Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_016
Impella-Assisted High-Risk PCI in a Patient With Recent Stroke and Myocardial Infarction: Navigating Hemodynamic and Access Challenges
By Jen Chueh Wu, Chih-Fan Yeh, Hsien-Li Kao
Presenter
Jen Chueh Wu
Authors
Jen Chueh Wu1, Chih-Fan Yeh1, Hsien-Li Kao1
Affiliation
National Taiwan University Hospital, Taiwan1
View Study Report
CASE20251107_016
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Impella-Assisted High-Risk PCI in a Patient With Recent Stroke and Myocardial Infarction: Navigating Hemodynamic and Access Challenges
Jen Chueh Wu1, Chih-Fan Yeh1, Hsien-Li Kao1
National Taiwan University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
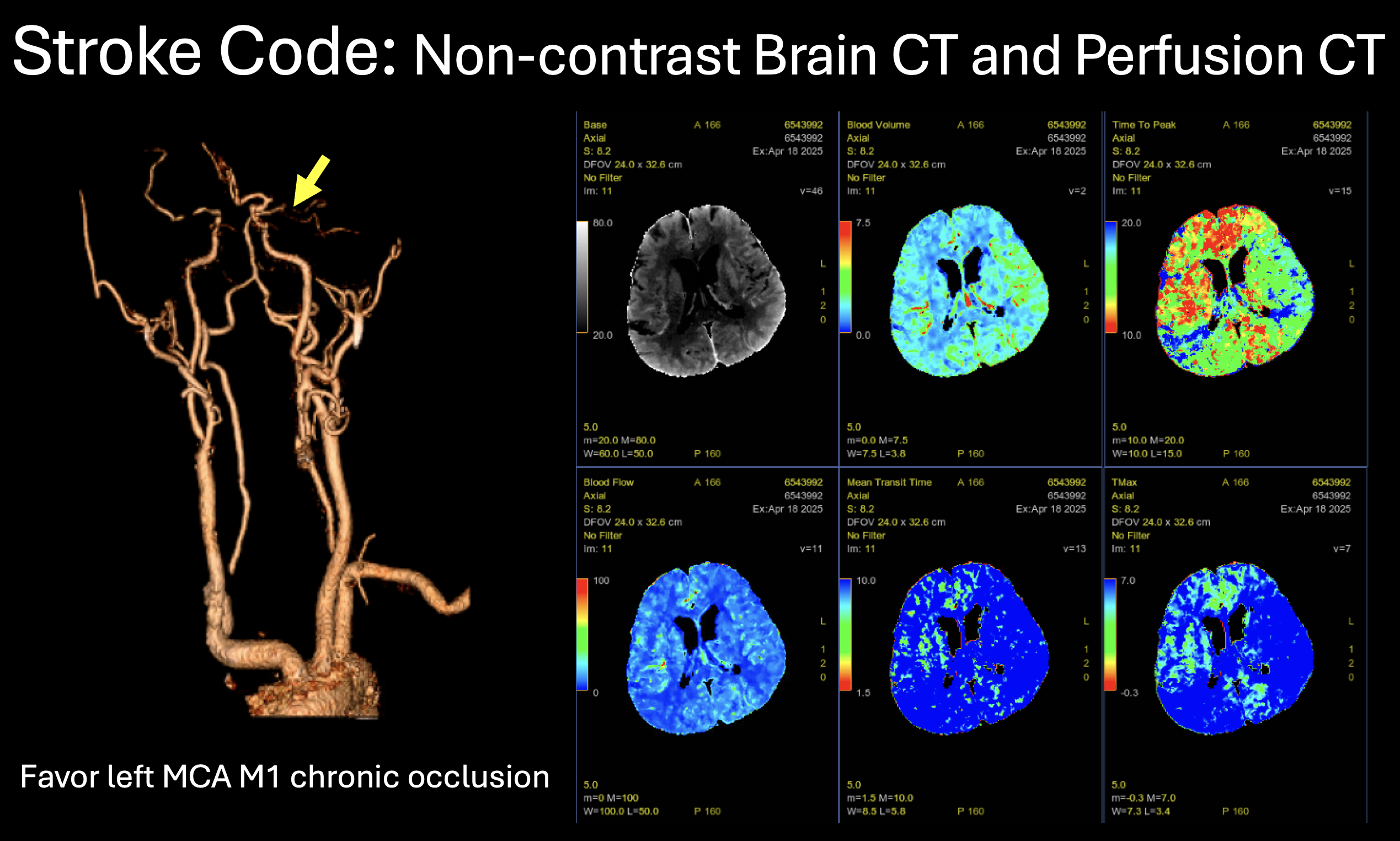
An 82-year-old man with hypertension presented with acute-onset aphasia and right arm weakness for 3 hours. Right foot was red, swollen, and tender. He had a fever of 38°C and was relatively hypotensive (100/64 mmHg, baseline 160 mmHg). A stroke code was activated. Emergent brain imaging showed no hemorrhage but chronic left MCA occlusion. The neurological deficit improved after CT, suggesting a transient ischemic attack. However, acute chest pain then occurred, prompting cardiac evaluation.
