Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_018
When to Fall Back and Fight Another Day: Management of Large Thrombus Burden in RCA Ectasia
By Abhirama Nofandra Putra, Heng Ge
Presenter
Abhirama Nofandra Putra
Authors
Abhirama Nofandra Putra1, Heng Ge2
Affiliation
Mandaya Royal Hospital Puri, Indonesia1, Renji Hospital, China2
View Study Report
CASE20251107_018
Coronary - ACS/AMI
When to Fall Back and Fight Another Day: Management of Large Thrombus Burden in RCA Ectasia
Abhirama Nofandra Putra1, Heng Ge2
Mandaya Royal Hospital Puri, Indonesia1, Renji Hospital, China2
Clinical Information
Relevant Clinical History and Physical Exam
A 49-year-old male presented with inferior MI, 20 hours from onset. He experienced recurrent chest pain upon admission. His cardiovascular risk factors are smoking and dyslipidemia. His hemodynamics are stable: blood pressure 134/78 mmHg, heart rate 88 bpm. His physical examination was unremarkable with no signs of heart failure nor hemodynamic disturbance.
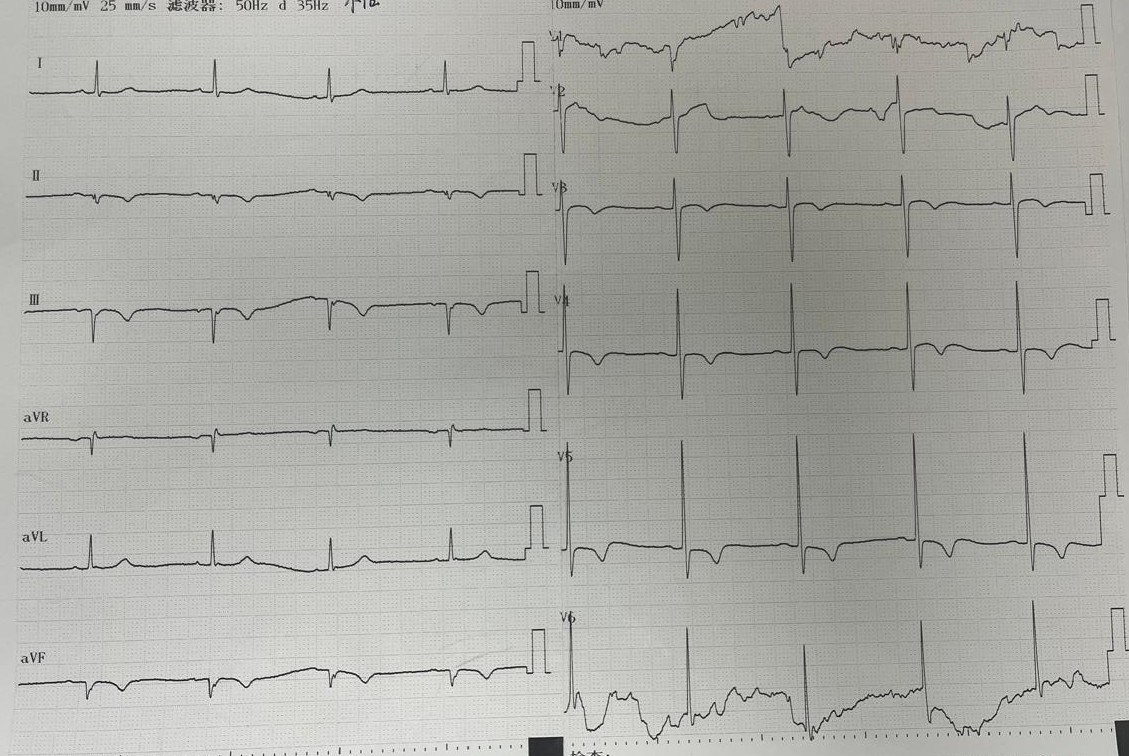
Relevant Test Results Prior to Catheterization
Laboratory examination revealed increased troponin, normal renal function, normal random blood glucose levels.
