Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_015
Transcatheter Iatrogenic Ventricular Septal Perforation Closure After Surgical Aortic Mechanical Valve Replacement Through the Aortic Paravalvular Leakage
By Hidehiko Hara, Go Hashimoto, Yoshiyuki Yazaki, Hiroki Niikura, Kenji Makino, Nobutaka Ikeda, Keijiro Nakamura, Raisuke Iijima
Presenter
Hidehiko Hara
Authors
Hidehiko Hara1, Go Hashimoto1, Yoshiyuki Yazaki1, Hiroki Niikura1, Kenji Makino1, Nobutaka Ikeda1, Keijiro Nakamura1, Raisuke Iijima1
Affiliation
Toho University Ohashi Medical Center, Japan1
View Study Report
CASE20251107_015
Structural - Other Structural Interventions
Transcatheter Iatrogenic Ventricular Septal Perforation Closure After Surgical Aortic Mechanical Valve Replacement Through the Aortic Paravalvular Leakage
Hidehiko Hara1, Go Hashimoto1, Yoshiyuki Yazaki1, Hiroki Niikura1, Kenji Makino1, Nobutaka Ikeda1, Keijiro Nakamura1, Raisuke Iijima1
Toho University Ohashi Medical Center, Japan1
Clinical Information
Relevant Clinical History and Physical Exam
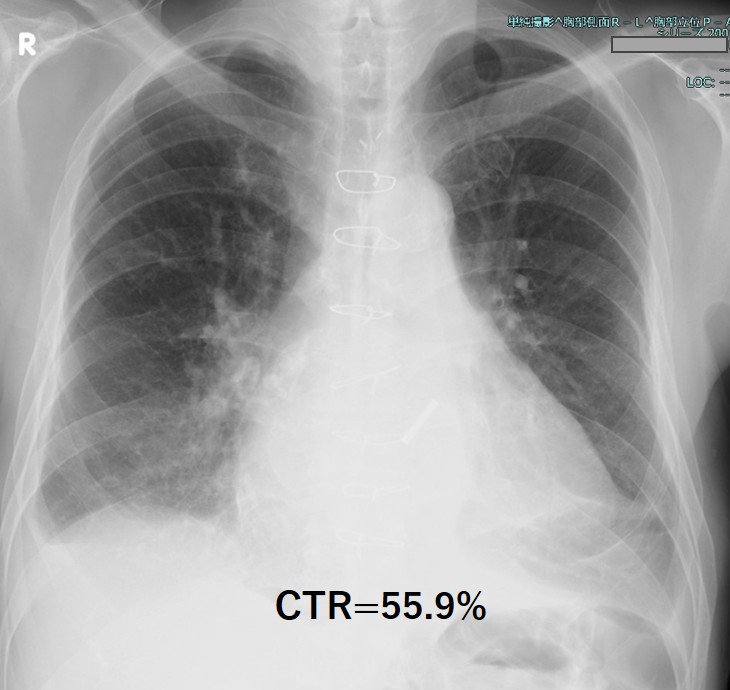
70 years old male with dyspnea on effort wasintroduced to our center for percutaneous ventricular septal perforation (VSP)closure. His past history revealed aortic valve replacement(AVR) 16 years agoand recent re-do AVR with mechanical valve due to the paravalvular leakage (PVL).Heart failure symptom was NYHA class 3. The auscultation revealed holo-systolicmurmur 3/6 at the left sternal border and regurgitant murmur at the right side,and also significant bilateral pretibial edema.

