Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_017
When Trauma Masks Infarction: A Case of LAD Occlusion Presenting as Anterior STEMI After Blunt Chest Impact in a Young Adult
By Lutfi Hafiz Zunardi
Presenter
Lutfi Hafiz Zunardi
Authors
Lutfi Hafiz Zunardi1
Affiliation
Sunan Kalijaga General Hospital, Indonesia1
View Study Report
CASE20251107_017
Coronary - ACS/AMI
When Trauma Masks Infarction: A Case of LAD Occlusion Presenting as Anterior STEMI After Blunt Chest Impact in a Young Adult
Lutfi Hafiz Zunardi1
Sunan Kalijaga General Hospital, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
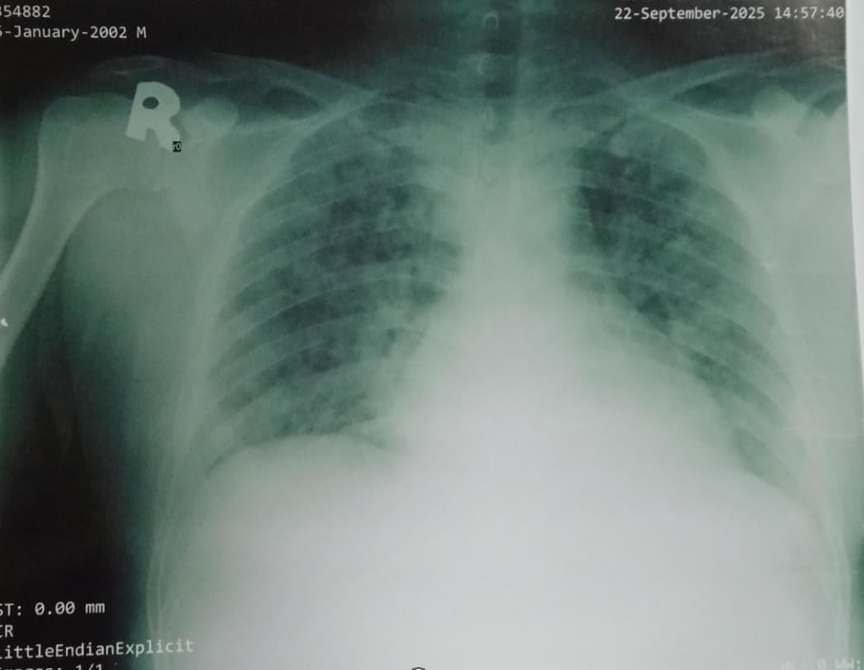