Relevant Test Results Prior to Catheterization
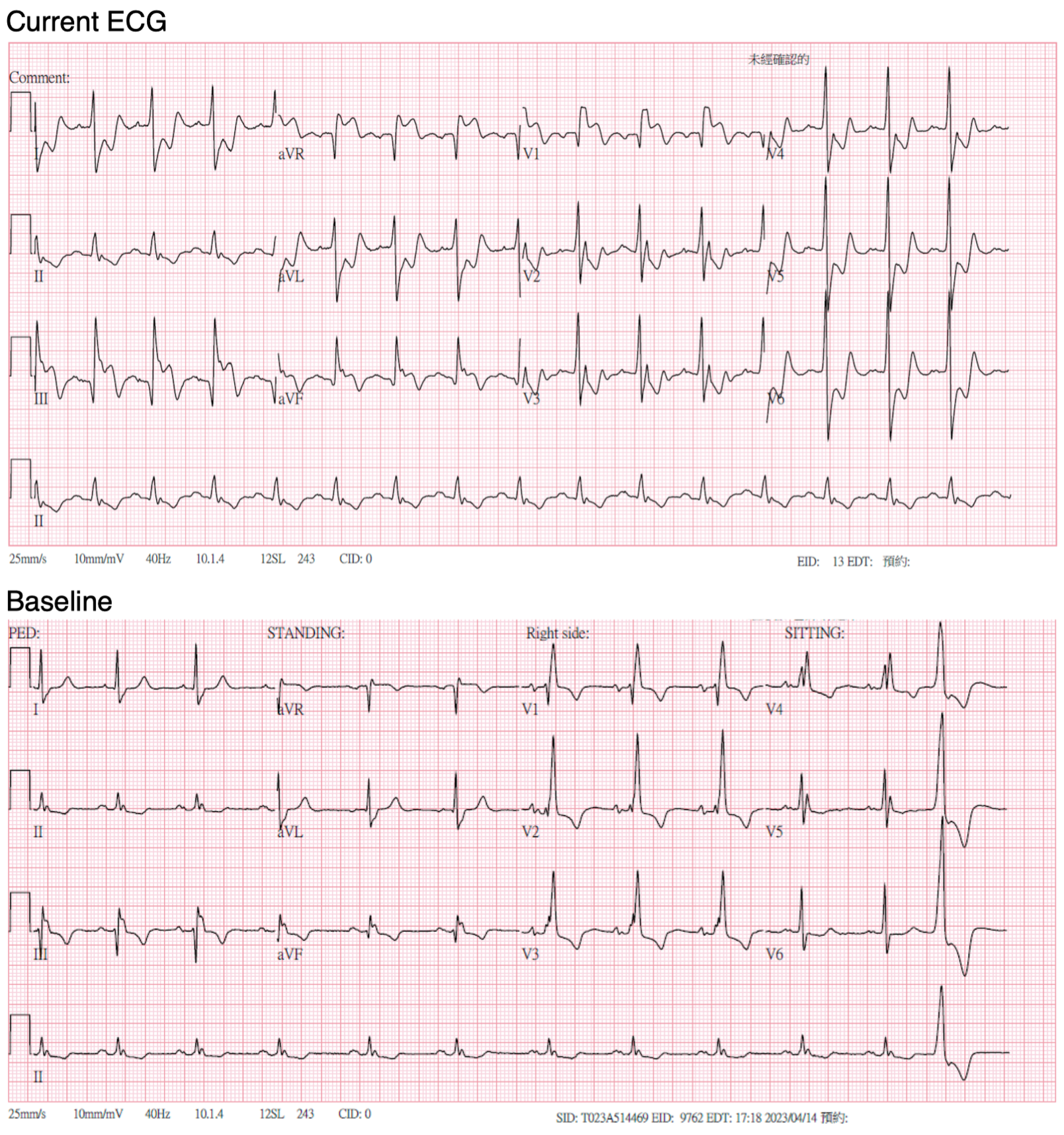
Electrocardiography suggested an inferior-posterior STEMI with probable left main equivalent. Echocardiography showed preserved left ventricular ejection fraction with regional wall motion abnormalities. Chest X-ray showed cardiomegaly with mild pulmonary congestion. Laboratory results revealed normal hemoglobin (16.3 g/dL), leukocytosis (26.09 × 10³/μL, segmented neutrophils 88.5%), elevated creatinine (2.04 mg/dL), high-sensitivity troponin T (37.66 ng/L) and lactate (2.68 mmol/L).

