In the end, we were able to retrieve the GCA occluder using strong crocodile forceps usually used in laparoscopic cholecystectomy, and closed the ASD with Figulla Flex 2 occluder.