A 23-year-old heavy smoker presented after a motorcycle crash with direct chest impact on the handlebar. Initially admitted under orthopedic care for suspected skeletal injury, he developed worsening epigastric and substernal chest pain with dyspnea and impending respiratory failure, requiring ICU admission and anesthesiology evaluation. Both parents died of myocardial infarction; his father was a heavy smoker with hypertension and diabetes.
Relevant Test Results Prior to Catheterization
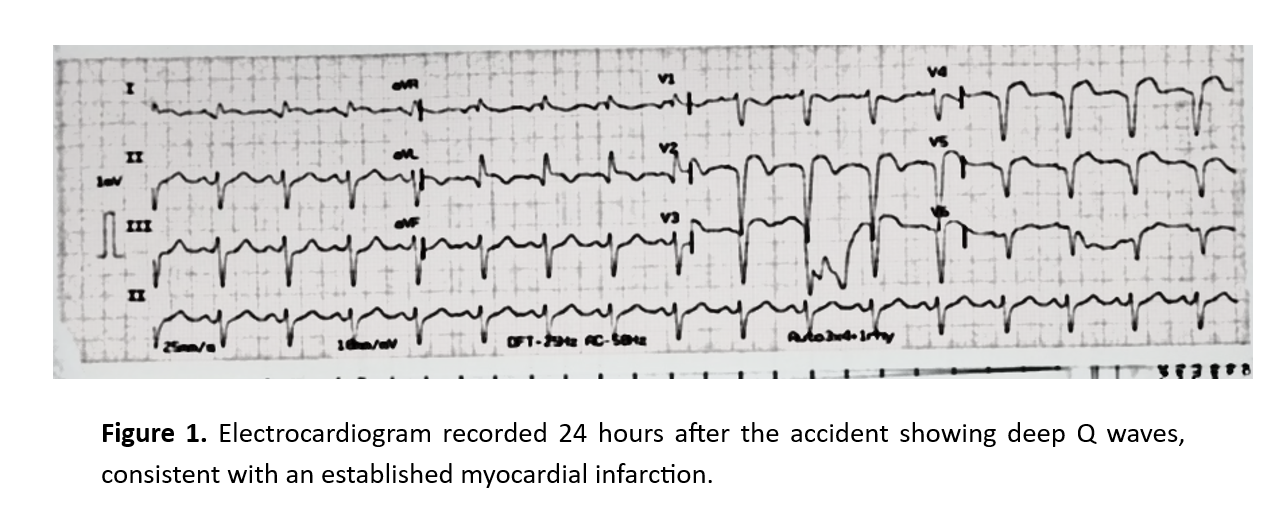
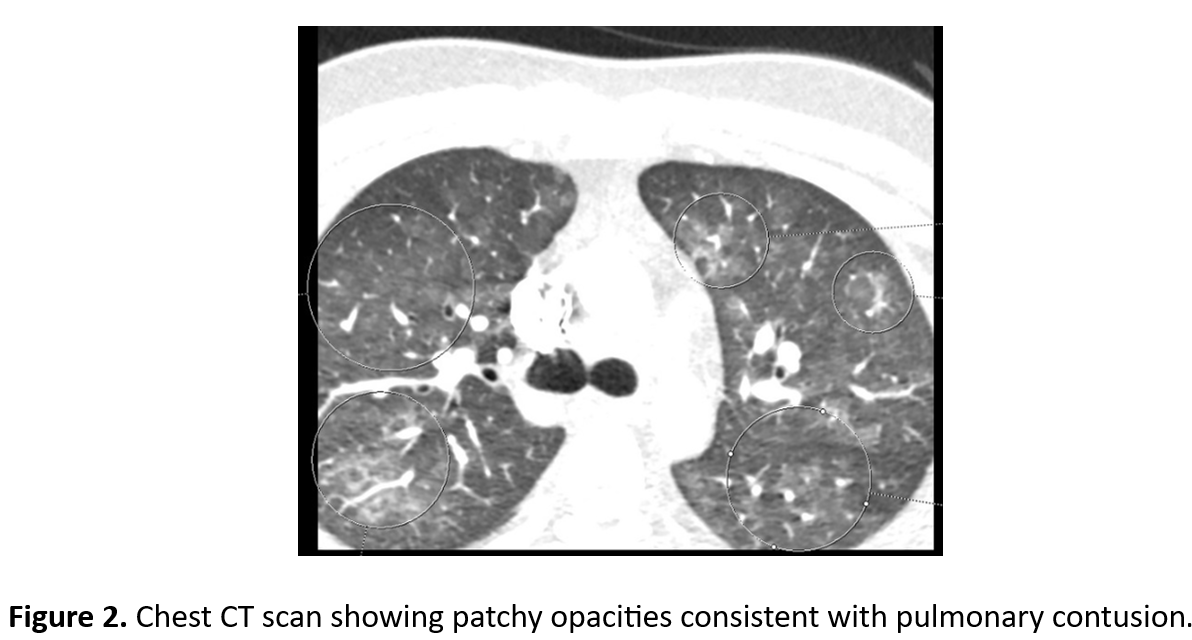
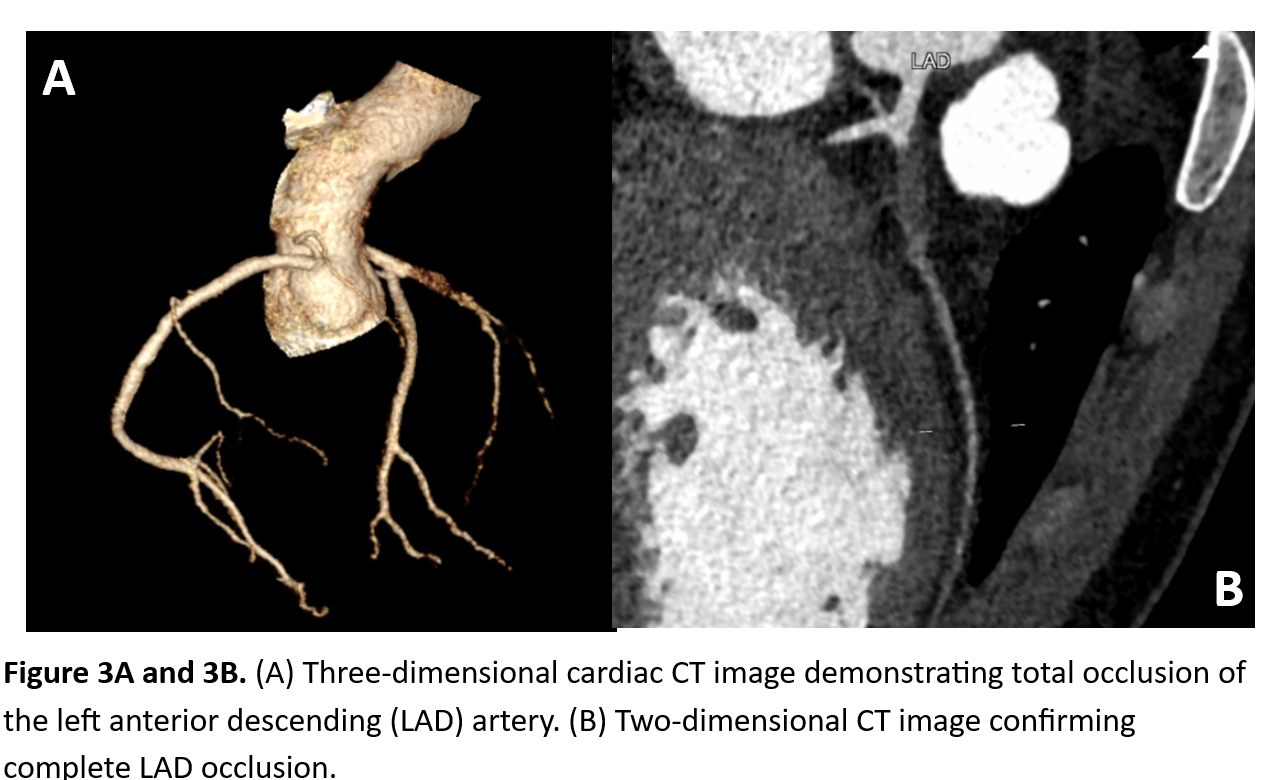
STEMI was initially unrecognized, and no ECG was performed for over 24 hours. As symptoms worsened, ECG showed anterior STEMI and Troponin I was