Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_012
Periprocedural PCI Paradoxical Effect Cases on Massive Ischemic and Hemorrhagic Stroke Post PCI
By Anggia Endah Satuti, Yoka Mahendra
Presenter
Anggia Endah Satuti
Authors
Anggia Endah Satuti1, Yoka Mahendra1
Affiliation
Yogyakarta Regional Hospital, Indonesia1
View Study Report
CASE20251107_012
Coronary - ACS/AMI
Periprocedural PCI Paradoxical Effect Cases on Massive Ischemic and Hemorrhagic Stroke Post PCI
Anggia Endah Satuti1, Yoka Mahendra1
Yogyakarta Regional Hospital, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
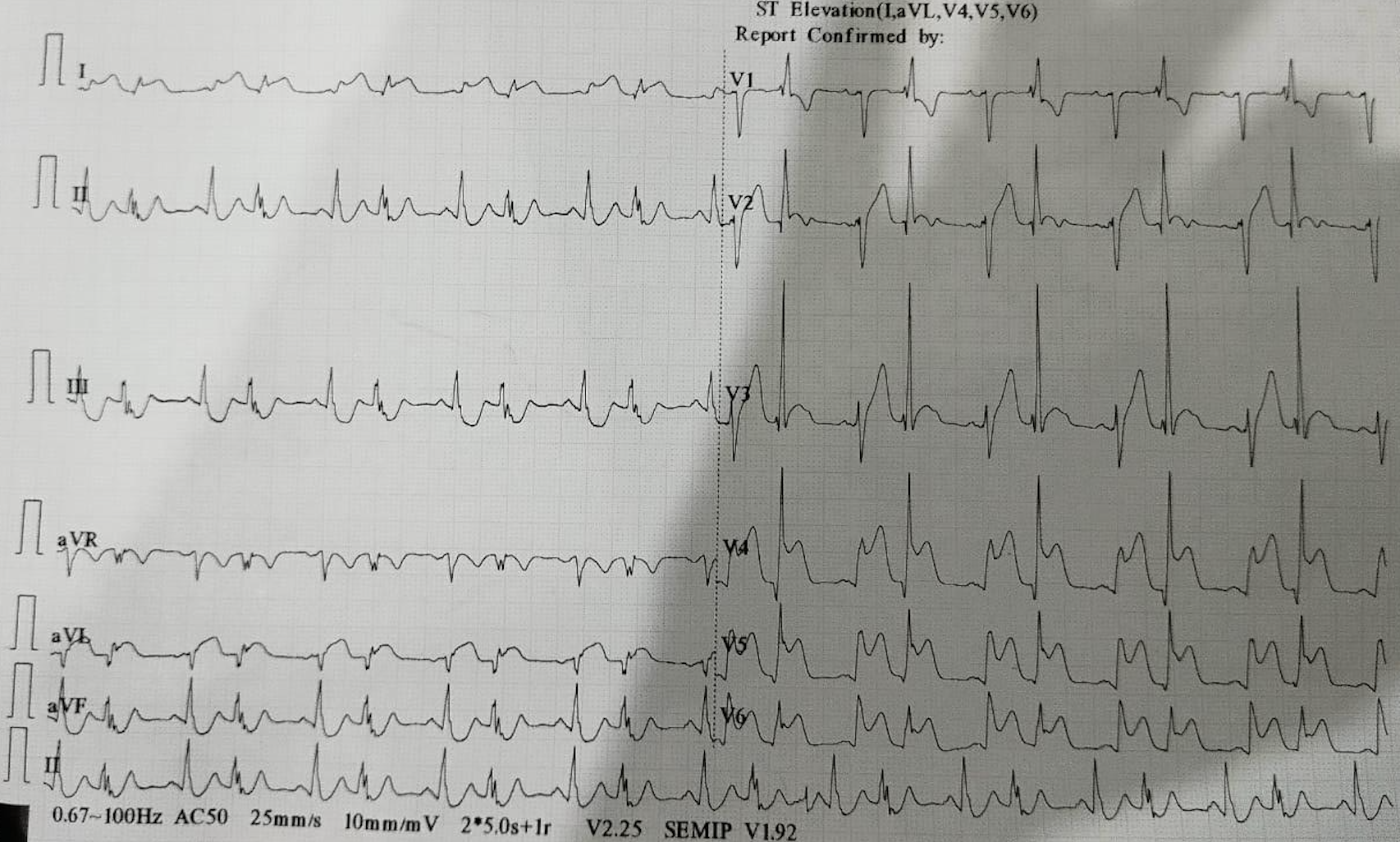
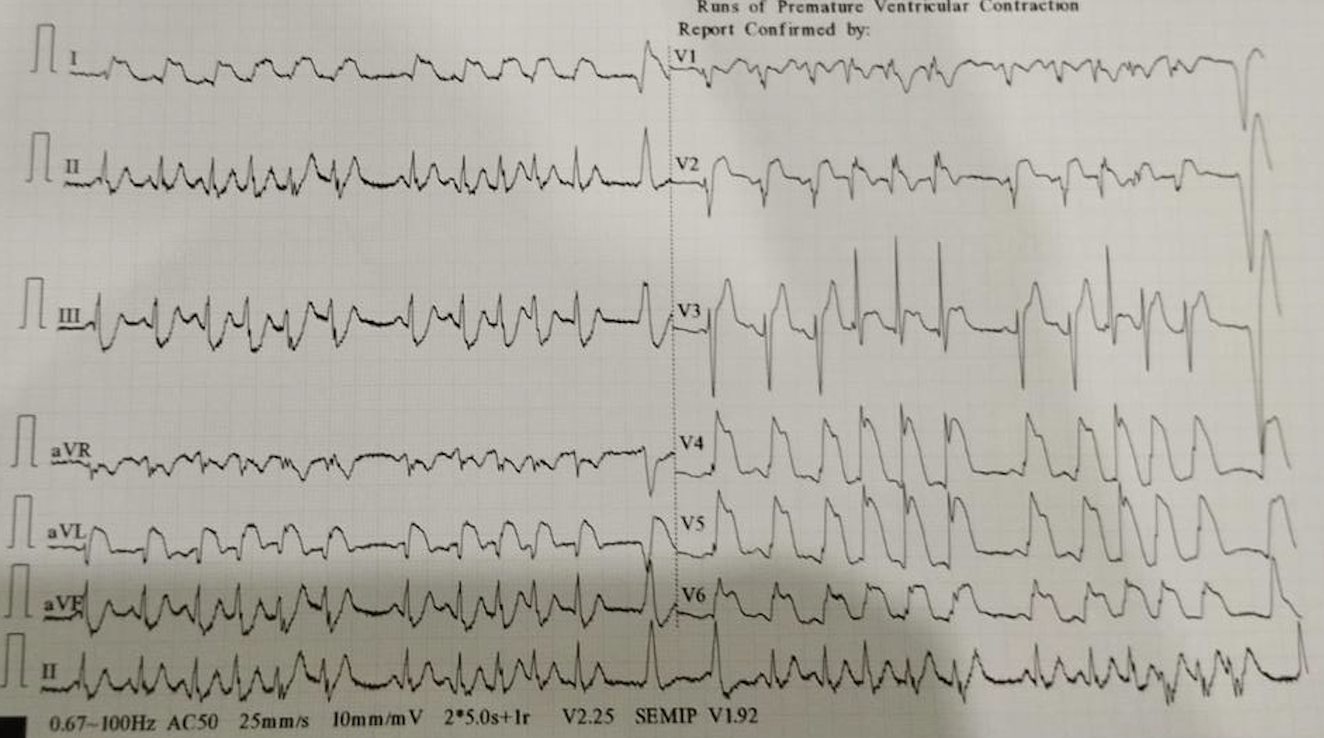
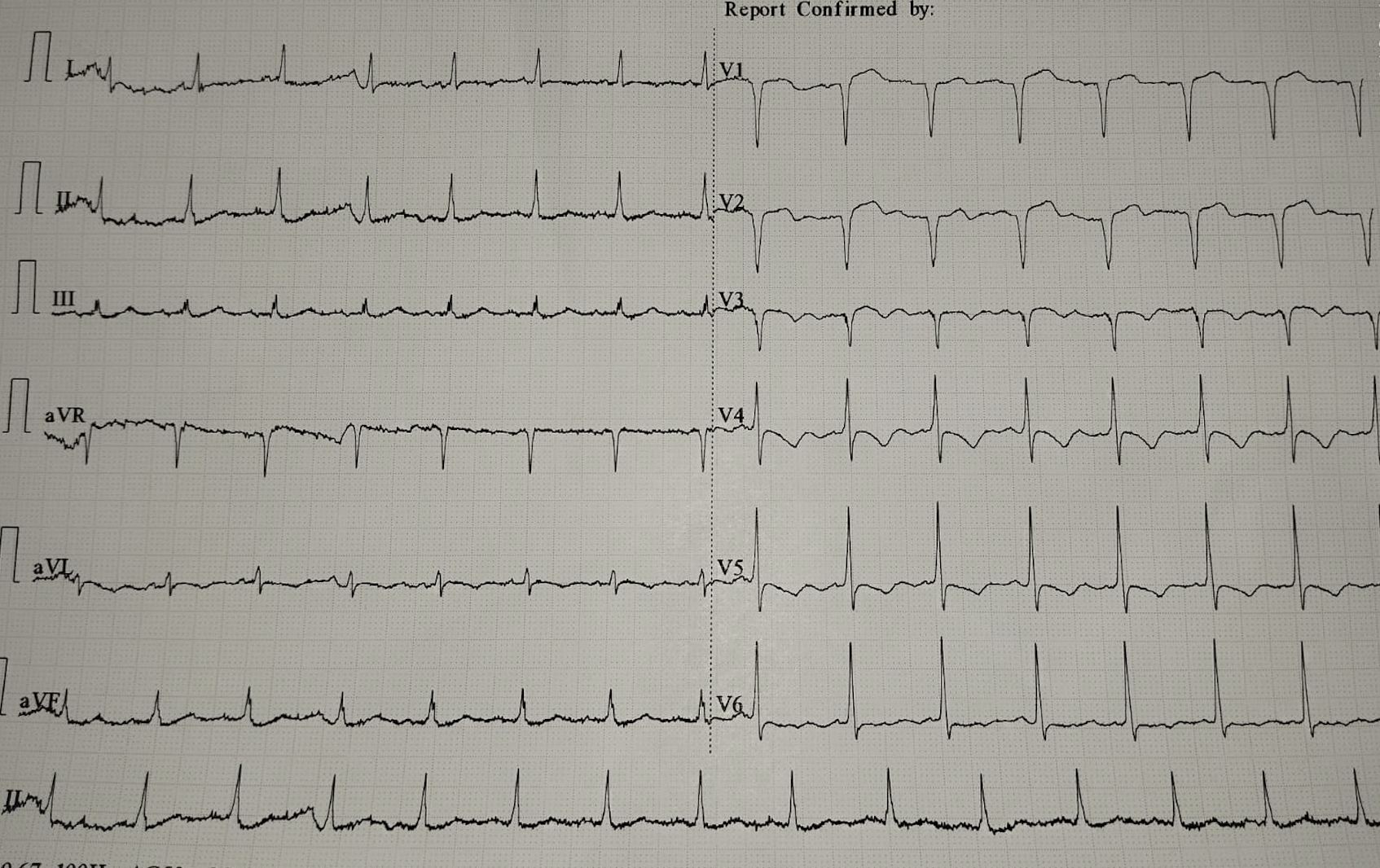
First patient 20 years male with STEMI Anterior Extensive. Risk factor : electronic cigarette smoking.The ECG was RBBB type ST elevation in V1-V6 and I, aVL.Hs troponin level 130.7 ng/L.Second Patient 44 years old male with Anteroseptal STEMI. Risk factor hypertension and a heavy smoker for 20 years. His ECG was Anteroseptal ST elevation with downslope ST depression on V4-V6. The Hs Troponin level 958 ng/L.