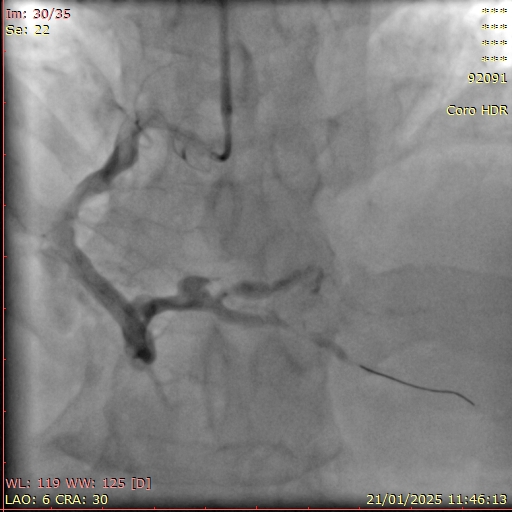
Relevant Catheterization Findings
Diagnostic coronary angiography was performed via right radial access using a 5F TIG diagnostic catheter:LM: short, no stenosisLAD: large calibre from ostial to mid LAD with intermediate stenosis at mid LAD, TIMI 3 flowLCx: non-dominant, large calibre, no stenosis, TIMI 3 flowRCA: dominant, very large calibre, diffuse ectasia, TIMI 2 flow with haziness suggestive of thrombus from distal RCA extending to PLB & PDA
 MOVIE-0002.mp4
MOVIE-0002.mp4
MOVIE-0003.mp4
MOVIE-0005.mp4
Interventional Management
Procedural Step
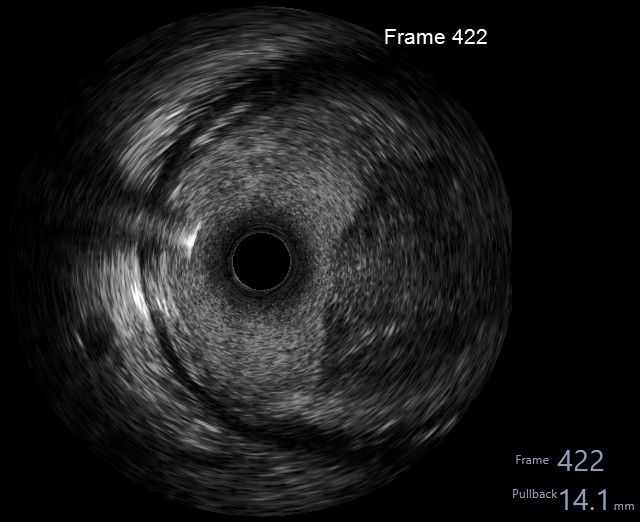
Index procedure:Right radial access with SAL 0.75/6F guide and 6F guide extension catheter. Wiring succeeded with Fielder XTR. Sequential predilation with 2.5/15 mm SC balloon, followed with aspiration thrombectomy & intracoronary injections of tirofiban & fasudil via the thrombectomy catheter. Evaluation angiography showed residual large thrombus burden. IVUS catheter had a significant bias due to the large vessel calibre, it could only reach as far as distal RCA. IVUS revealed heavy burden of consolidated thrombus in distal RCA with diffuse ectasia. Predilation with 3.0/15 mm NC balloon and further intracoronary injections of tirofiban via guide catheter still produced a significant residual thrombus burden, albeit with a slightly better distal flow. Deferred stenting and put the patient on anticoagulant on top of DAPT.
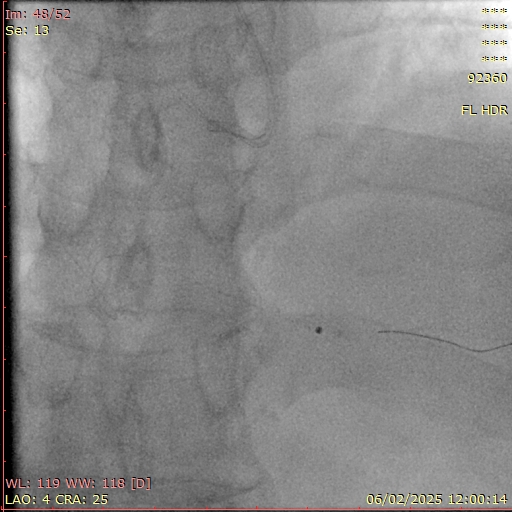
Repeat procedure:Repeat procedure was performed 2 weeks after the index procedure. We used right radial access with AL 0.75/7F guide and 7F guide extension catheter. Angiography revealed TIMI 2 flow to distal RCA, residual stenosis at distal RCA, residual haziness suggestive of thrombus in PDA. IVUS showed partially recanalized consolidated distal RCA thrombus with acceptable luminal size. ELCA was performed with 1.4 mm ELCA catheter under pure saline infusion technique followed by PCI (2.25/29 mm DES) to PDA. Final angiography showed TIMI 3 flow with residual stenosis at distal RCA. FFR LAD 0.84, no further intervention to LAD.
IVUS pullback index procedure.wmv
2nd procedure IVUS pullback.wmv
2nd PCI Final Angio.wmv
Repeat procedure:Repeat procedure was performed 2 weeks after the index procedure. We used right radial access with AL 0.75/7F guide and 7F guide extension catheter. Angiography revealed TIMI 2 flow to distal RCA, residual stenosis at distal RCA, residual haziness suggestive of thrombus in PDA. IVUS showed partially recanalized consolidated distal RCA thrombus with acceptable luminal size. ELCA was performed with 1.4 mm ELCA catheter under pure saline infusion technique followed by PCI (2.25/29 mm DES) to PDA. Final angiography showed TIMI 3 flow with residual stenosis at distal RCA. FFR LAD 0.84, no further intervention to LAD.
Case Summary
Acute coronary syndrome in coronary artery ectasia is a challenging clinical scenario: heavy thrombus burden, distal embolization, slow & stagnant flow, discrepancy in device sizing, difficulty in device delivery.
Intracoronary imaging has an important role in determining vessel anatomy and the pathophysiological basis of acute coronary syndrome in coronary ectasia.
Pharmacological treatment remains the mainstay of therapy. However, thrombus aspiration might be useful in case of acute coronary syndrome precipitated by thrombosis in the dilated arterial segment. ELCA is an available adjunct to debulk thrombus through its photomechanical, photothermal, photochemical effects.
Intracoronary imaging has an important role in determining vessel anatomy and the pathophysiological basis of acute coronary syndrome in coronary ectasia.
Pharmacological treatment remains the mainstay of therapy. However, thrombus aspiration might be useful in case of acute coronary syndrome precipitated by thrombosis in the dilated arterial segment. ELCA is an available adjunct to debulk thrombus through its photomechanical, photothermal, photochemical effects.