Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_014
IVUS-Guided Bilateral Iliac Recanalization for Leriche Syndrome: Precise Lumen Sizing and IMA-Sparing Stent Deployment
By Yu-Jou Wu, Shu-Han Lin, Hao-Yun Lo
Presenter
Yu-Jou Wu
Authors
Yu-Jou Wu1, Shu-Han Lin1, Hao-Yun Lo1
Affiliation
Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1
View Study Report
CASE20251107_014
Endovascular - Iliac / SFA Intervention
IVUS-Guided Bilateral Iliac Recanalization for Leriche Syndrome: Precise Lumen Sizing and IMA-Sparing Stent Deployment
Yu-Jou Wu1, Shu-Han Lin1, Hao-Yun Lo1
Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 65-year-old man with hypertension,hyperlipidemia, and type 2 diabetes mellitus had chronic bilateral leg painwith claudication for years. Peripheral arterial occlusive disease wasdiagnosed by ABI. Cilostazol and aspirin were initiated but later discontinuedbecause of intolerable skin lesions. Recurrent leg wounds persisted. Physicalexamination revealed bilateral leg hair loss and weak dorsalis pedis pulses.Imaging confirmed Leriche syndrome, and the patient was admitted forangioplasty.

Relevant Test Results Prior to Catheterization
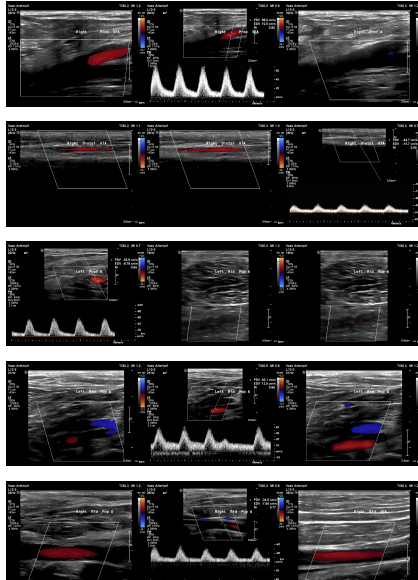
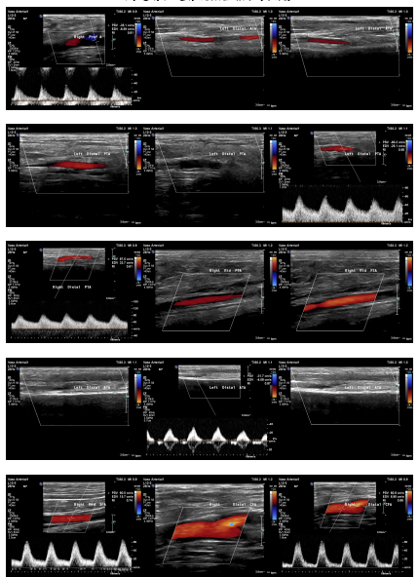
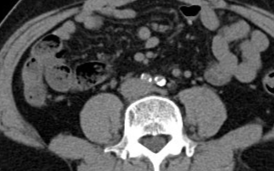
ABI measured on December 13, 2021, was 0.64on the right and 0.59 on the left. Duplex ultrasonography performed on August6, 2024, revealed monophasic flow in bilateral CFA, SFA, popliteal, ATA, andPTA arteries, favoring bilateral severe iliac artery disease. Subsequent CTangiography on November 15, 2024, demonstrated aortoiliac occlusive disease,without evidence of aneurysm or distal vessel obstruction. Laboratory databefore admission showed HbA1c 6.9% and LDL 76 mg/dL.

