Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_020
Disruption of Stuck Mechanical Prosthetic Valve: A Bailout Procedure
By Sumanta Shekhar Padhi
Presenter
Sumanta Shekhar Padhi
Authors
Sumanta Shekhar Padhi1
Affiliation
Raipur-MMI Narayana Superspeciality Hospital, India1
View Study Report
CASE20251107_020
Structural - Other Structural Interventions
Disruption of Stuck Mechanical Prosthetic Valve: A Bailout Procedure
Sumanta Shekhar Padhi1
Raipur-MMI Narayana Superspeciality Hospital, India1
Clinical Information
Relevant Clinical History and Physical Exam
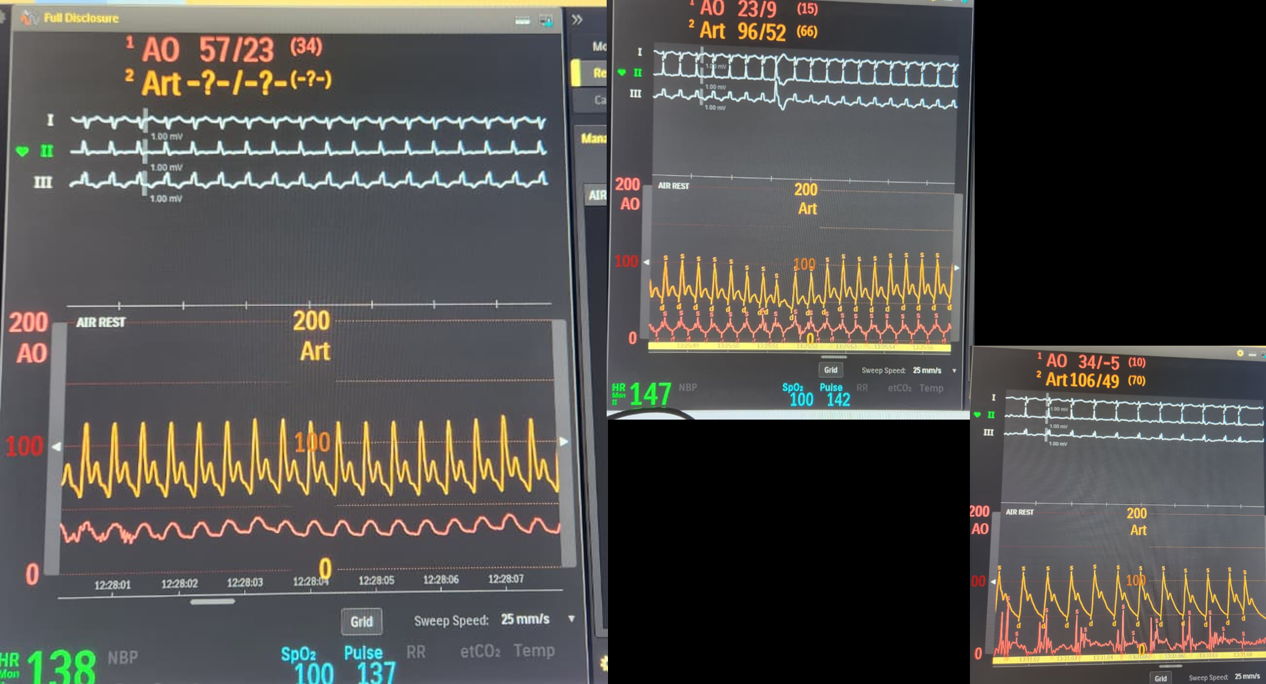
19yr/F,MVR ( 25mm CORCYM MPV)+ Pericardial patch closure ofASD-28.3.25.Discharged uneventfully. 