Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_023
Three-Time Encounter: Complex PCI Management Strategy After Failed CABG
By Sondang Jasmine Mustikasari, Chunjian Li
Presenter
Sondang Jasmine Mustikasari
Authors
Sondang Jasmine Mustikasari1, Chunjian Li1
Affiliation
Jiangsu Province Hospital (The First Affiliated Hospital of Nanjing Medical University), China1
View Study Report
CASE20251107_023
Coronary - Complex PCI - Calcified Lesion
Three-Time Encounter: Complex PCI Management Strategy After Failed CABG
Sondang Jasmine Mustikasari1, Chunjian Li1
Jiangsu Province Hospital (The First Affiliated Hospital of Nanjing Medical University), China1
Clinical Information
Relevant Clinical History and Physical Exam
A 76-year-old man presented with worsening chest pain. He had a history of exertional angina and underwent CABG one year earlier for AMI. Comorbidities included hypertension, PAD, and previous cerebral infarction. Physical examination was unremarkable. Achieving optimal PCI and favorable clinical outcomes required three separate encounters—reminding us that success in the cath lab is not only about the lesion’s complexity, but the precision and execution of our strategy.
 LIMA.mp4
LIMA.mp4
CRA.mp4
RCA.mp4
Relevant Test Results Prior to Catheterization
Echocardiography showed LAD 27 mm, LVDd 43 mm, and a reduced LVEF of 41%. Segmental wall motion abnormalities were noted after previous CABG, with a tendency toward apical ventricular aneurysm formation. The mitral valve demonstrated severe regurgitation with leaflet malcoaptation, tricuspid valve showed moderate regurgitation, and the aortic valve was calcified with mild regurgitation. Pro-BNP level was 7836 pg/ml.