Relevant Test Results Prior to Catheterization
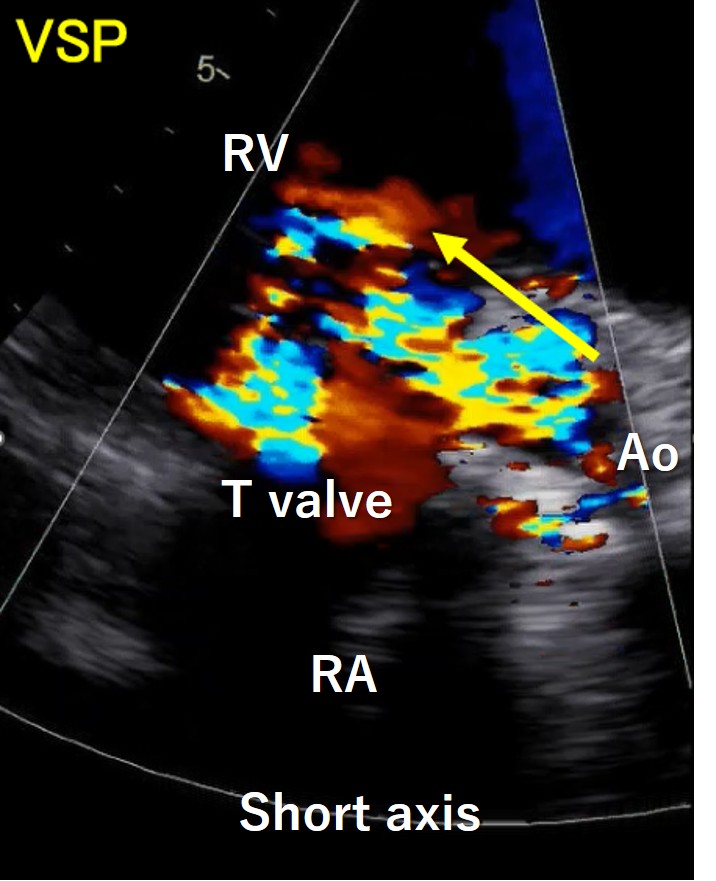
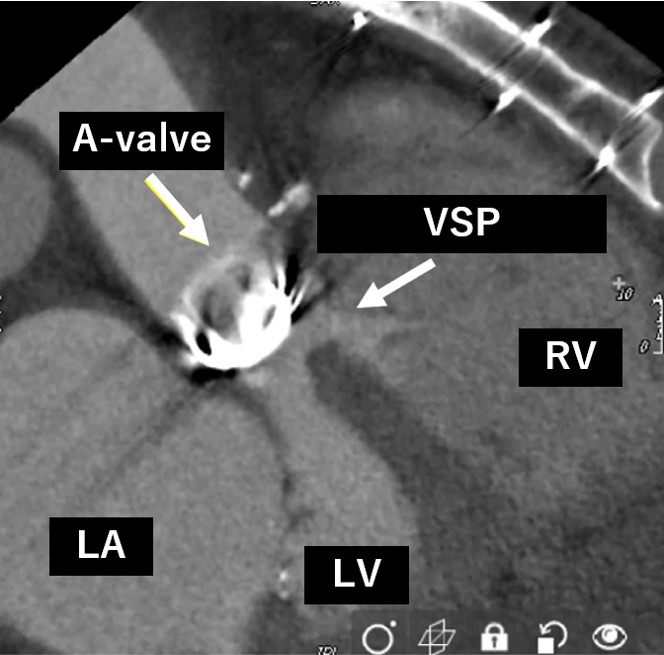
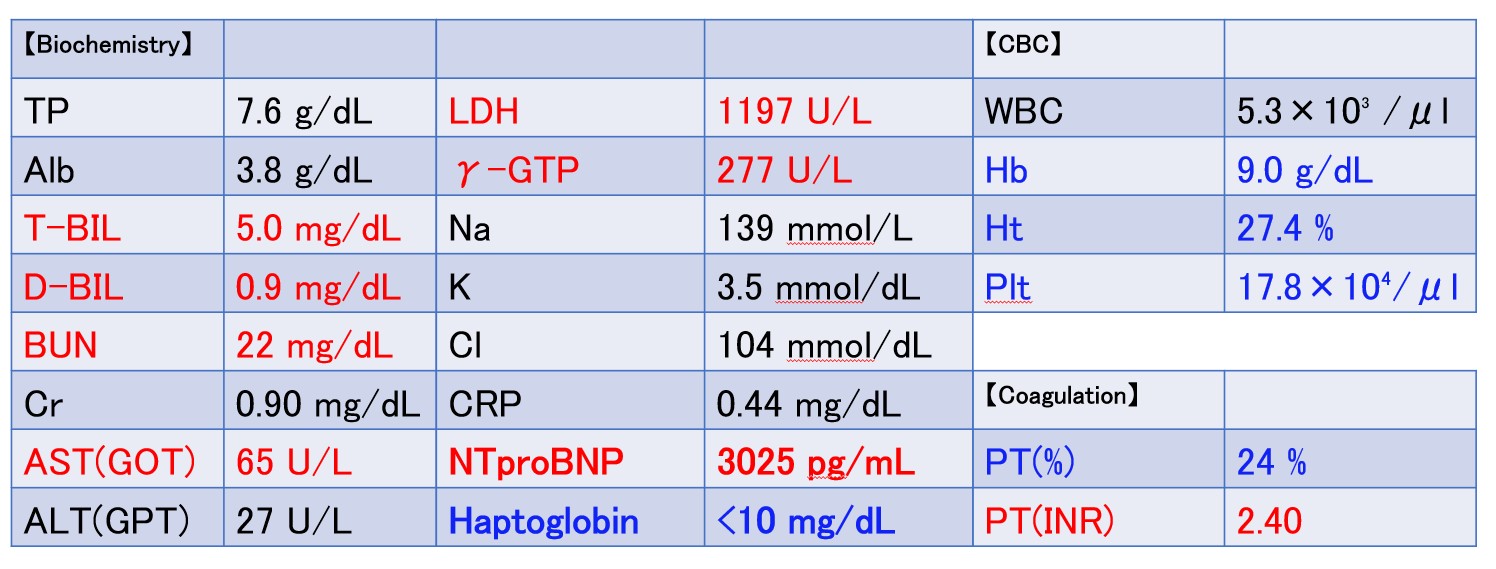
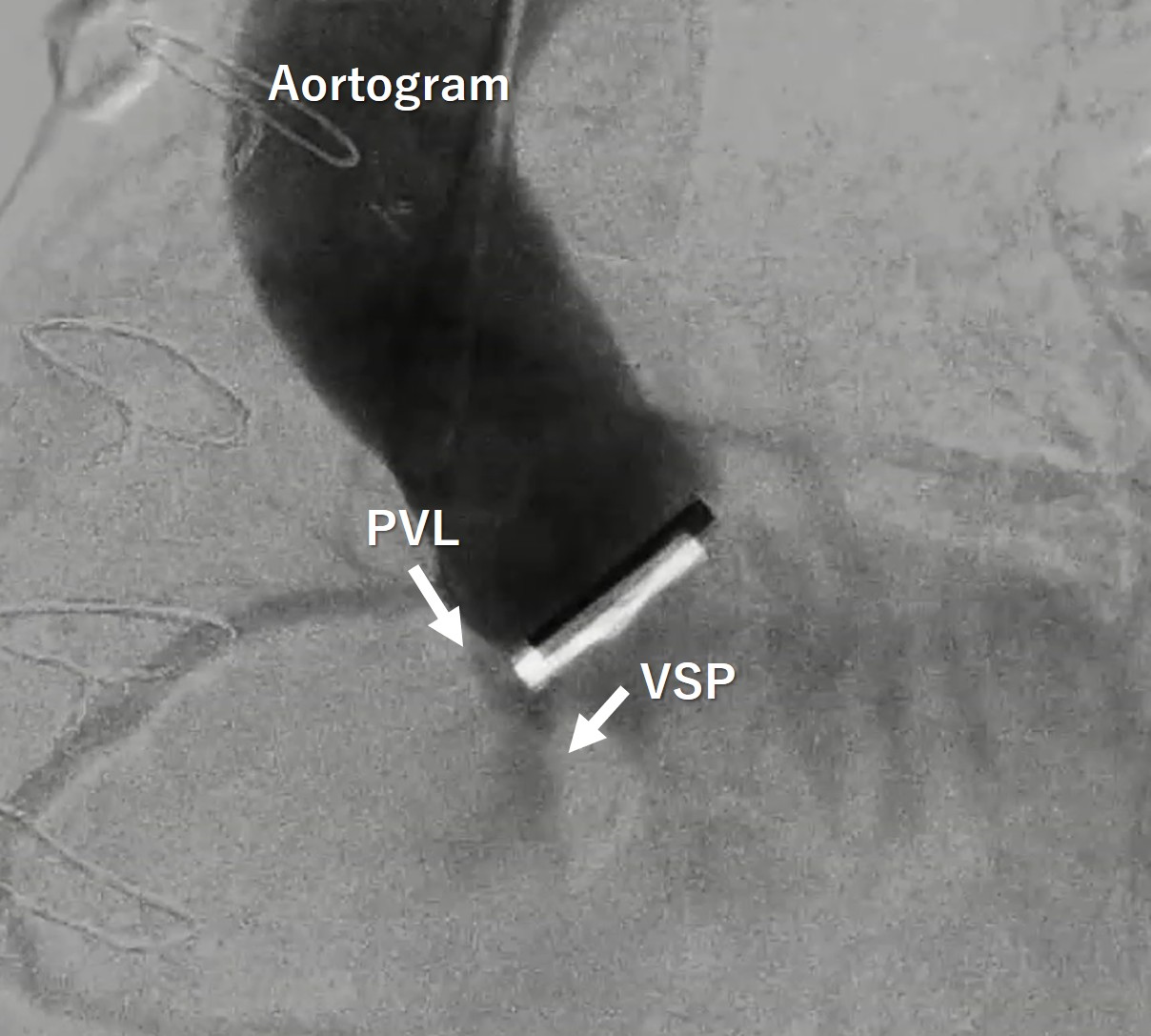
Blood tests showed an increase in totalbilirubin to 5.0 mg/dl, along with an increase in LDH and decreases in Hb andhaptoglobin, indicating hemolytic anemia. NTproBNP also increased to over 3000.The transthoracic echocardiogram showed the VSP at the membranous septum nearthe aortic PVL, and also moderate tricuspid regurgitation. Aortogram and CTscan demonstrated the severe aortic PVL with interventricular left to right shuntnearby.