Relevant Test Results Prior to Catheterization
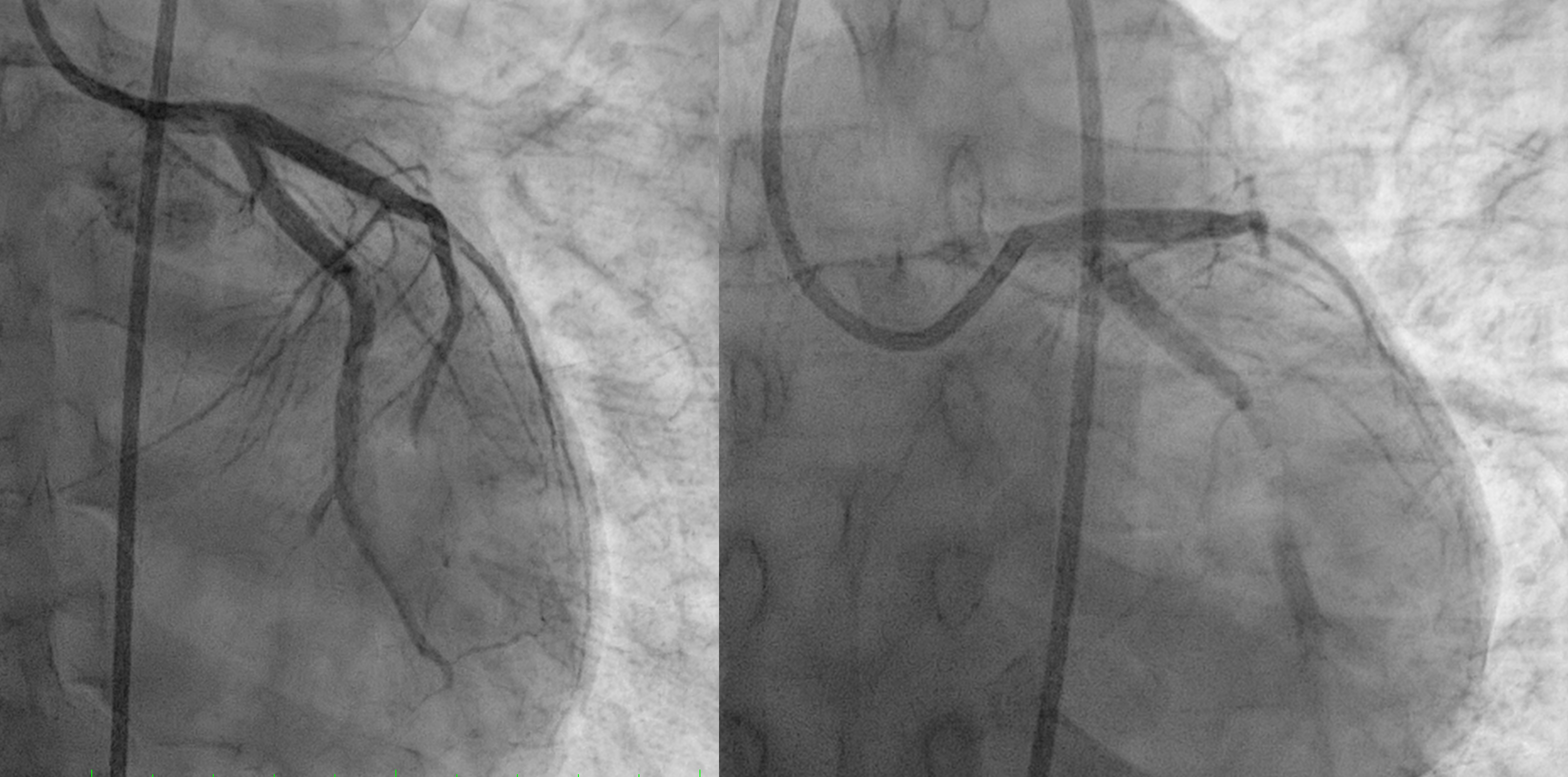
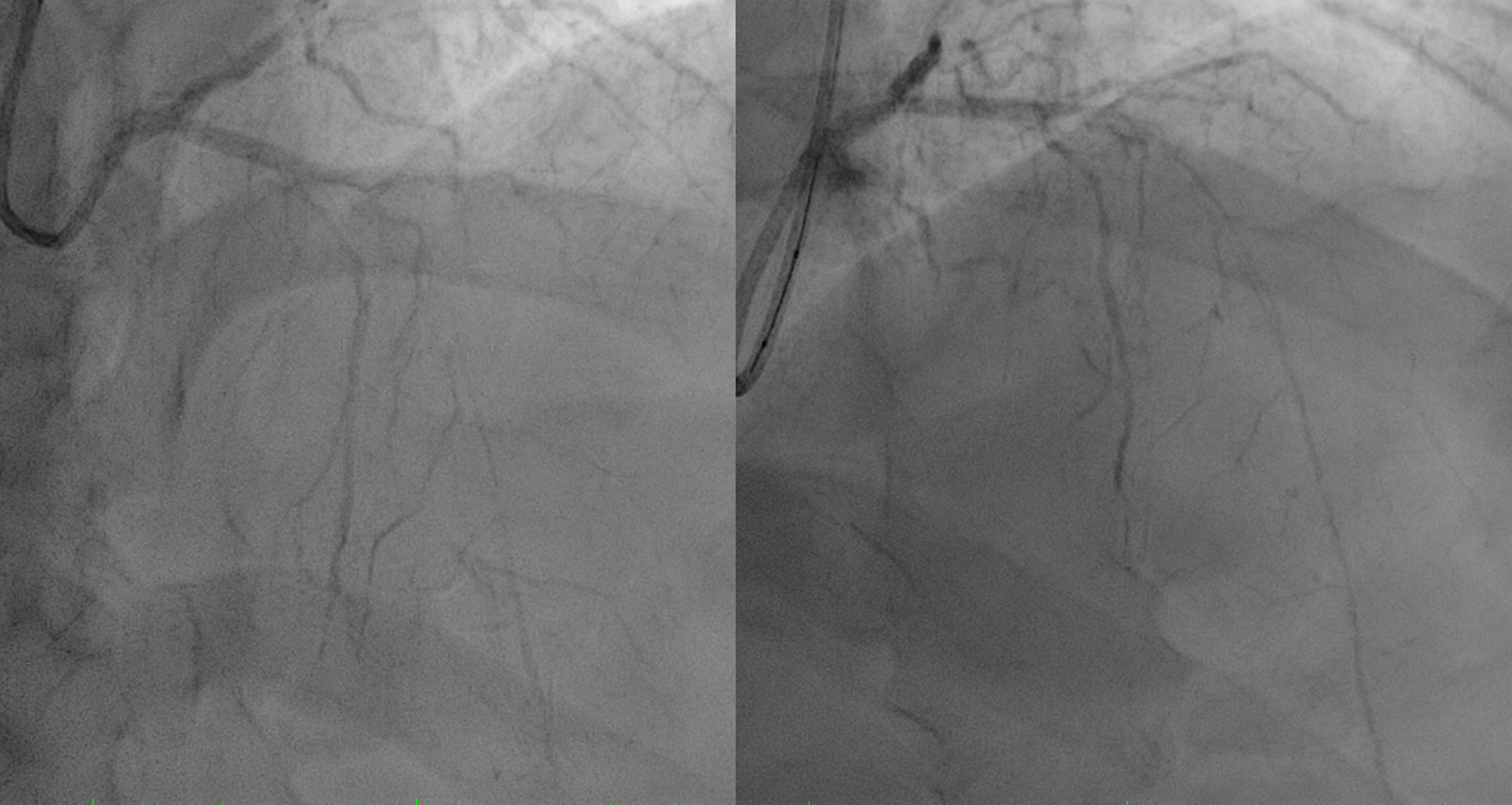
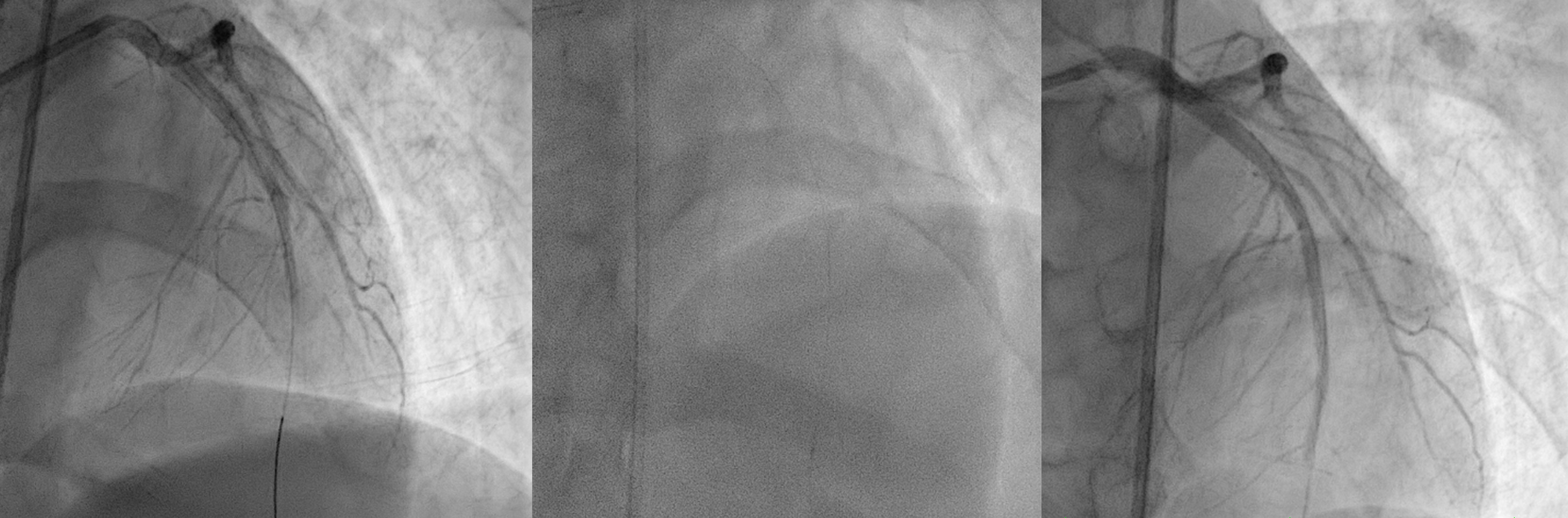
First patient was done thrombolytic therapy and failed, was done angiography with thrombus in LAD and LCx. We did thrombus aspiration and get TIMI 2 flow.Second patient was done primary PCI and having only POBA due to ambiguous distal LAD
Relevant Catheterization Findings
First patient develop massive ischemic stroke post PCI although patient got thrombolytic, PCI and anticoagulant and dual antiplatelet.