Relevant Catheterization Findings
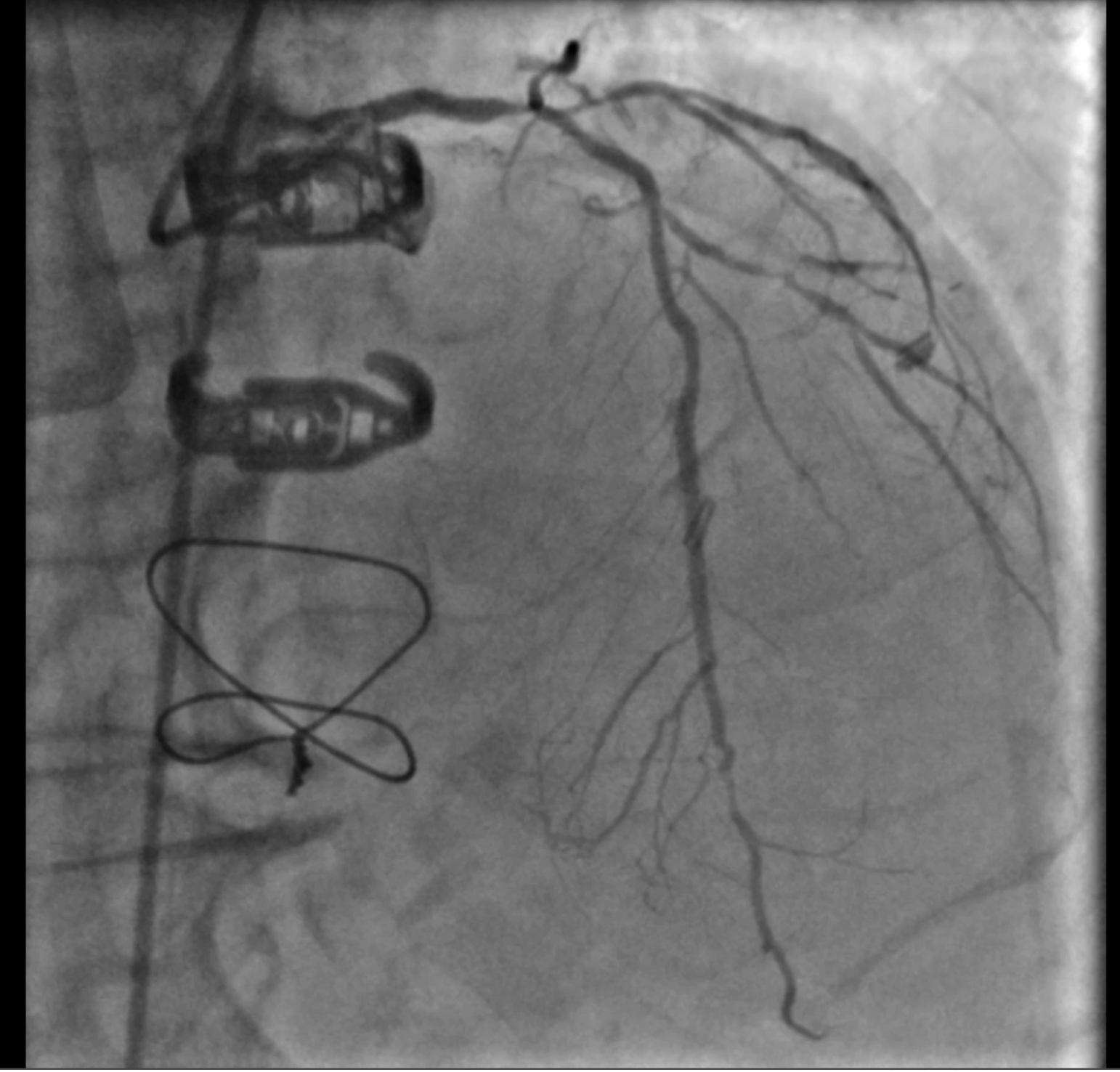
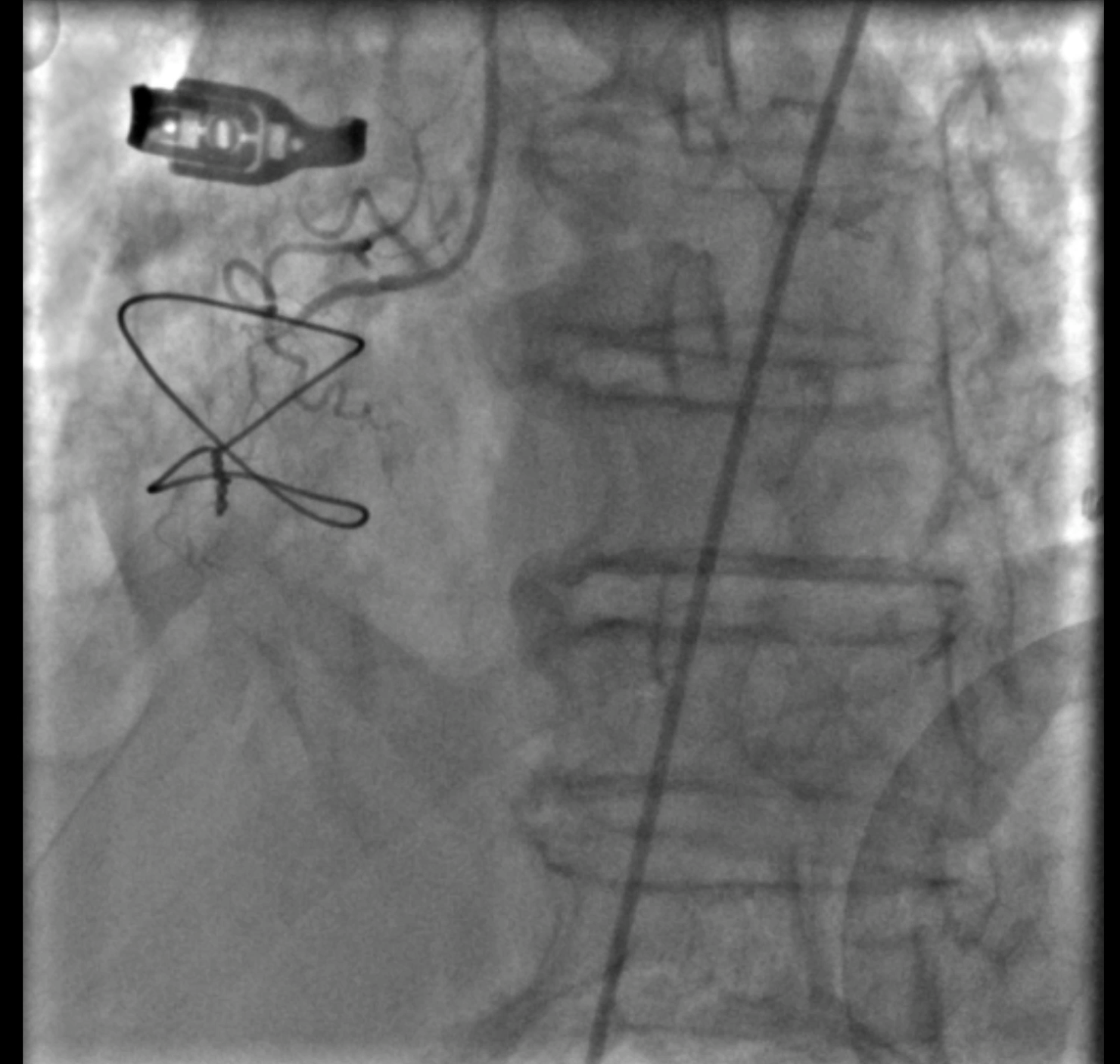
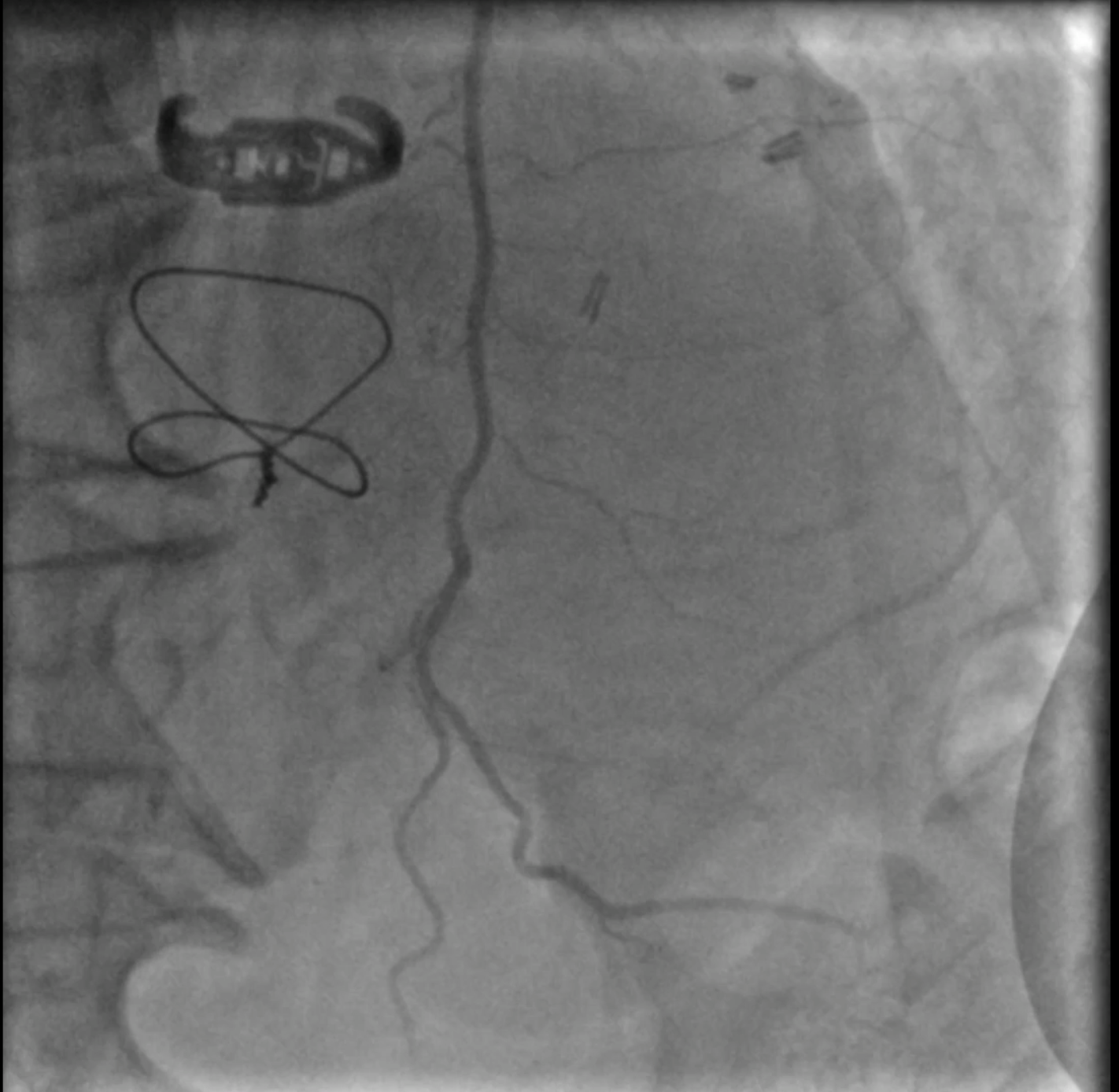
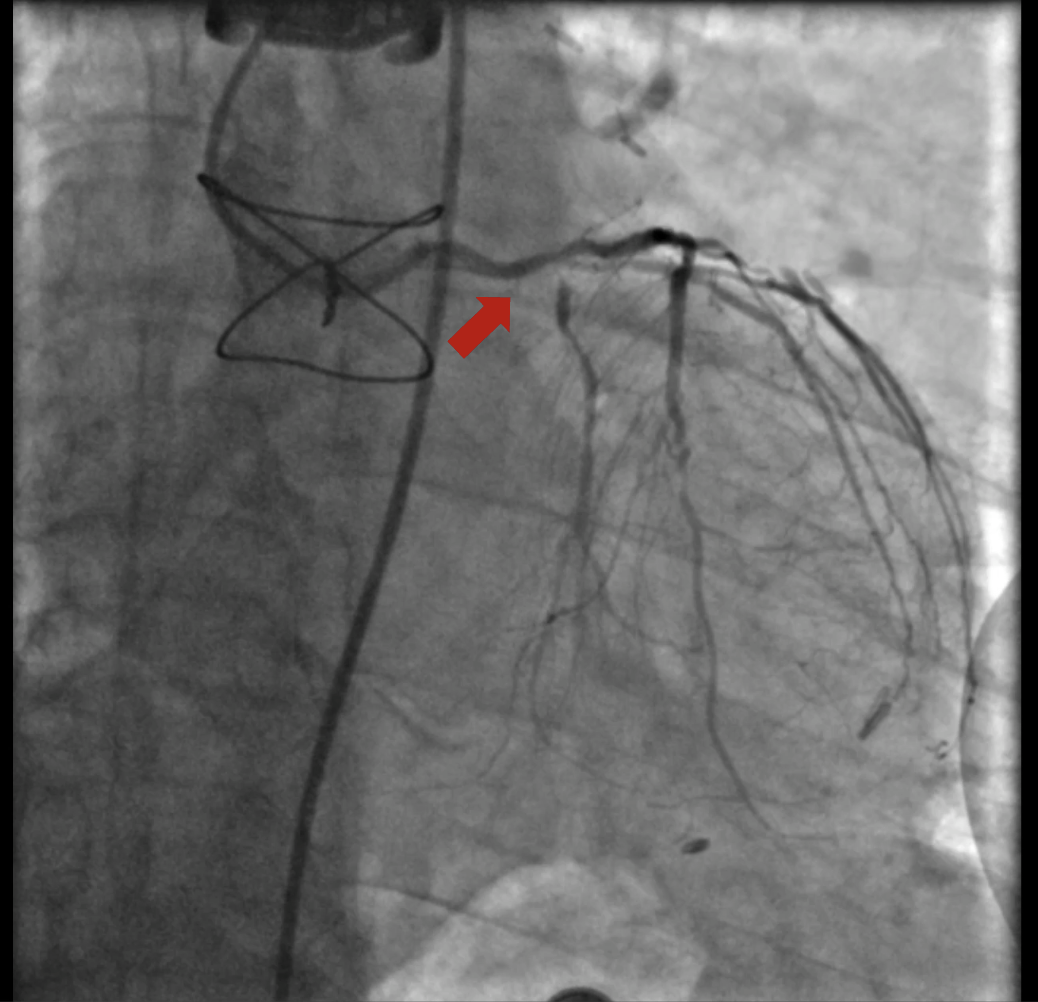
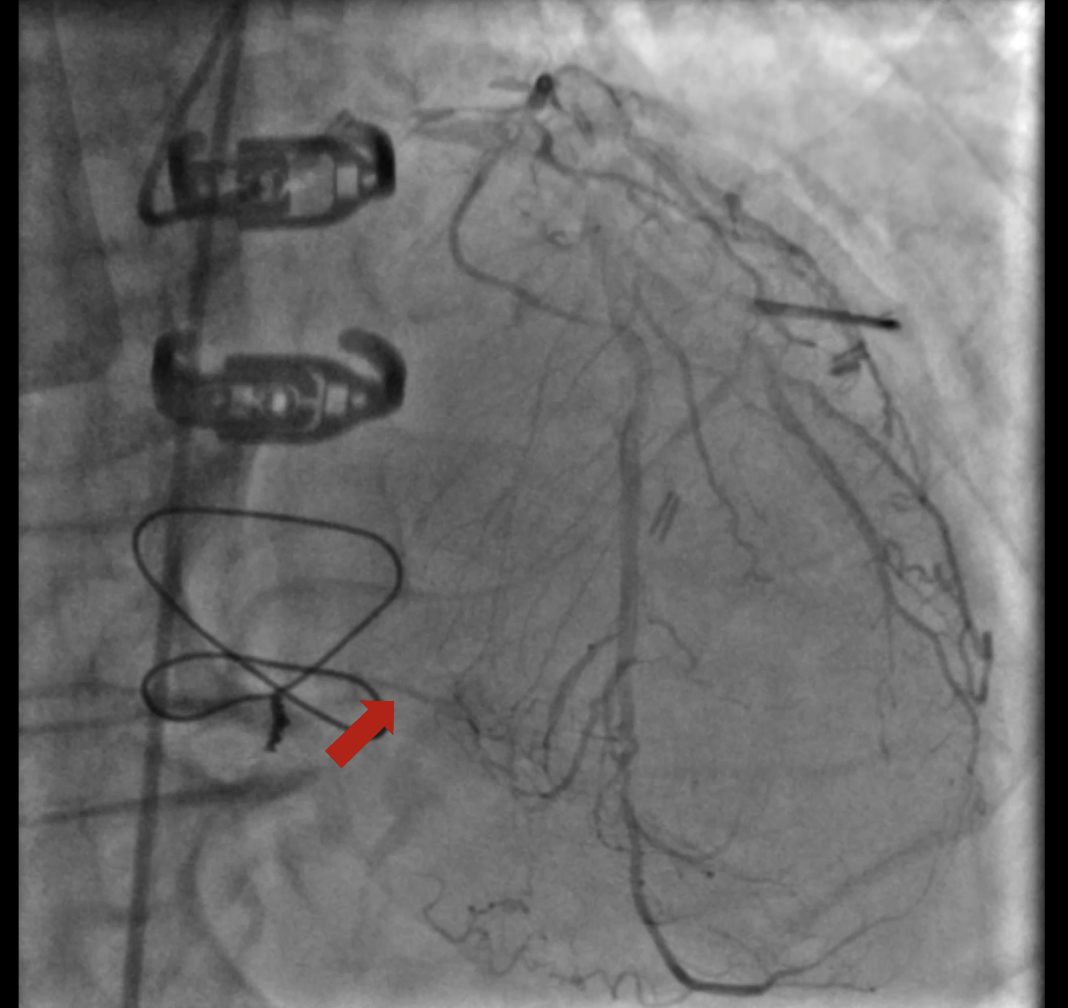
At the first encounter, coronary angiography revealed a left main bifurcation lesion (Medina 1-1-1) with 99% ostial stenosis of the LCX and severe stenosis in the proximal LAD and the 2nd diagonal branch. Collateral circulation was observed from the LAD