 05683262_001.AVI
05683262_001.AVI
Relevant Catheterization Findings
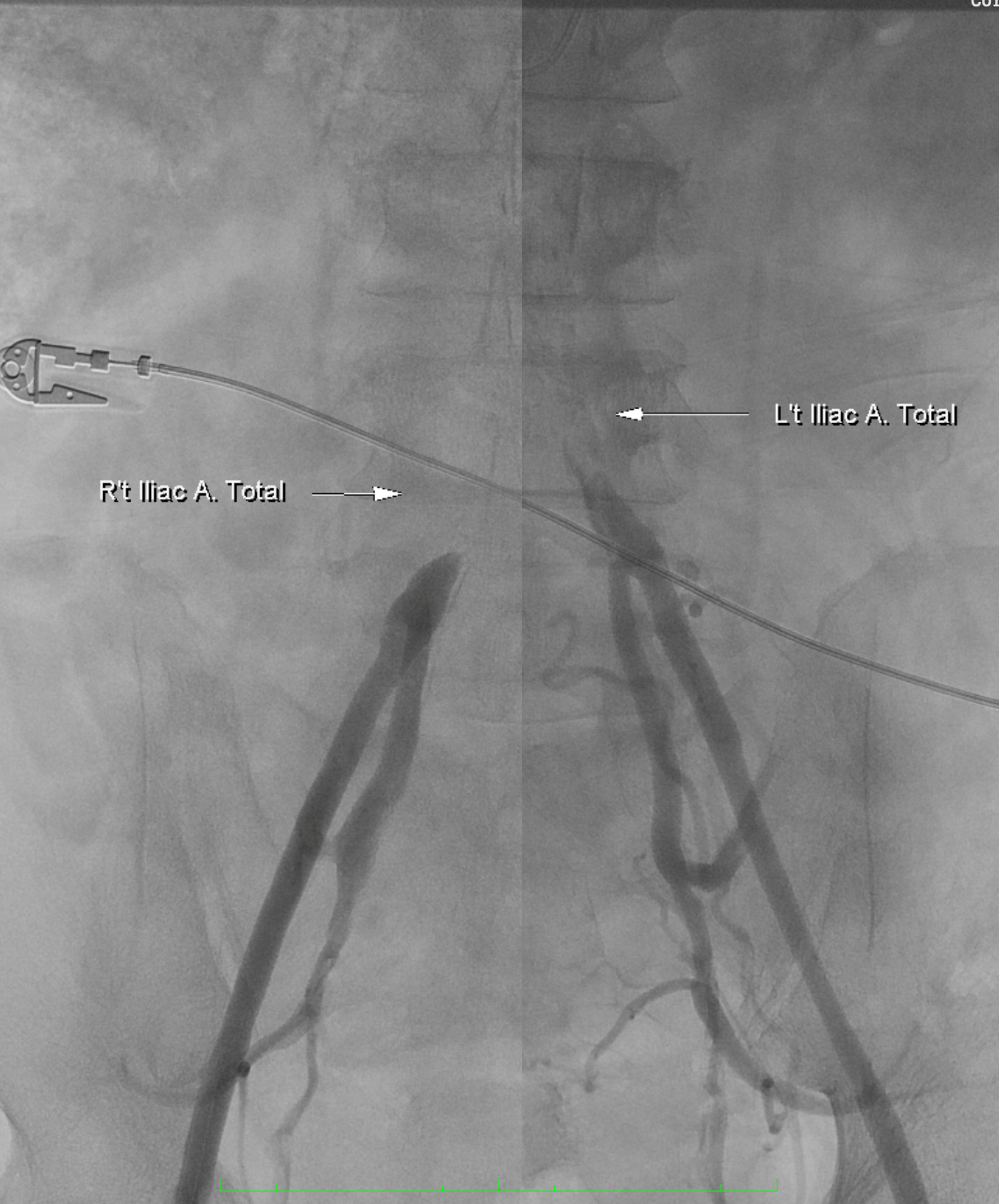
Diagnosticangiography revealed total occlusion of both common iliac arteries, while theexternal iliac arteries remained patent bilaterally. The lesions wereconsistent with aortoiliac occlusive disease (Leriche syndrome), and the distalflow was preserved via collateral circulation.