elevated. Echo revealed LVEF 45% with akinetic mid–apical LV segments. Due to respiratory distress, myocarditis or contusion was suspected. Cardiac CT confirmed total LAD occlusion. The patient received Fondaparinux, aspirin 300 mg, and clopidogrel 300 mg before PPCI.
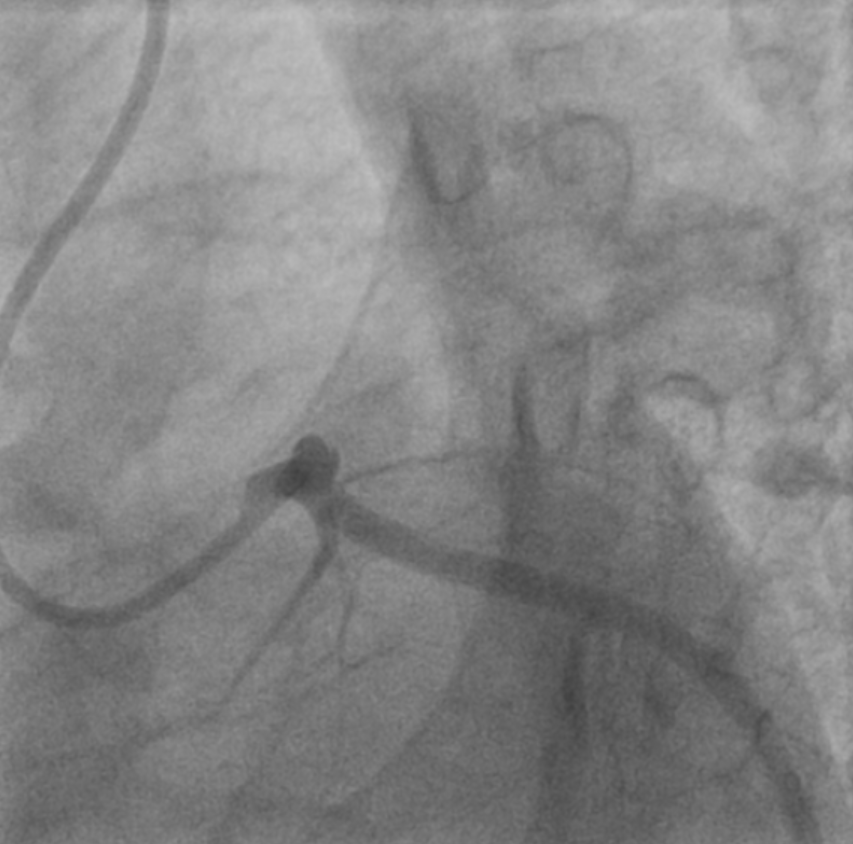
Relevant Catheterization Findings
Coronary angiography via rightradial access confirmed acute total occlusion of the proximal to mid LAD, whileLCx and RCA were patent. The lesion showed a thrombotic pattern consistent withplaque rupture likely triggered by blunt trauma. No evidence of coronarydissection or aortic injury was observed, confirming STEMI rather thanmyocarditis or myocardial contusion.