and LCX to the distal RCA. Right coronary angiography showed a proximal CTO with a J-CTO score of 3 due to calcification, bending, and lesion length. The LIMA was not grafted to the LAD.
CAU.mp4
CRA.mp4
LIMA.mp4
Interventional Management
Procedural Step
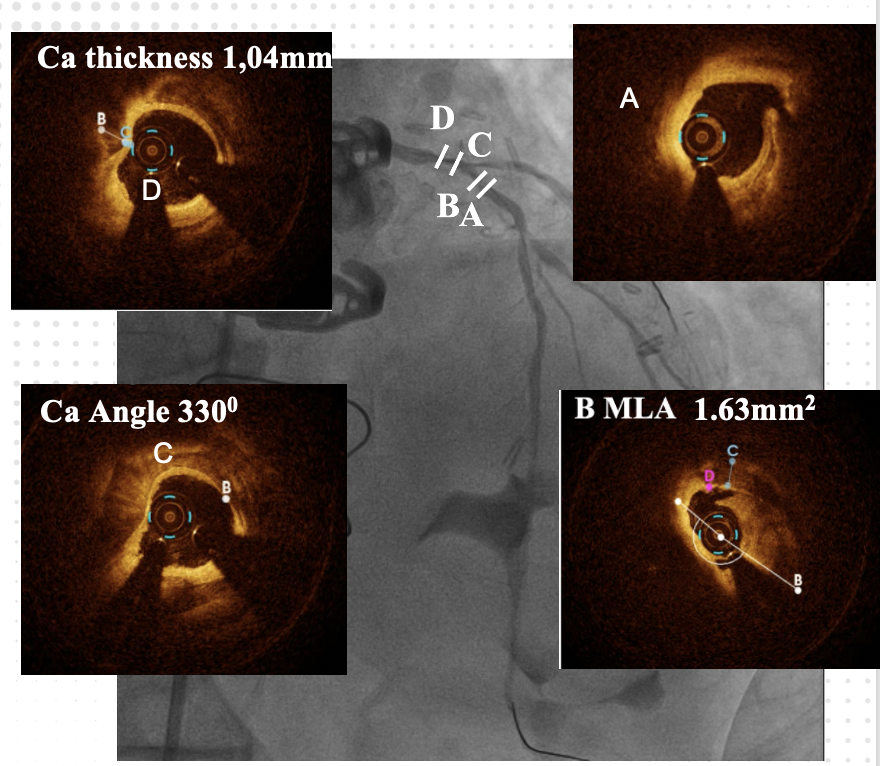
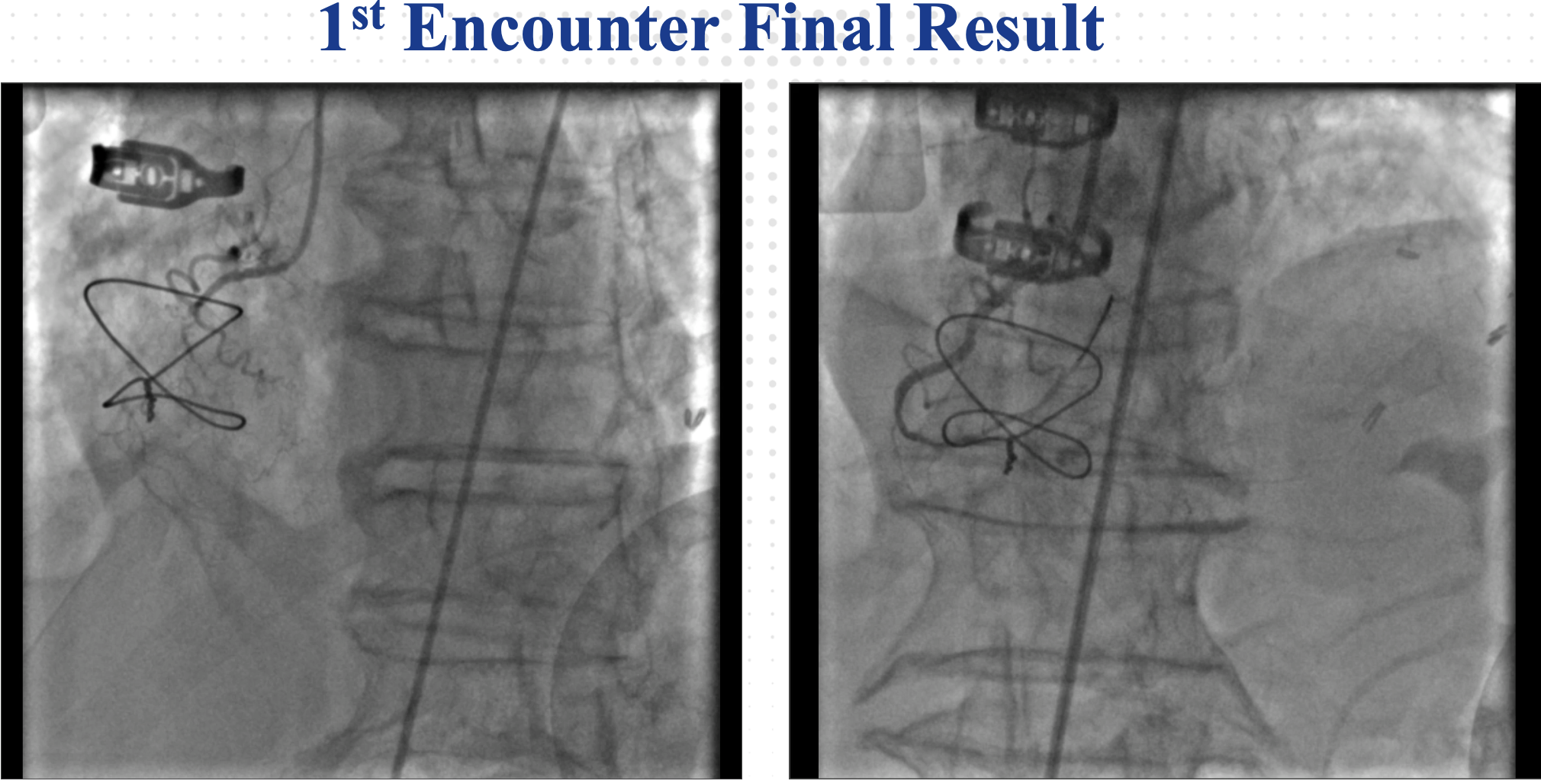
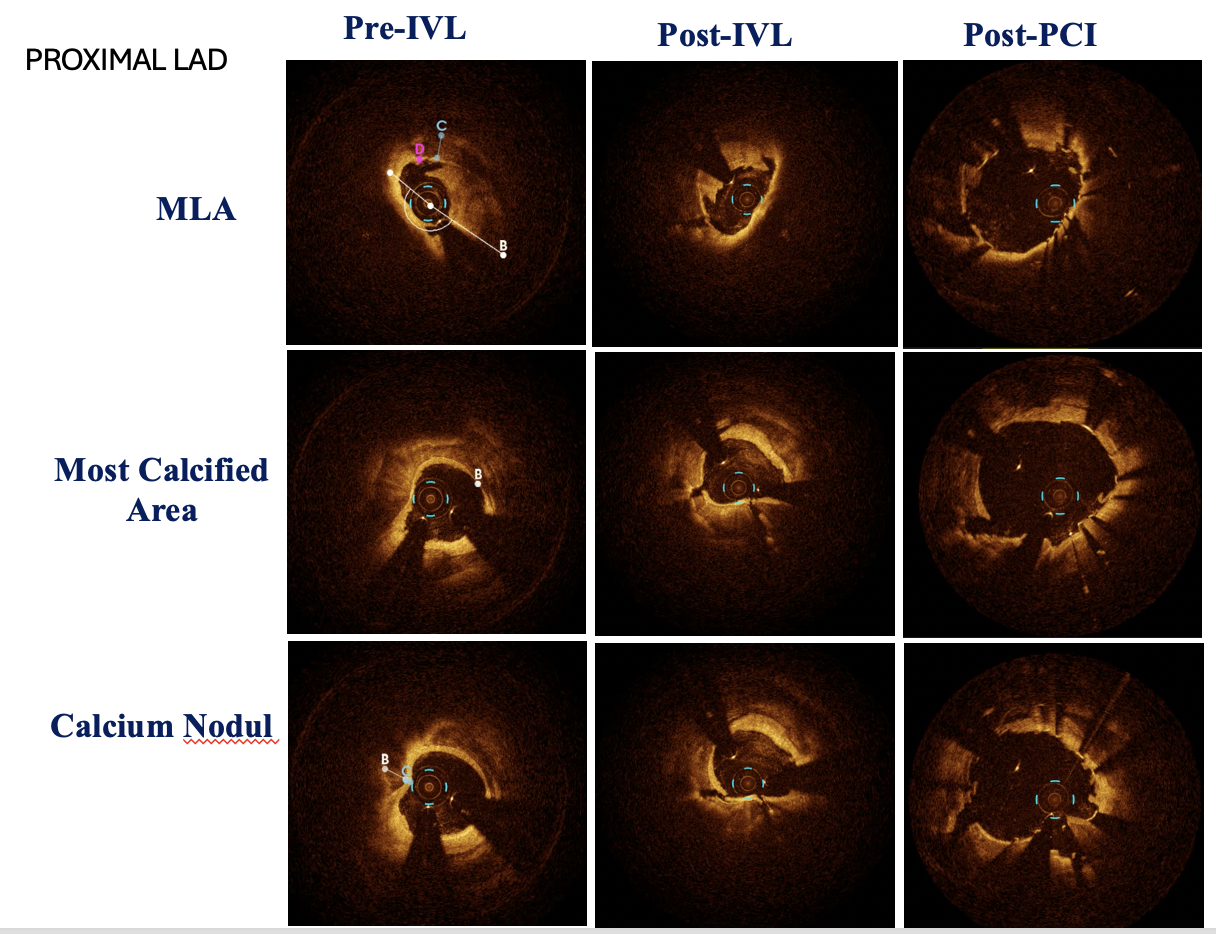
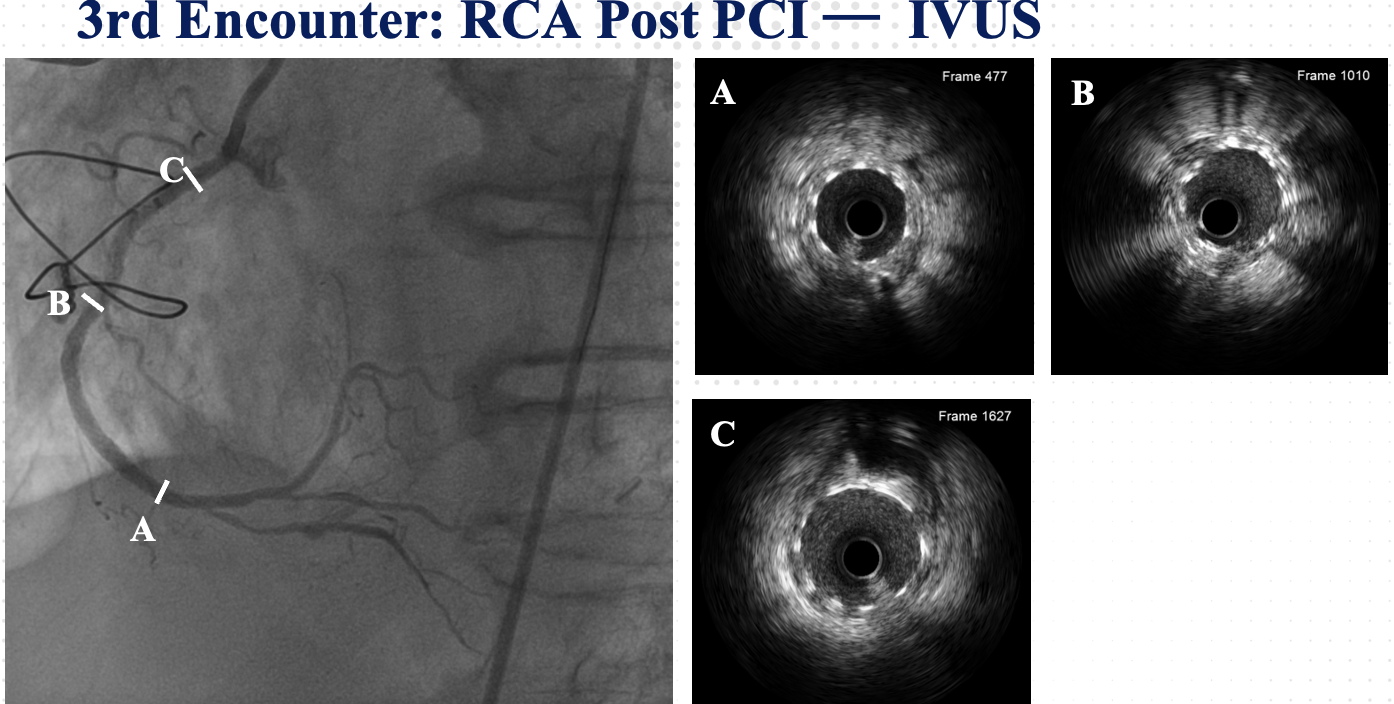
At the 1st encounter, RCA CTO PCI was performed with a plan for staged PCI of the left system. Using a 7F AL 0.75 for strong