Relevant Catheterization Findings
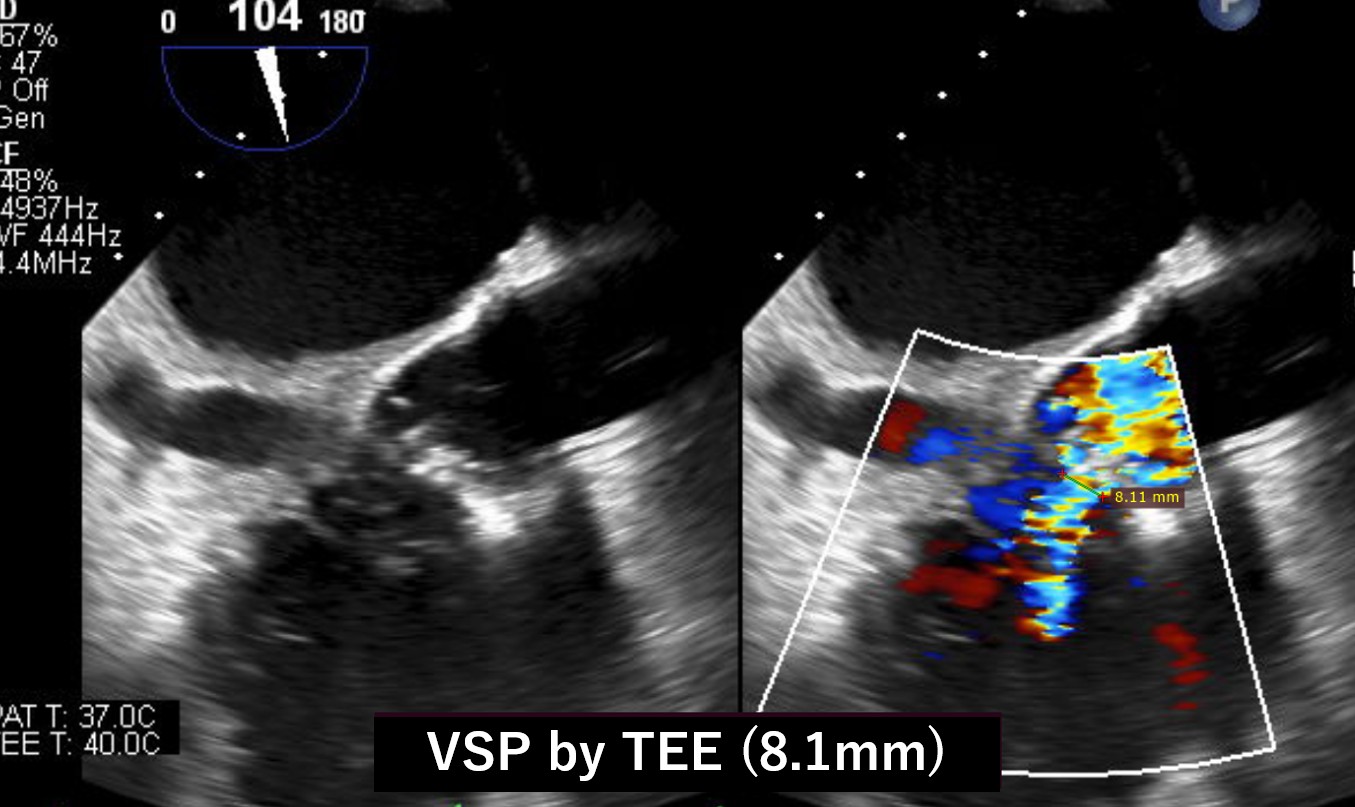
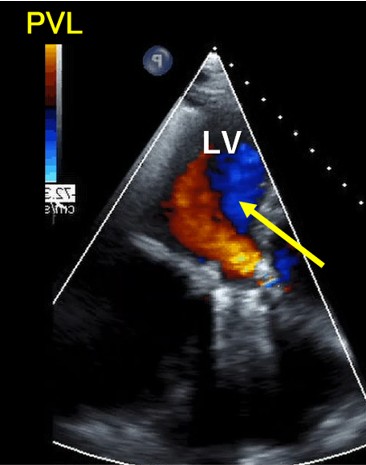
Our heart team decided to perform both VSP and PVL closure by transcatheter technique because of the previous multiple open-heart surgery with high surgical risk score. Before percutaneous VSP closure, the oximetry-run exams revealed Qp/Qs 1.3 but the transesophageal echo(TEE) showed the EROA of aortic PVL was 0.51 mm2 and the defect size was 10.5 x 5.4 mm which meant severe PVL. We also confirmed the defect size of VSP with TEE, and the size was 8.1mm.