 MOVIE-0005.mp4
MOVIE-0005.mp4
MOVIE-0006.mp4
Interventional Management
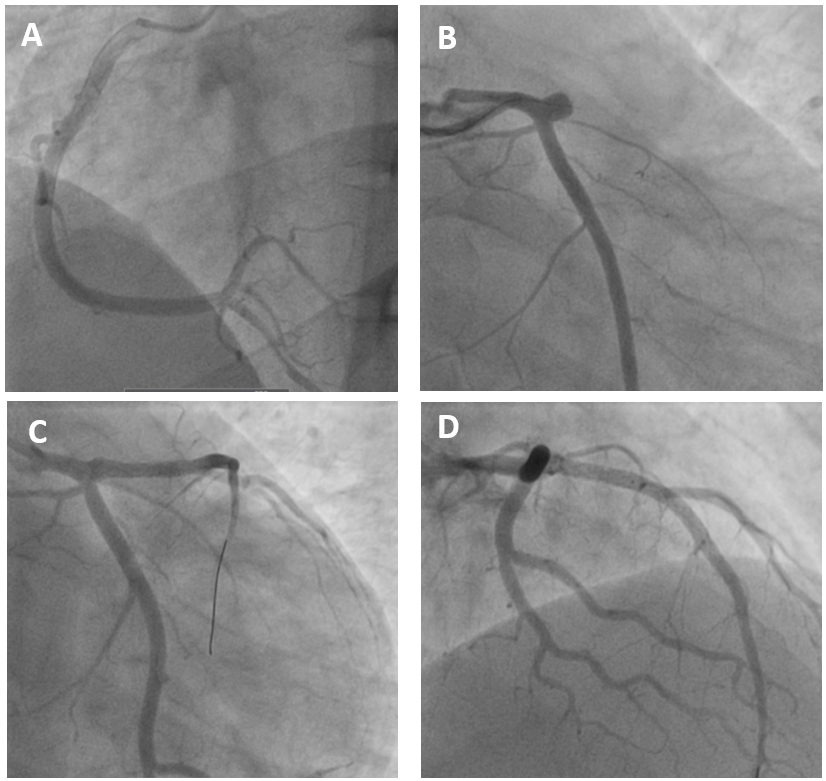
Procedural Step
Primary percutaneous coronaryintervention (PPCI) was performed via right radial artery access. A 6 Fr Tigercatheter was used for diagnostic angiography, followed by a 6 Fr XB 3.5 guidingcatheter for intervention. The LAD lesion was crossed with a floppy guidewireand pre-dilated using a semi-compliant balloon. Two drug-eluting stents (DES)were implanted: 3.5 × 20 mm in the proximal LAD and 3.0 × 30 mm in the mid LAD.Post-dilatation was performed to optimize stent expansion and apposition. Finalangiography showed TIMI 3 flow with no residual stenosis or dissection. Thepatient was started on dual antiplatelet therapy (aspirin and ticagrelor),statins, and beta-blockers. Recovery was uneventful, and he was discharged instable condition.
MOVIE-0003.mp4
MOVIE-0004.mp4
Case Summary
This case demonstrates that bluntchest trauma can mask ACS, leading to delayed recognition of STEMI in a youngadult. Initial diagnostic uncertainty, including consideration of myocarditisor contusion, combined with the absence of an early ECG, postponed definitivetherapy. Once ACS was confirmed, prompt initiation of anticoagulation andprimary PCI proved lifesaving. This case emphasizes that all adult traumapatients presenting with chest pain, even young individuals, should undergoearly ECG screening, as blunt trauma may precipitate coronary plaque rupture orthrombosis. High clinical vigilance and early cardiac evaluation are essentialto prevent missed or delayed interventions.