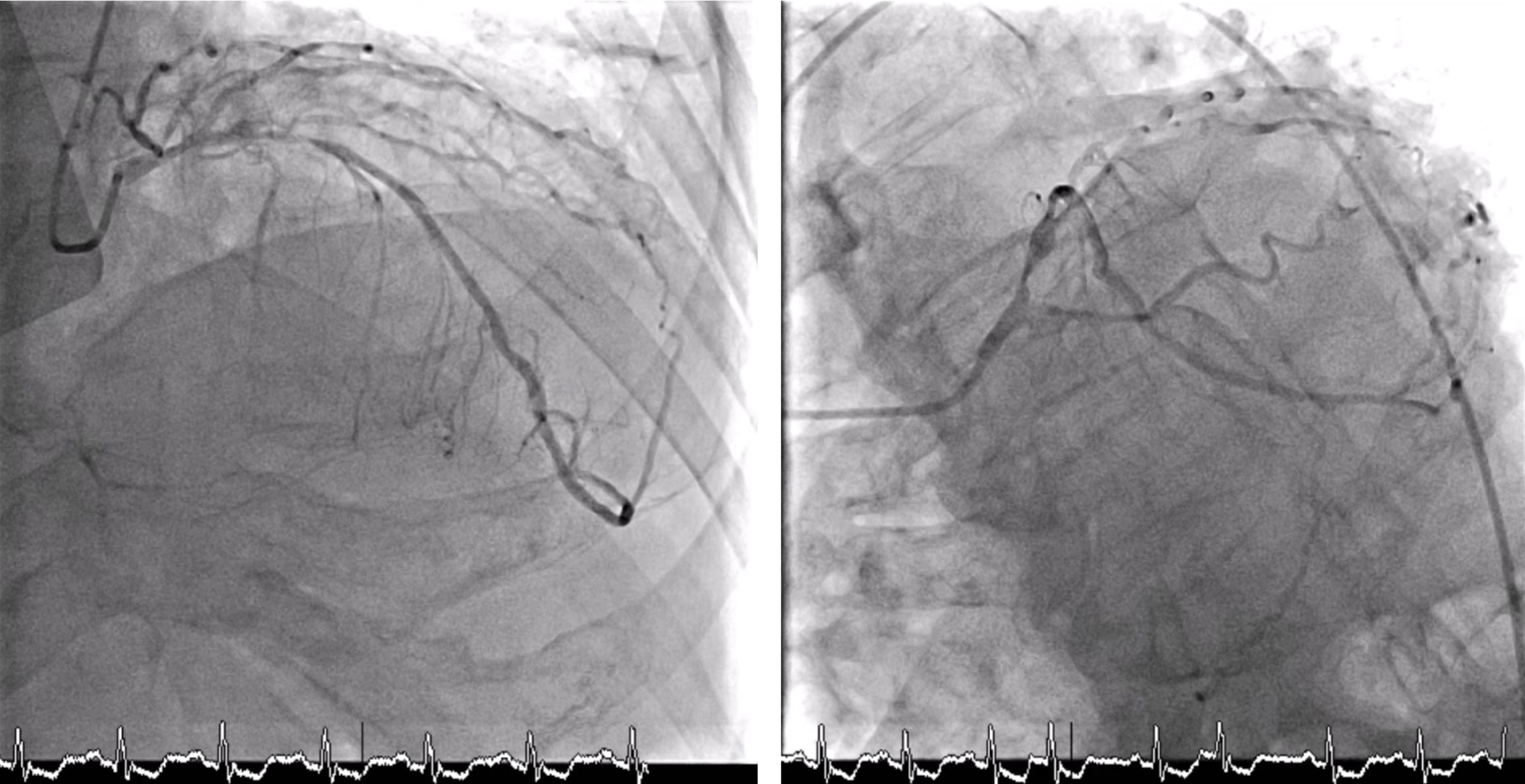
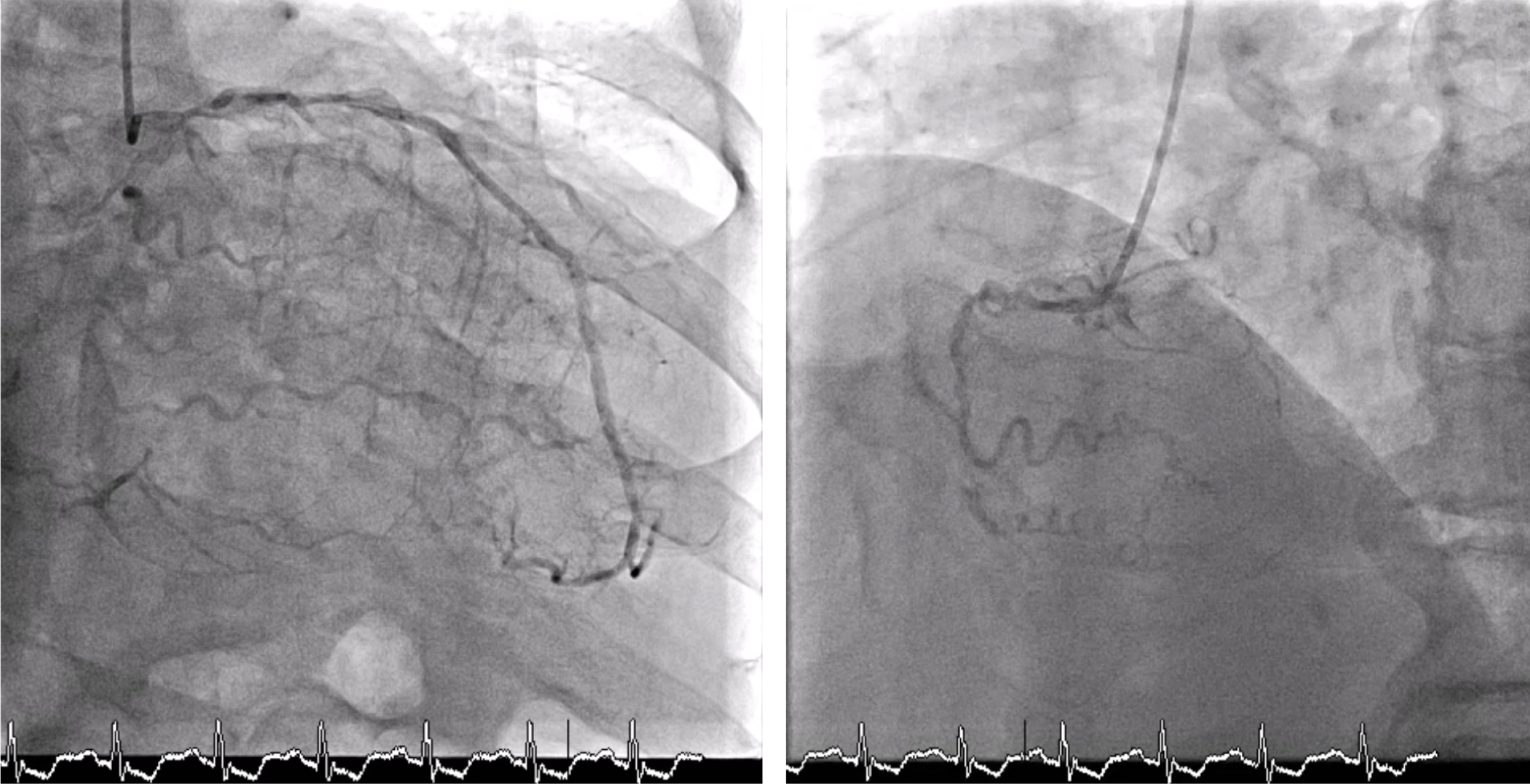
Relevant Catheterization Findings
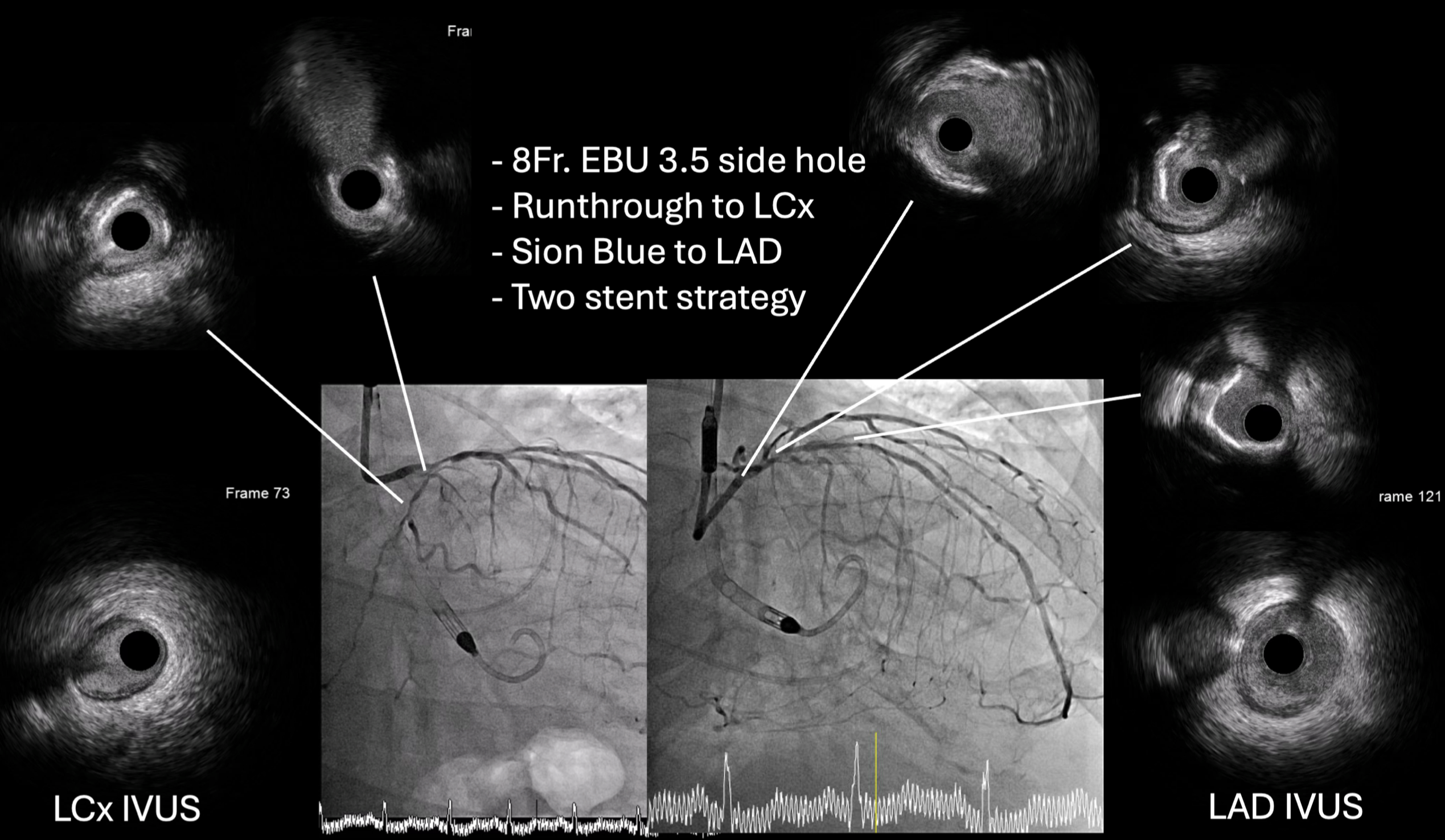
- LM: Bifurcation lesion (medina 0, 1, 1)
Interventional Management
Procedural Step
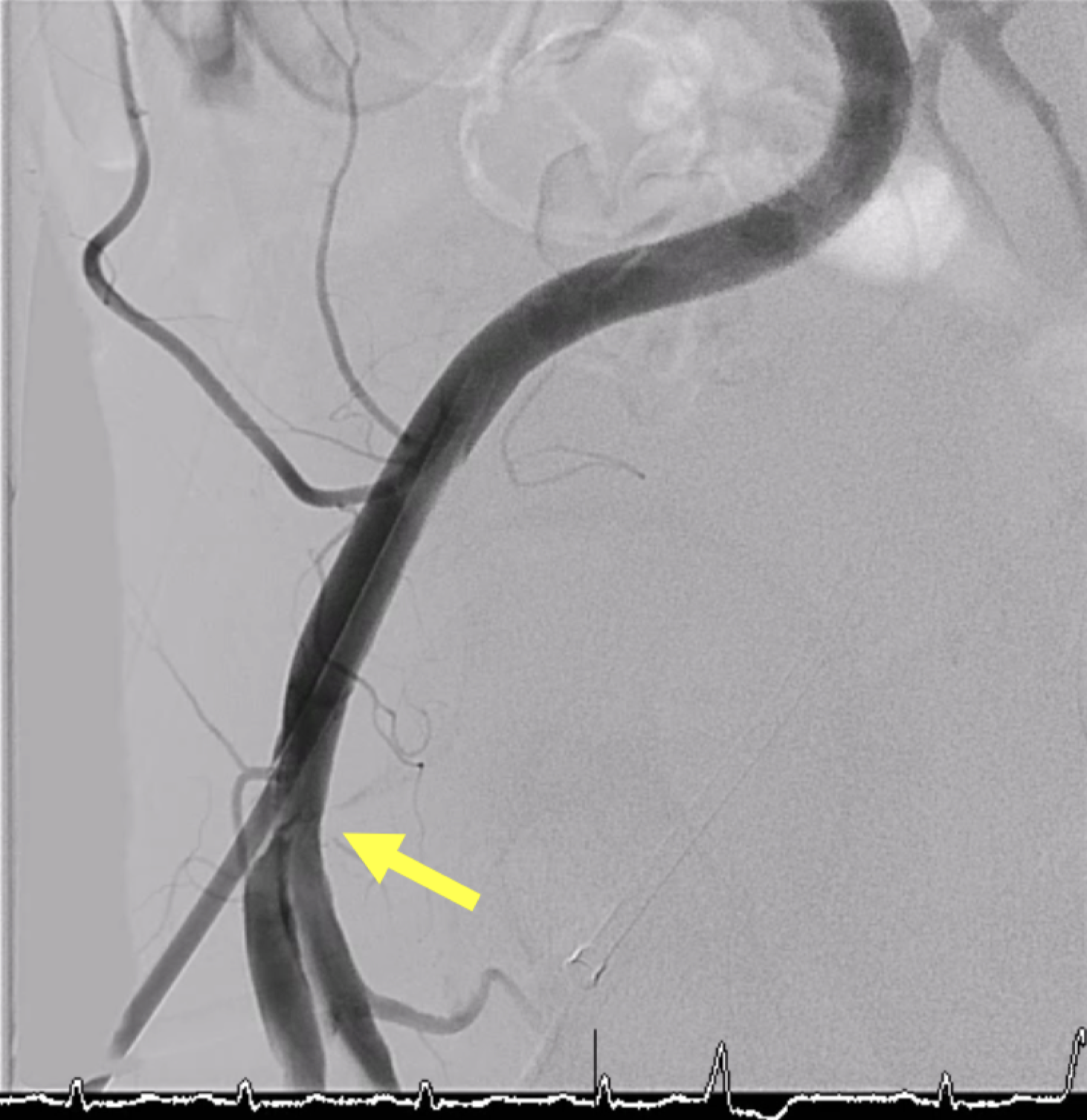
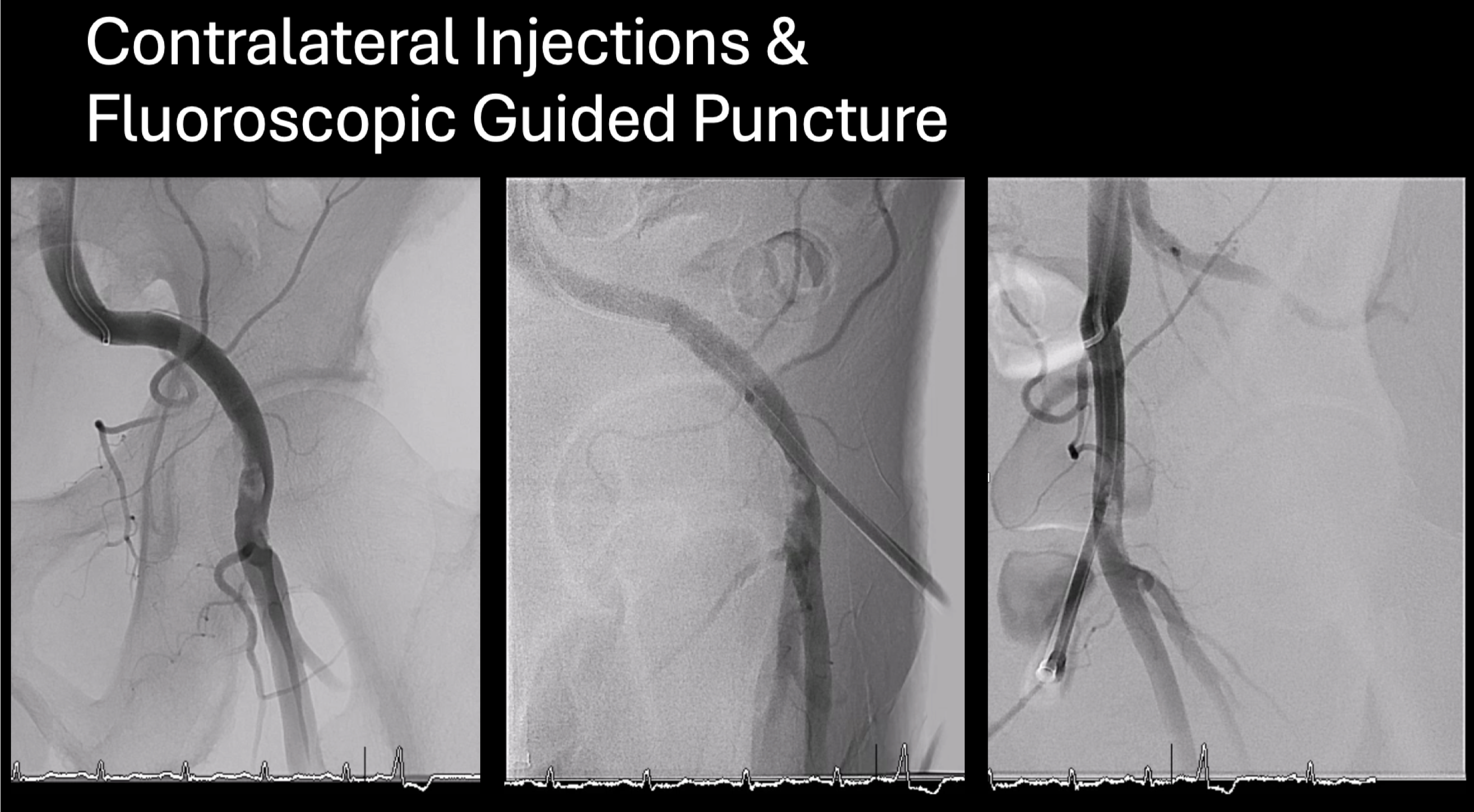
Vascular duplex was performed instead of CT for large-bore access evaluation due to acute kidney injury, revealing severe stenosis of the left common femoral artery. Despite this, an Impella CP® sheath was successfully inserted using contralateral injection and fluoroscopic-guided puncture, and the device was advanced into the left ventricle uneventfully. Initial hemodynamic data from the pulmonary artery catheter showed elevated pulmonary artery wedge pressure (32 mmHg), pulmonary hypertension (68/22 mmHg, mean 43 mmHg), and a low cardiac index (1.98 L/min/m²) without vasopressors or inotropes. The wedge pressure decreased to 23 mmHg after Impella insertion, demonstrating effective hemodynamic support.
Case Summary
High-risk percutaneous coronary intervention in patients with recent stroke and myocardial infarction remains challenging, requiring precise planning and individualized assessment. Proper preparation for large-bore access—using CT, duplex imaging, contralateral injection, and fluoroscopic or ultrasound guidance—can reduce access-site complications. The Impella CP® provides essential hemodynamic support during high-risk PCI, improving safety, stability, while reducing complications.