05683262_001.AVI
05683262_005.AVI
05683262_006.AVI
Interventional Management
Procedural Step
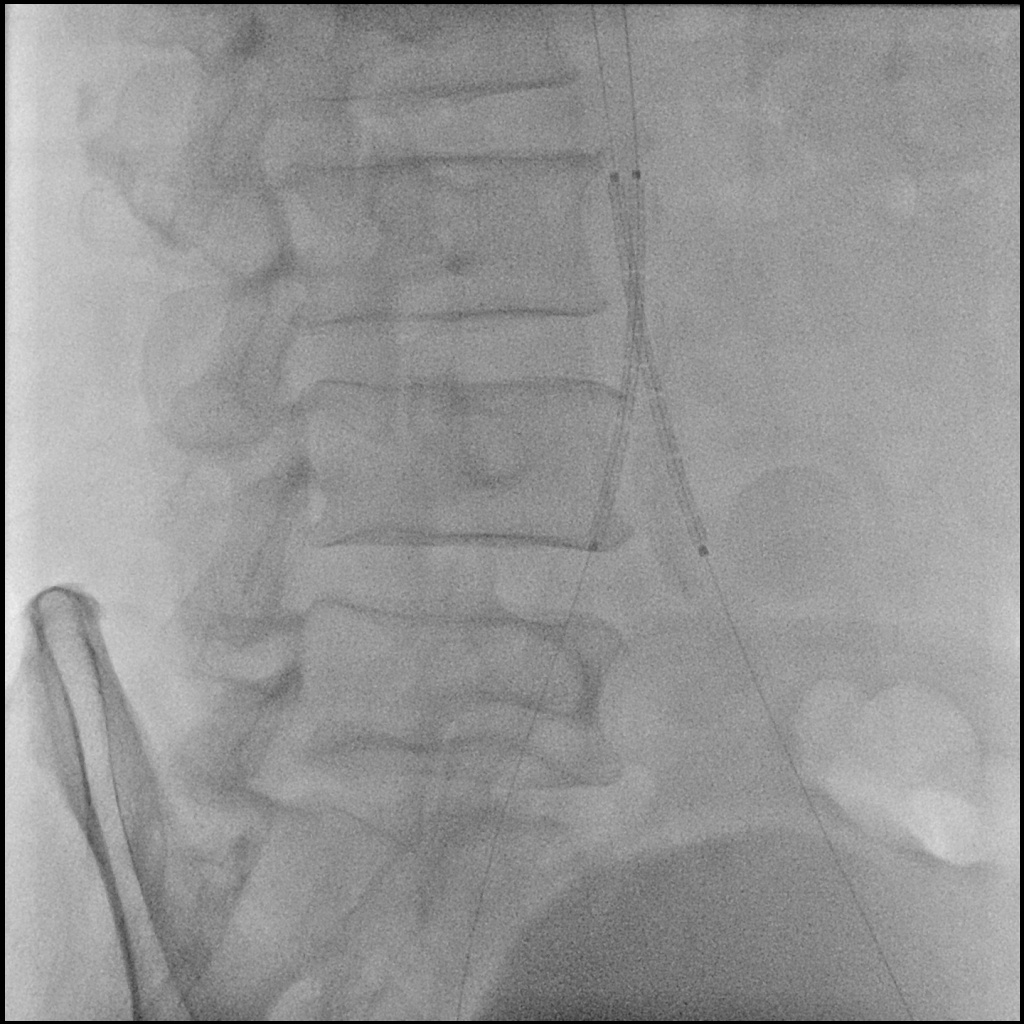
A 6F Mach1 MP guiding catheter waspositioned via aterial access. Wiring was performed sequentially with Gladius0.014″ and Halberd 0.014″ under NaviCross 0.018″ catheter support, then switched to an Astato XS 40 for bettercontrol. Using a CSI microcatheter, the 0.018″ system was exchanged for a 0.014″ wire to performIVUS. IVUS initially could not advance but succeeded after predilatation withan Ultraverse 2.0 balloon.