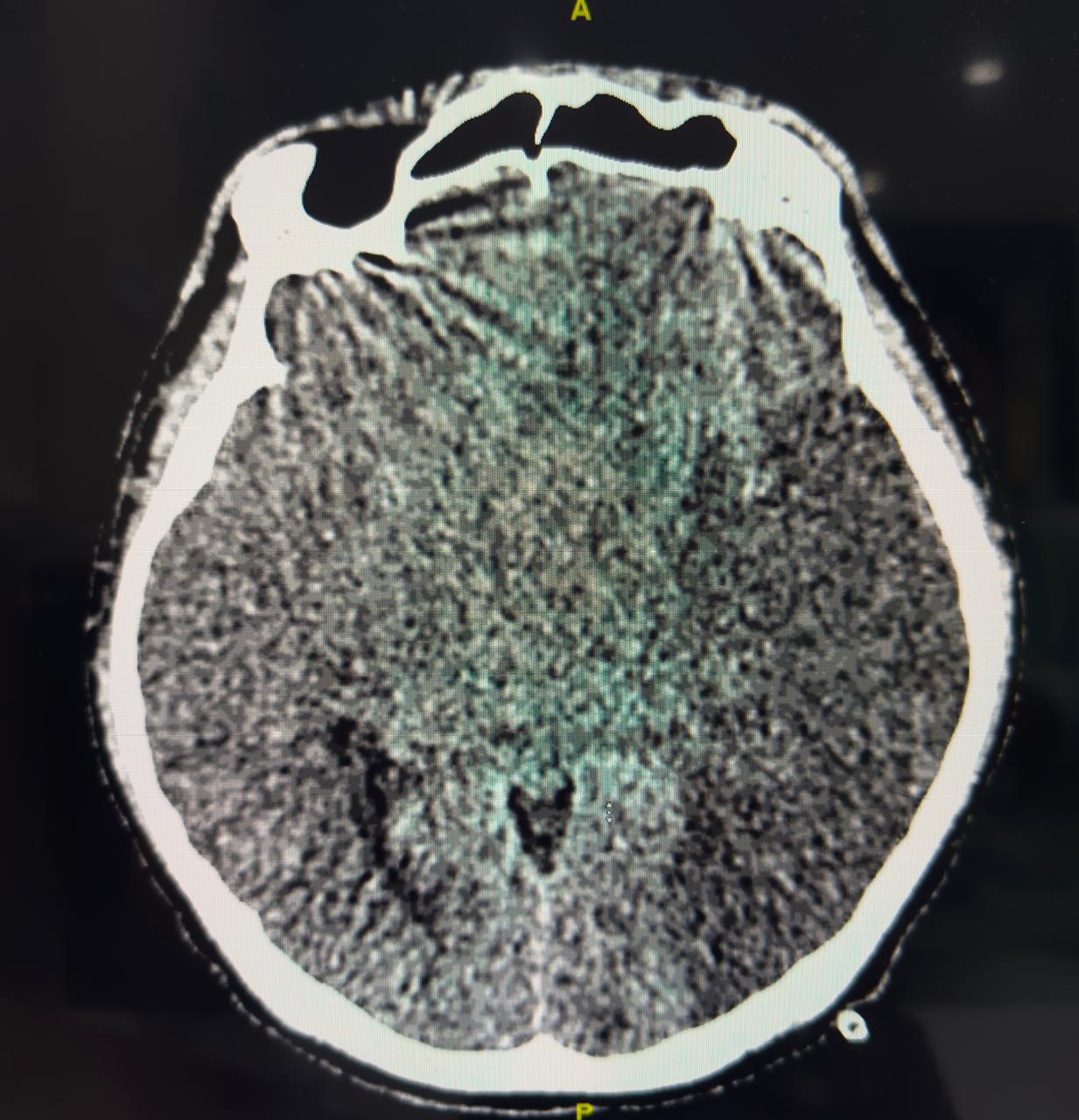
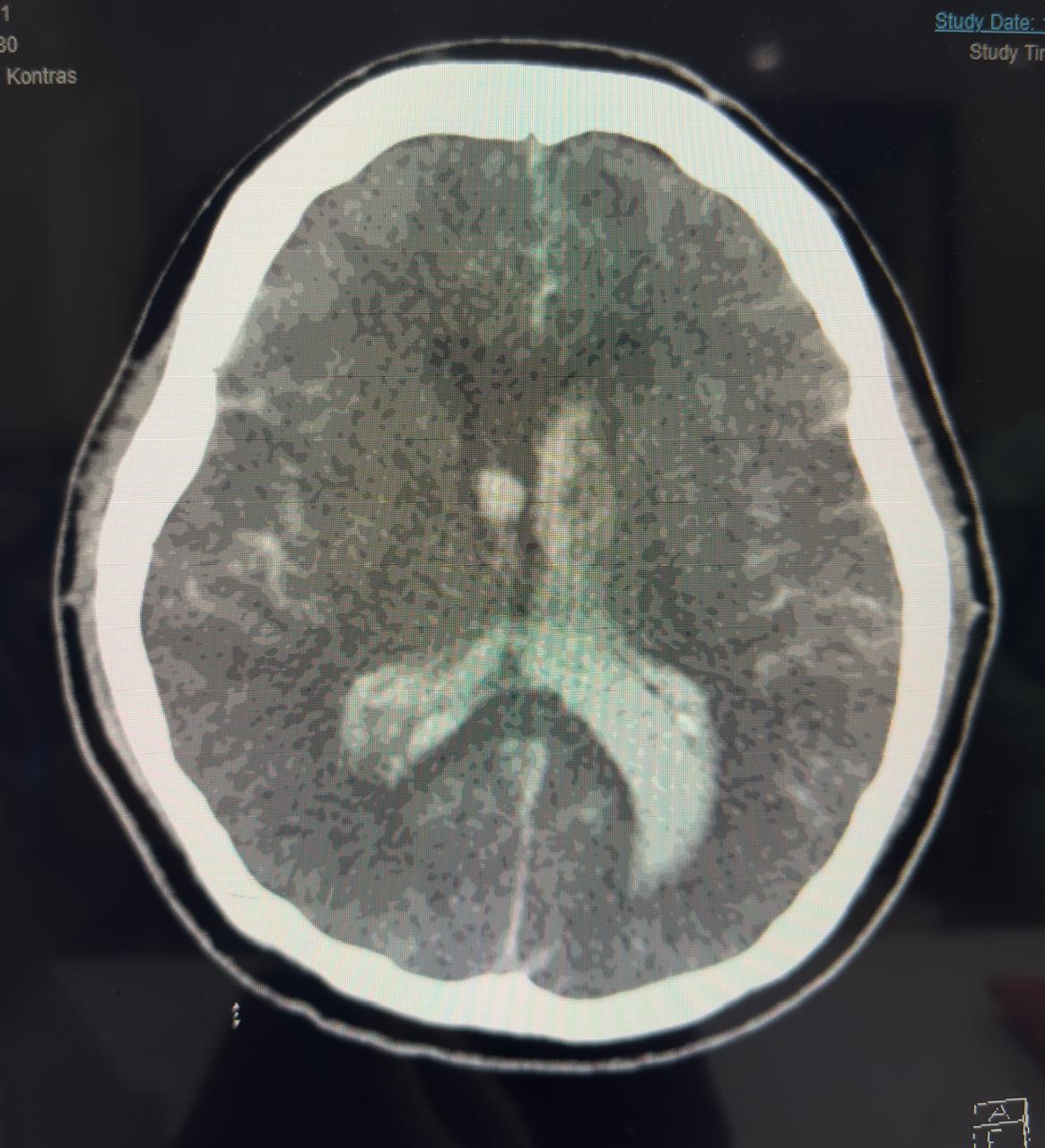
Second patient developed massive haemorrhagic stroke, despite normal APTT after PCI, anticoagulant use in normal dosage.
Interventional Management
Procedural Step
first patient using Guidewire Runthrough to LAD and done Thrombus Aspiration and move to LCx to do Thrombus Aspiration. Patient was given eptifibatide bolus. But thrombus still high burden but already have better flow so we stopped case and heparinized. Second patient was having CTO LAD, wire with Pilot 50 but then escalated to Pilot 150. We could puncture the proximal cap, done POBA proximal with small balloon 1.5x15 mm and then up to 2.5x15 mm but the distal wire we suspect not in true lumenso we stopped the case after having better view distal LAD.

Case Summary
Both patient developed stroke periprocedural but in a paradoxical way. One with heavy thrombus burden young patient with thrombolytic, GP2B3A infusion, anticoagulation and dual antiplatelet but developed acute massive ischemic stroke and did not survive. The second patient developed acute massive haemorrhagic stroke due to sudden increase of blood pressure, despite the use of normal dose of anticoagulation, low ARC HBR score, and normal pressure during procedure. So stroke both ischemic or haemorrhagic are devastating and have high mortality, but until now there is no actual scoring system to predict only on ARC HBR to prevent bleeding periprocedural.