1st FU @ 1 wk - INR 2.5.INR on 14.05.25- 2.9 ( send by Watts App) on 20.05.25 Fever& vomiting x 2 day,Possibly had vomited out one dose of Acitrome, Seve weakness and SOB. C/E: pulse ~ 130/min,SBP 80-90mmHg,Sat ~ 90%,Severe Metacidosis – pH- 7.2, Lactates > 15, BE- >-20,Evevated liver enzymes andINR > 5,Put on BIPAP, notrope- Nad, IV bicarbonate
Relevant Test Results Prior to Catheterization
Initial plan- TLT not done in v/o very high INR. Started onIV UFH. FFP and Vi t K was given to correct the INR and then TLT.After 6 hr –needed Intubation and mechanical ventilation ,TEE done to know the mechanism of valve non function
Relevant Catheterization Findings
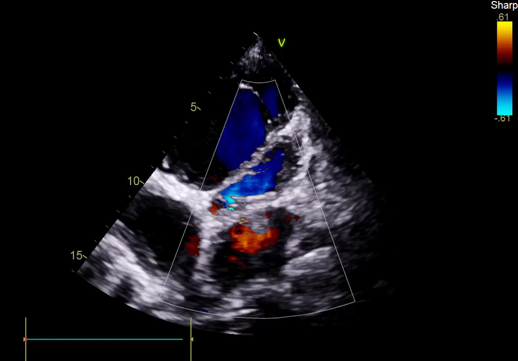
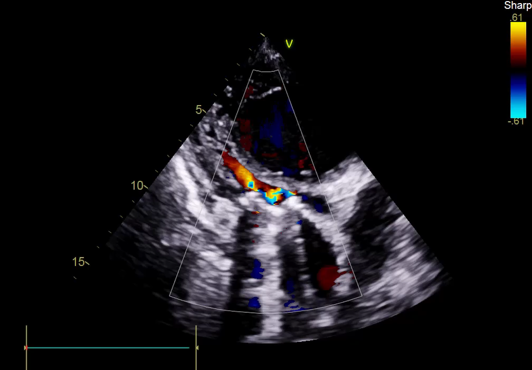