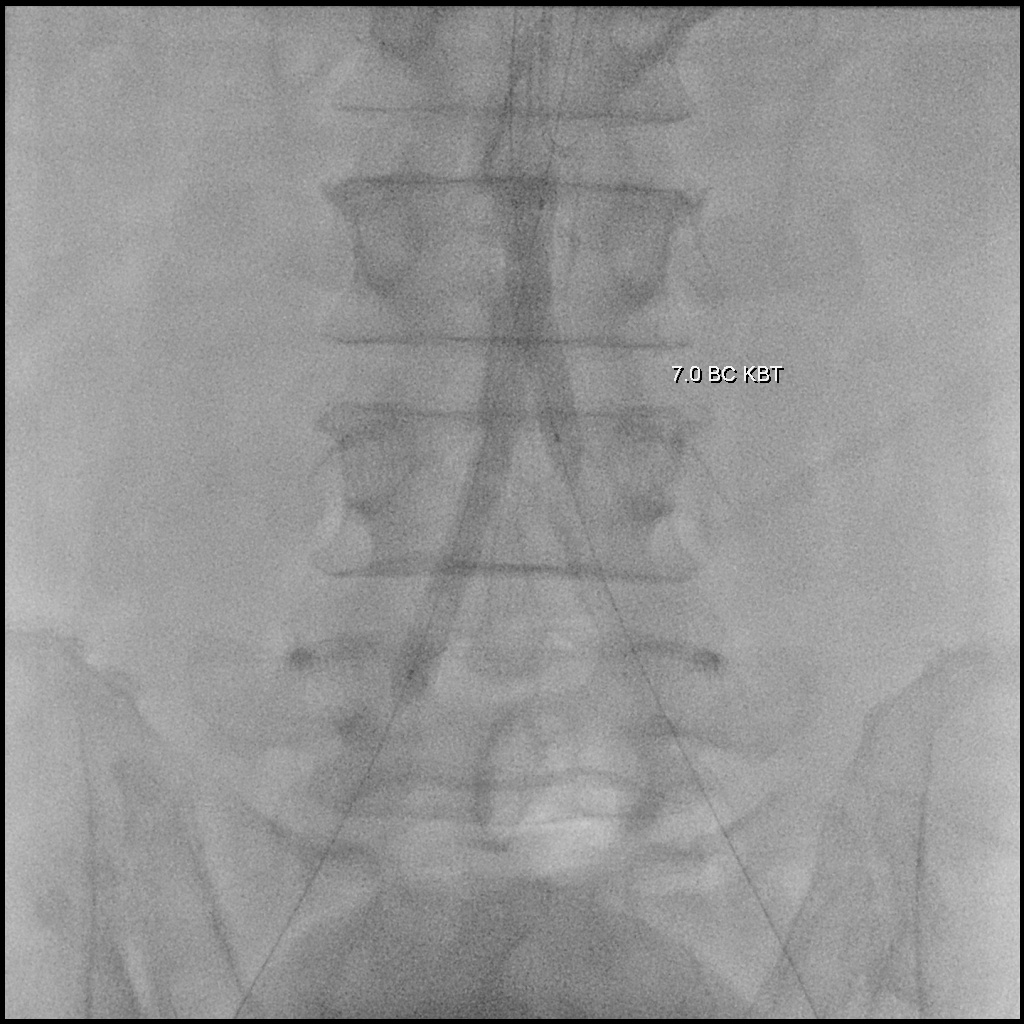
05683262_037..AVI
05683262_062..AVI
Case Summary
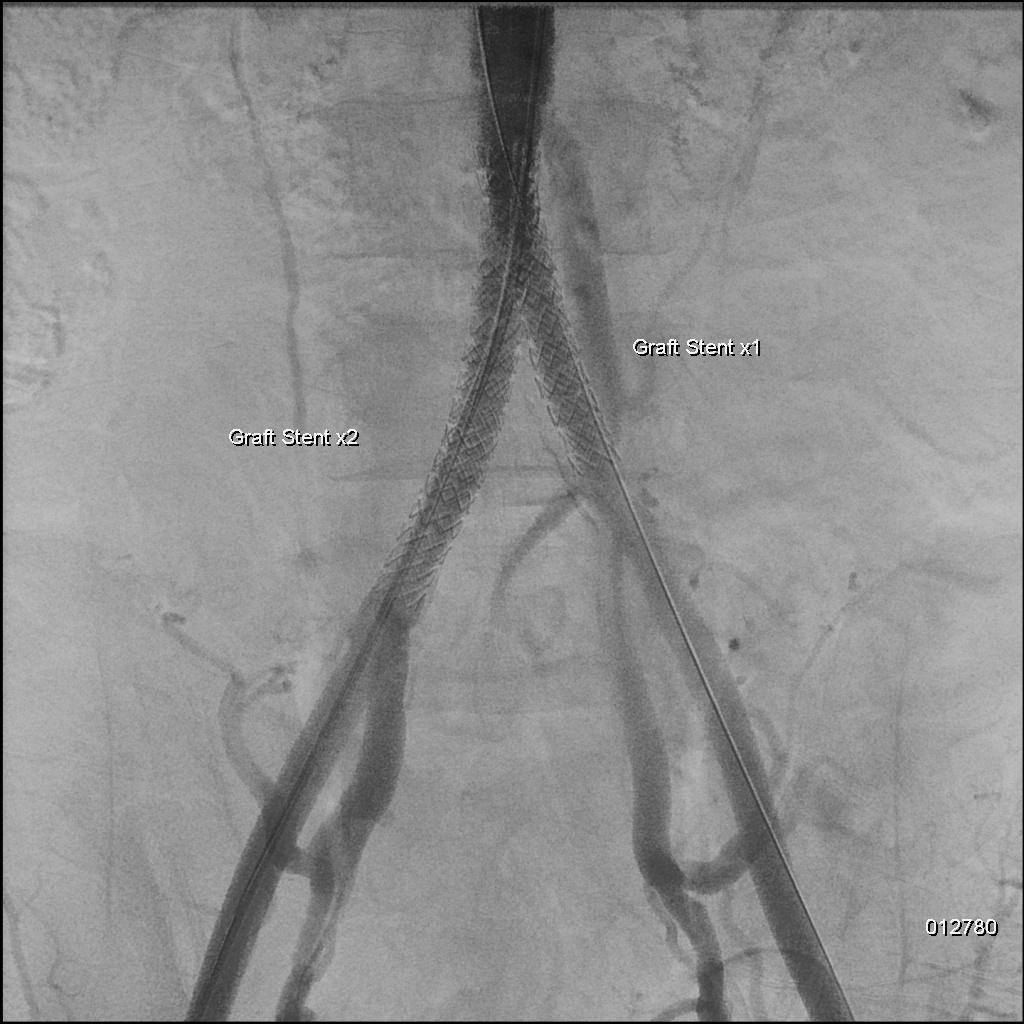
This case demonstrates successful IVUS-guided endovascular revascularization for aortoiliac occlusive disease . IVUS played a crucial role in confirming true lumen passage, identifying the lesion’s proximity to the inferior mesenteric artery, and providing accurate vessel sizing to guide optimal stent selection and landing zones while sparing the inferior mesenteric artery. Bilateral VBX stent graft implantation achieved excellent angiographic results with complete revascularization and restoration of distal flow. This case highlights the value of IVUS guidance in enhancing procedural precision and safety in complex aortoiliac interventions.