Interventional Management
Procedural Step
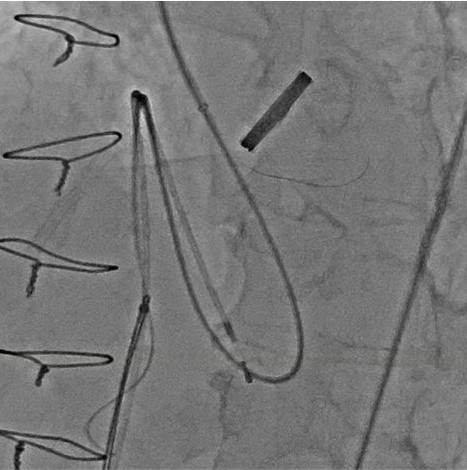
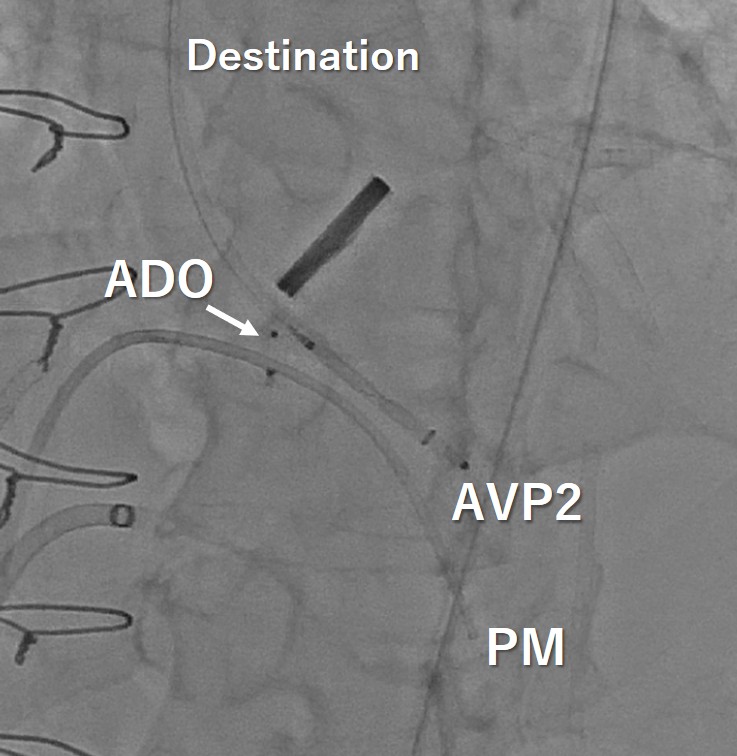
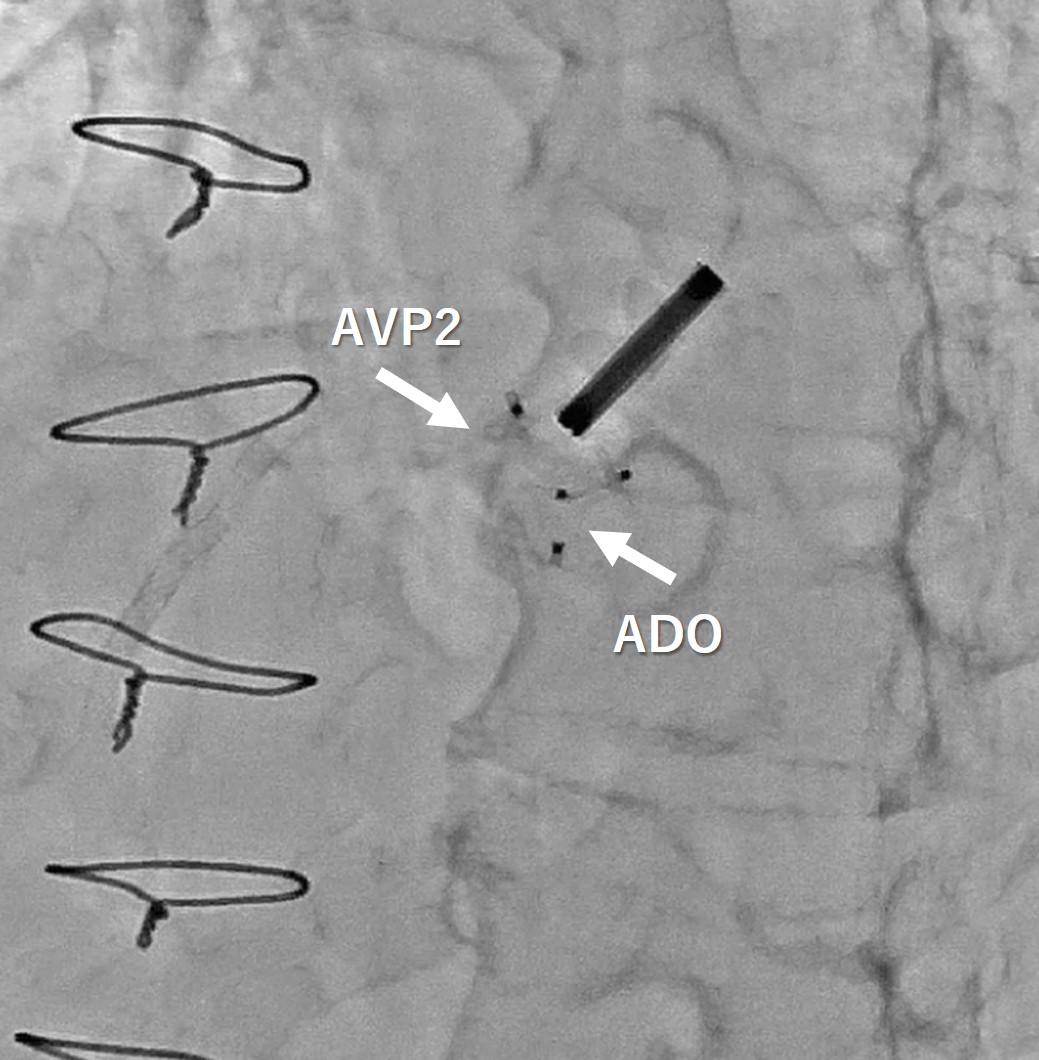
We performed this procedure under generalanesthesia with TEE. The first step was to close the VSP so that we manipulateda 5 Fr. Destination sheath with diagnostic JR4 catheter as mother and childtechnique. Inside of the system, 0,014-inch wire and microcatheter was advancedleft ventricle(LV) from aortic PVL. We turned the wire inside LV to access theVSP. We succeeded to have the wire advance to right ventricle(RV) through the LVand PVL. The next step was creating AV loop so that the 0.014 wire was snaredin the pulmonary artery and pulled out from right femoral vein. After creatingAV loop with 0.014 wire, the loop was exchanged to 0.035 wire and AMPLATZERDuct Occluder 6/4 was implanted into VSP. After closing VSP, we accessed insidethe PVL again and the wire was switched to super stiff one to advance theDestination sheath inside LV. Once the sheath was advanced in LV, 8mm AMPLATZERvascular plug 2 was deployed to close the PVL.
Case Summary
We experienced to close VSP after redosurgical AVR through the aortic PVL. The technique to close the VSP was as sameas the standard VSD closure, however the aortic valve was already replaced bythe mechanical valve, so that the procedure itself was more difficult thanusual but finally turned to success. The imaging guidance like TEE with meticulousattentions not to injure any structure inside the heart was necessary to makeit success to the patients with this kind of complicated structural heart disease.The patient condition got better and both leakages are still suppressed nicely evenafter one year from this procedure.