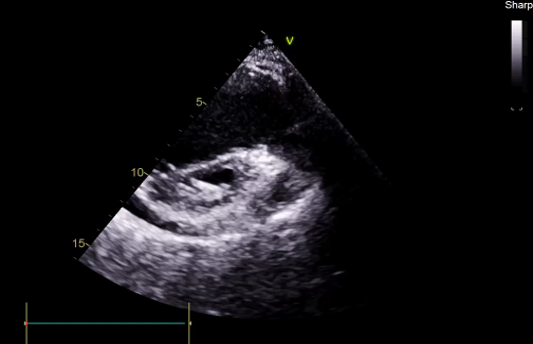
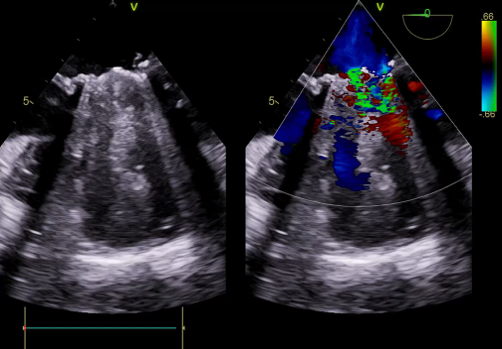
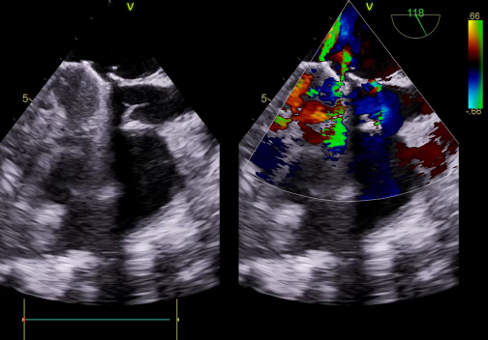
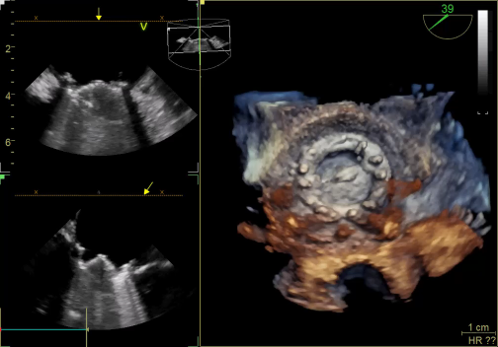
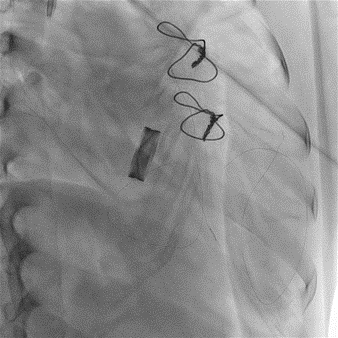
TEE, TEE and Floro showed both the leaflets to be stuck, almostno flow across the PV. The RV was higely dilated and there was severe RVdysfunction
Interventional Management
Procedural Step
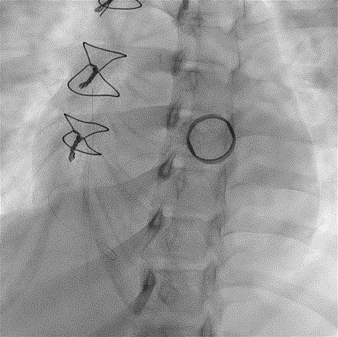
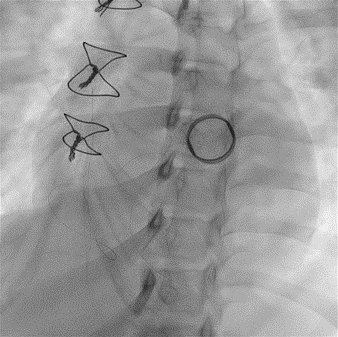
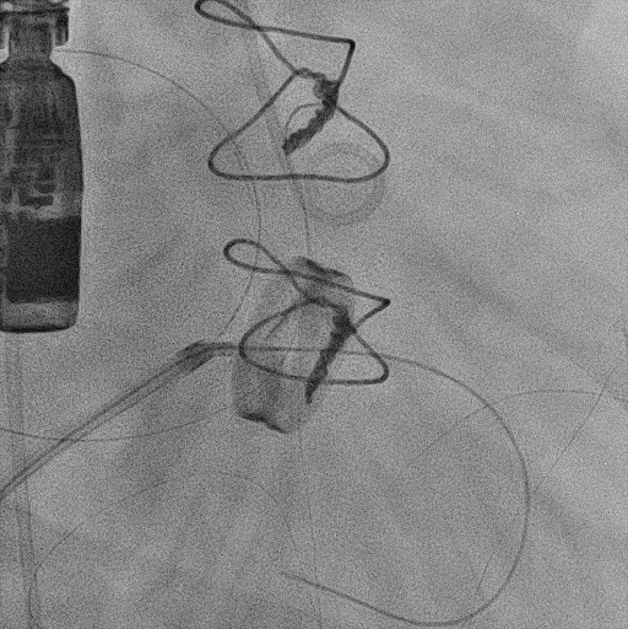
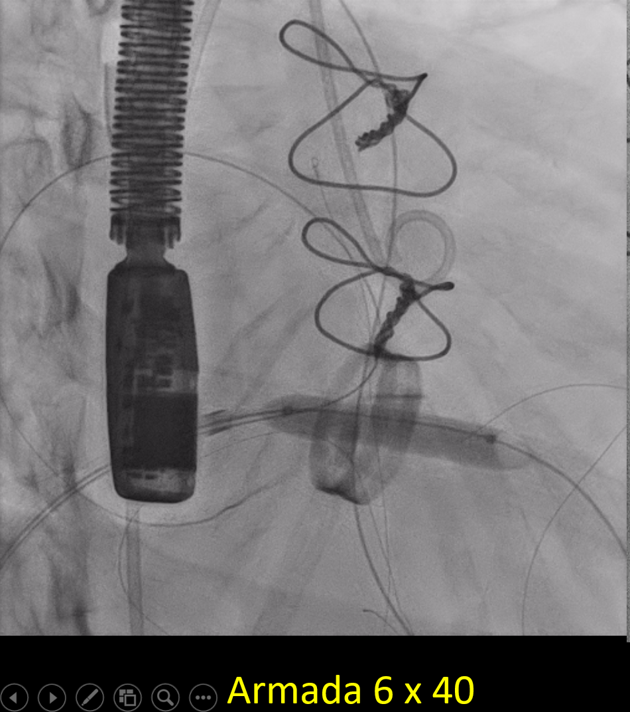
Since TLT was not possible and surgeon refused for emergencyTranscatheter valve disruption was planned. The issues involve in the procedure were
Case Summary
Take home message