Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_010
Artery Open, Flow Broken
By Chi Na Cheng, Chi Wing Wong, Shung Yee Wong
Presenter
Chi Na Cheng
Authors
Chi Na Cheng1, Chi Wing Wong1, Shung Yee Wong1
Affiliation
Pok Oi Hospital, Hong Kong, China1
View Study Report
CASE20251107_010
Coronary - Complex PCI - CTO
Artery Open, Flow Broken
Chi Na Cheng1, Chi Wing Wong1, Shung Yee Wong1
Pok Oi Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
Patient has history of DM, Hypertension, hyperlipidemia, infrarenal AAA. He also has know Ischemic cardiomyopathy. Coronary angiogram showed triple vessel disease with RCA CTO. He was referred CTS for CABG.
This time he was presenting with cardiogenic shock.
Noted progressive reduce in exercise tolerance with lower limb edema for 3 days
On examination, he was hypotensive with cold periphery
He was started on dopamine and adrenaline support.
This time he was presenting with cardiogenic shock.
Noted progressive reduce in exercise tolerance with lower limb edema for 3 days
On examination, he was hypotensive with cold periphery
He was started on dopamine and adrenaline support.
Relevant Test Results Prior to Catheterization
Lactate 4.2
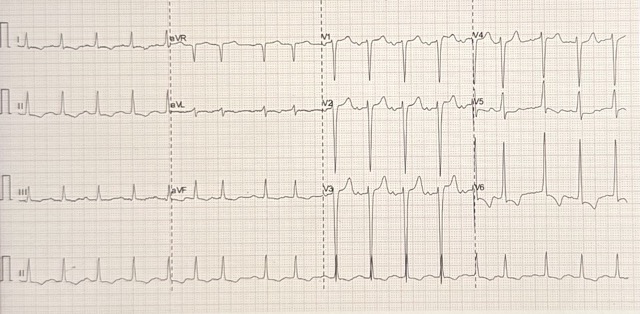
ECG SR, old TWI with no ST elevation
ECHO: LVEF 25%, global hypokinesia
ECG SR, old TWI with no ST elevation
ECHO: LVEF 25%, global hypokinesia
Relevant Catheterization Findings
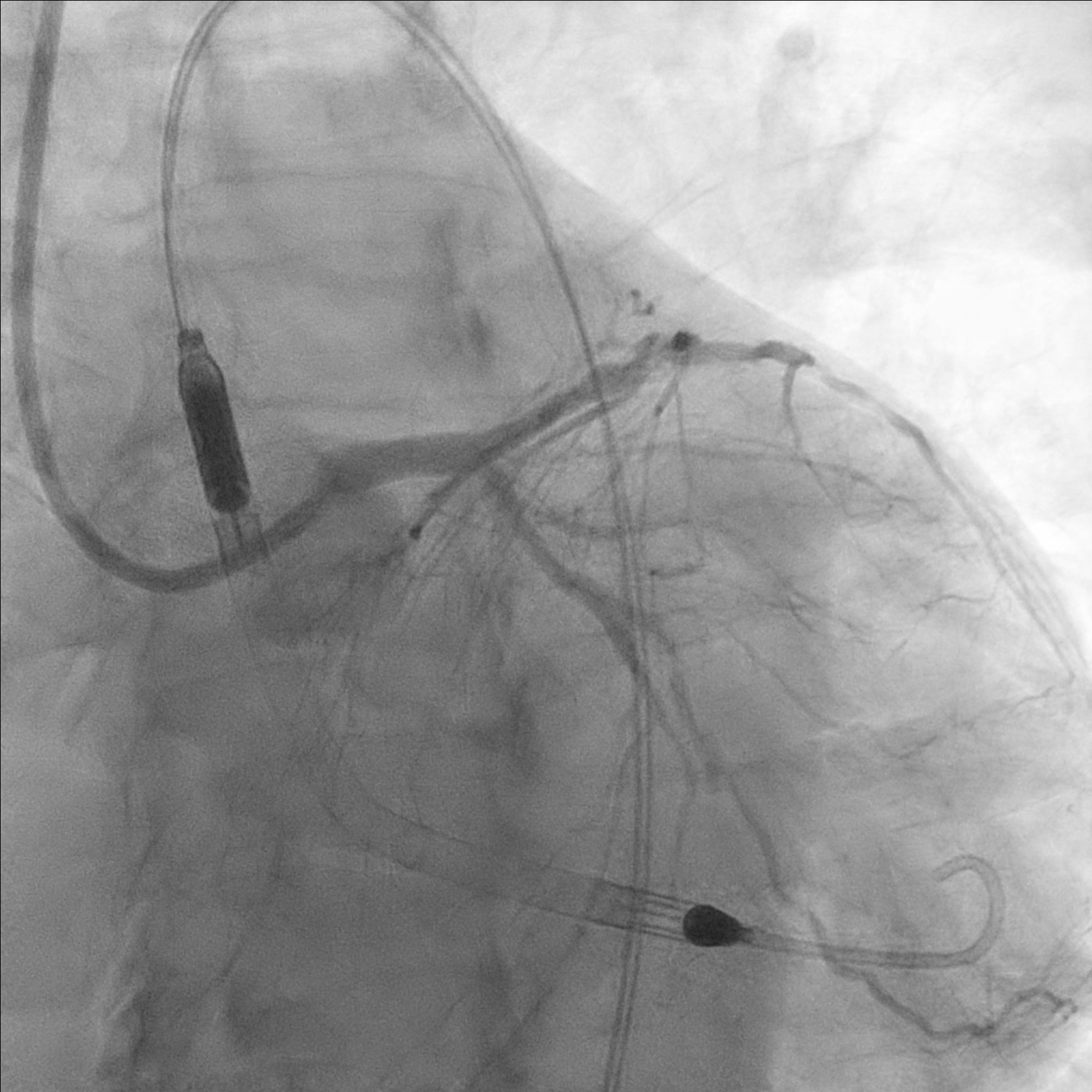
Coronary angiogram showed triple vessel disease and RCA CTO- Left main: normal- LAD: p-mLAD severe disease- LCx: m-dLCx severe disease- RCA: dominant, mRCA total occlusion with retrograde from left system
Interventional Management
Procedural Step
Impella inserted to left femoral artery due to known right femoral artery stenosis
7-in-6Fr slender sheath inserted to right radial artery. LM engaged with F7 EBU guiding catheter. p-mLAD was predilated with scoring balloon. 2.5/50 DES was deployed to p-mLAD.
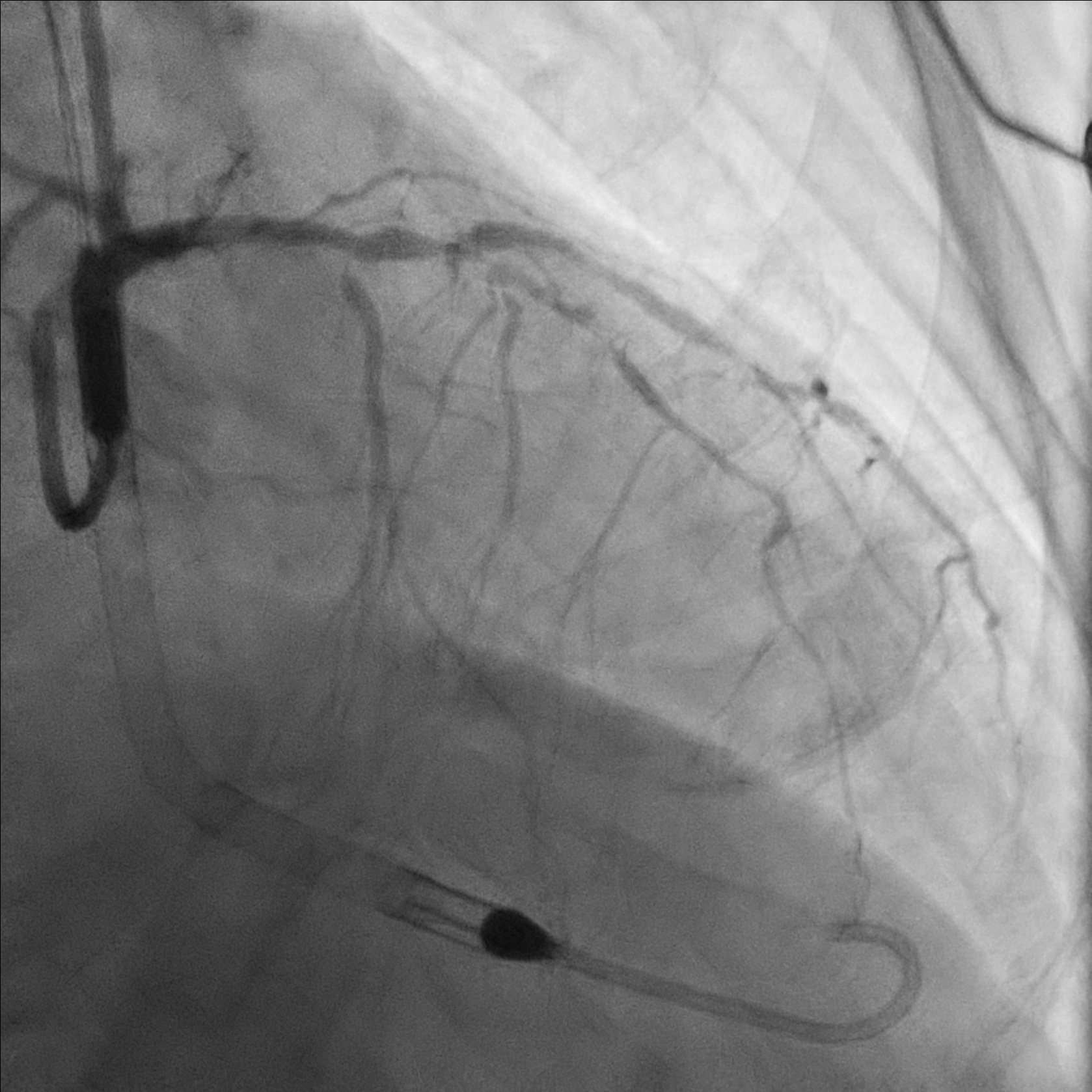
7Fr sheath inserted to right femoral artery. RCA engaged with F7 AL1. Attempted wiring with UB3, Fielder XT-A, Gaia Next 2 and Gaia Next 3. Finally successful RCA wiring with Gaia Next 2 by parallel wire technique. Predilation with Scoring balloon. IVUS showed true lumen wiring. A 3.5/50 DES was deployed over m-dRCA, another 4.0/38 DES was deployed over p-mRCA.