support, an antegrade approach with a double-lumen microcatheter and parallel wire technique (Pilot 150) successfully crossed the lesion. Predilatation with a 1.5 × 15 mm balloon was done. IVUS could not pass due to 360° calcification. Rotablation with a 1.25 mm burr was attempted but limited to mid-RCA. Two DES were implanted from mid to proximal RCA, followed by post-dilatation.At the 2nd encounter, RCA stents were patent. PCI was done on LM, LAD, and D2. D2 was treated with DCB. LAD predilatation followed by OCT showed severe 330° calcification (max thickness 1.04 mm, MLA 1.63 mm²). IVL with a 2.75 × 12 mm balloon (30 pulses) achieved multiple calcium fractures. A 2.75 × 33 mm DES was deployed with good OCT results.At the 3rd encounter, 6 months later, the patient presented with ADHF. Angiography revealed RCA ISR CTO at the mid-bending site. The lesion was crossed with a Pilot 200 wire; predilatation showed a dog-bone sign. We do balloon based strategy for plaque modification using cutting, scoring, and double-wire balloons. IVUS showed stent underexpansion with 270° calcification and distal RCA stenosis. IVL with 2.5 and 2.75 mm balloons optimized the lesion, followed by two DES from distal to mid RCA. Post-PCI IVUS confirmed good result.
Rota mid RCA.mp4
RCA after 1st pci.mp4
RCA ISR.mp4
Case Summary
Success in complex PCI begins with meticulous imaging—before, during, and after the procedure. Never rush; precision matters. Poor calcium preparation means poor outcomes. In the end, ihow many encounters we have in the cath lab, not just about how complex the case is, but also how well we arrange and execute our strategy.