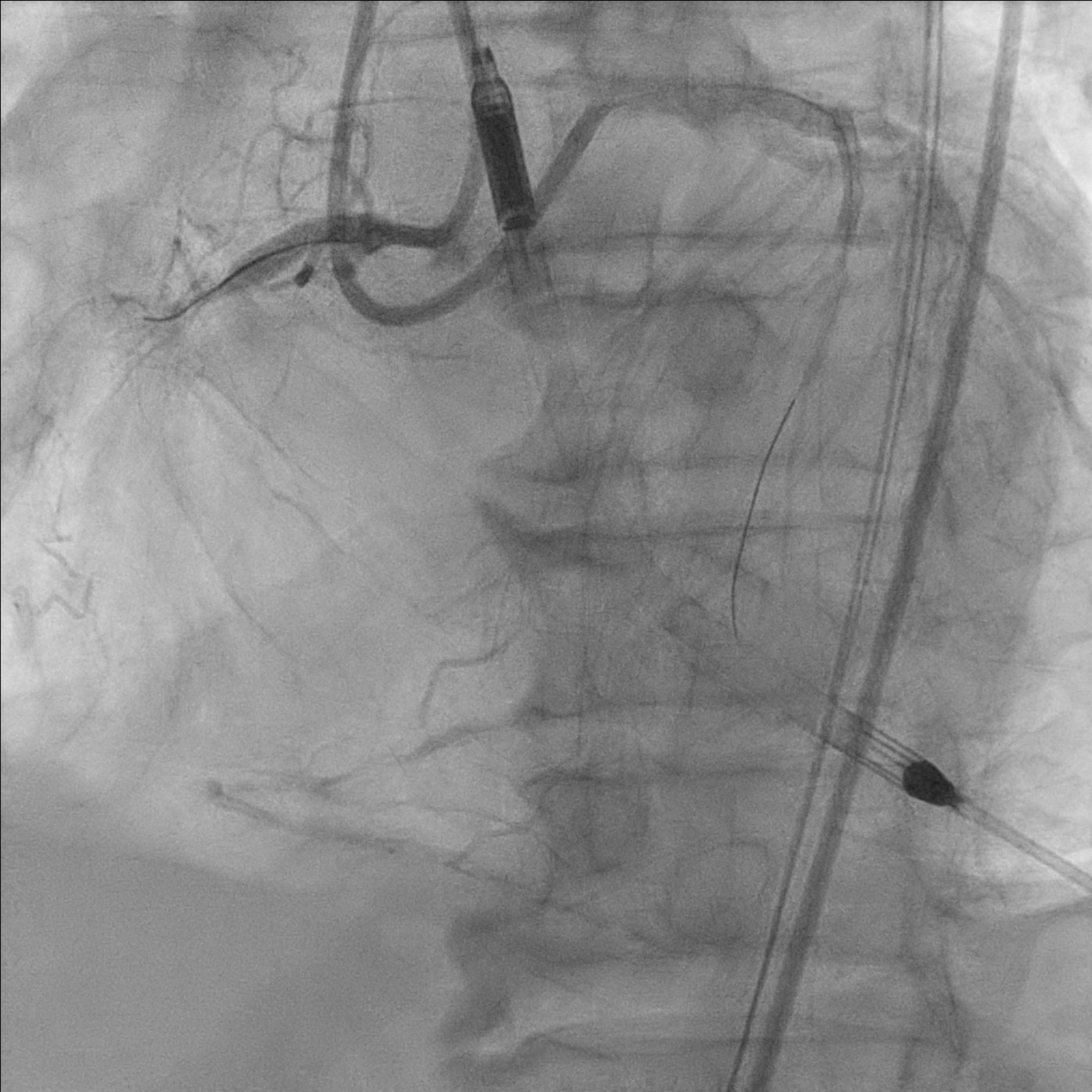
Developed diminishing arterial waveform. Angiogram showed TIMI 1-2 flow, retrograde injection showed no retrograde filling. IVUS showed subintimal hematoma, suspected distal dissection. Hematoma covered with a 4.0/14 DES. IVUS showed good stent apposition and no edge dissection. Flow improved to TIMI2-3 flow after intracoronary adenoscan and adrenaline. Noted filling defect over mRCA stent. Intracoronary integrillin was given and stent thrombosis resolved angiographically.

 PCI 3.mp4
PCI 3.mp4
PCI 4.mp4
7-in-6Fr slender sheath inserted to right radial artery. LM engaged with F7 EBU guiding catheter. p-mLAD was predilated with scoring balloon. 2.5/50 DES was deployed to p-mLAD.
7Fr sheath inserted to right femoral artery. RCA engaged with F7 AL1. Attempted wiring with UB3, Fielder XT-A, Gaia Next 2 and Gaia Next 3. Finally successful RCA wiring with Gaia Next 2 by parallel wire technique. Predilation with Scoring balloon. IVUS showed true lumen wiring. A 3.5/50 DES was deployed over m-dRCA, another 4.0/38 DES was deployed over p-mRCA.
Developed diminishing arterial waveform. Angiogram showed TIMI 1-2 flow, retrograde injection showed no retrograde filling. IVUS showed subintimal hematoma, suspected distal dissection. Hematoma covered with a 4.0/14 DES. IVUS showed good stent apposition and no edge dissection. Flow improved to TIMI2-3 flow after intracoronary adenoscan and adrenaline. Noted filling defect over mRCA stent. Intracoronary integrillin was given and stent thrombosis resolved angiographically.
Case Summary
Impella assisted PCI showed be considered in patient with high risk anatomy and poor LVEF.
Differential diagnoses of no reflow including microvascular dysfunction, intravascular obstruction and flow competition.
Rapid identification of complication is important for prompt management.
Differential diagnoses of no reflow including microvascular dysfunction, intravascular obstruction and flow competition.
Rapid identification of complication is important for prompt management.