Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_009
Transcatheter Closure of Paravalvular Leak Following Multiple Bioprosthetic Valve Replacements in a Rheumatic Heart Disease Patient
By MinJhih Chen
Presenter
MinJhih Chen
Authors
MinJhih Chen1
Affiliation
National Taiwan University Hospital, Taiwan1
View Study Report
CASE20251107_009
Structural - Aortic Valve Intervention - Valve in Valve TAVR
Transcatheter Closure of Paravalvular Leak Following Multiple Bioprosthetic Valve Replacements in a Rheumatic Heart Disease Patient
MinJhih Chen1
National Taiwan University Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 78-year-old woman with a long-standing history of rheumatic heart disease presented with complex multivalvular involvement, including MR, MS, AR and AS. She underwent two mitral valvuloplasties in her third and fourth decades of life and subsequently received combined surgical aortic valve replacement (AVR) and mitral valve replacement (MVR) in 2015, TAVR-in SAVR procedure in 2022 due to recurrent heart failure. However, in 2025, physical examination showed pitting edema and lung edema again.

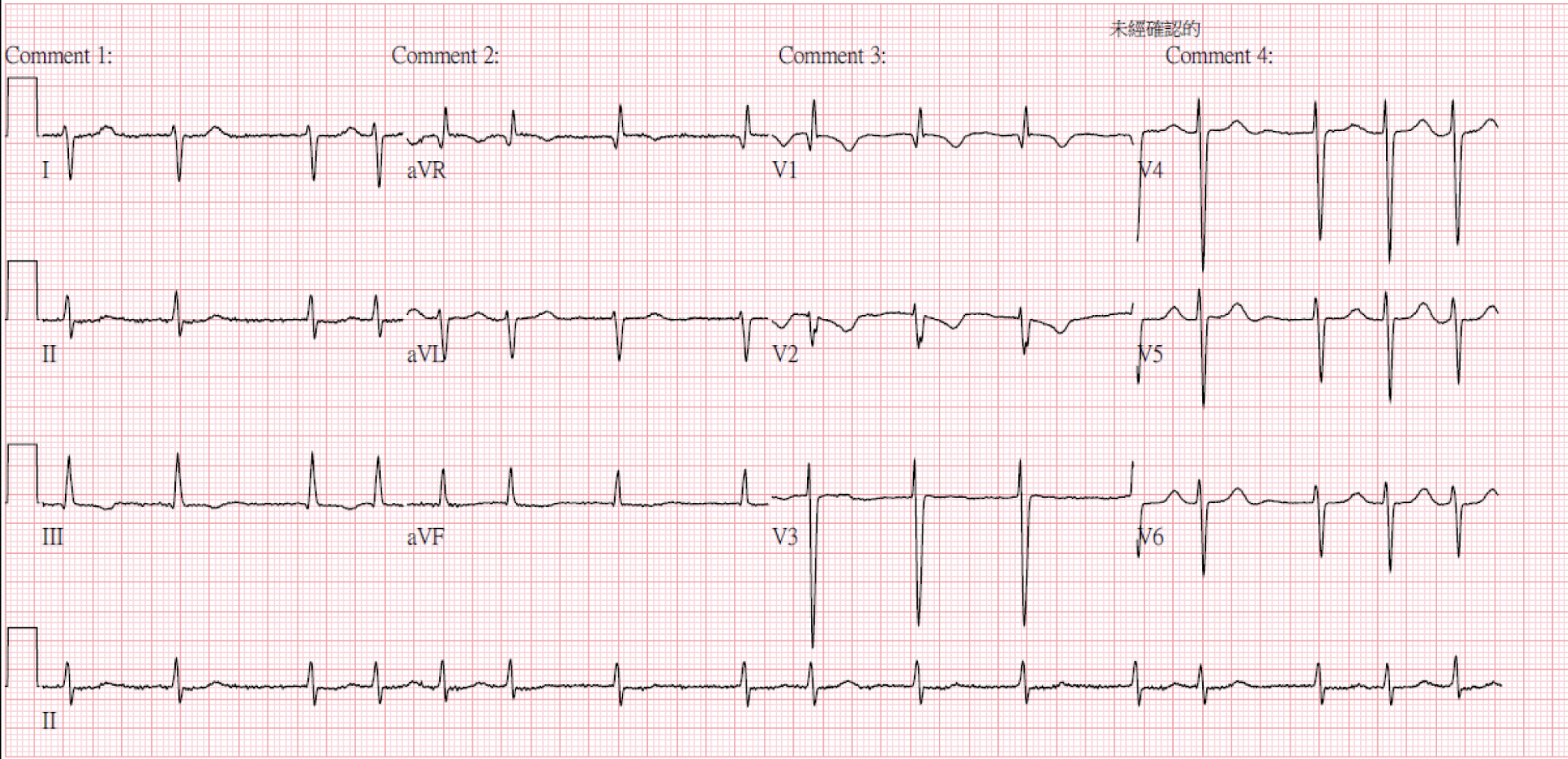
Relevant Test Results Prior to Catheterization
Laboratory examination: Hb: 6.3 g/dL, MCV 111.7 fL, Plt 246 k/uL, Reticulocyte 6.8 %, Iron 90 ug/dL, TIBC 326 ug/dL, ferritin 375 mg/mL, LDH 1025 U/L, Haptoglobin < 27.20 mg/dL, Creatinine 1.61 mg/dL, BUN 66.6 mg/dL, Total billirubin 1.44 mg/dL, ALT 14 U/L, NT-proBNP 9340 pg/mL
Echocardiogram: TTE and TEE
- LVIDd 40 mm, LA 68 mm, LVEF 70.9%, Ao mean PG 16.1 mmHg
- Increasing trans-aortic valve mean pressure gradient
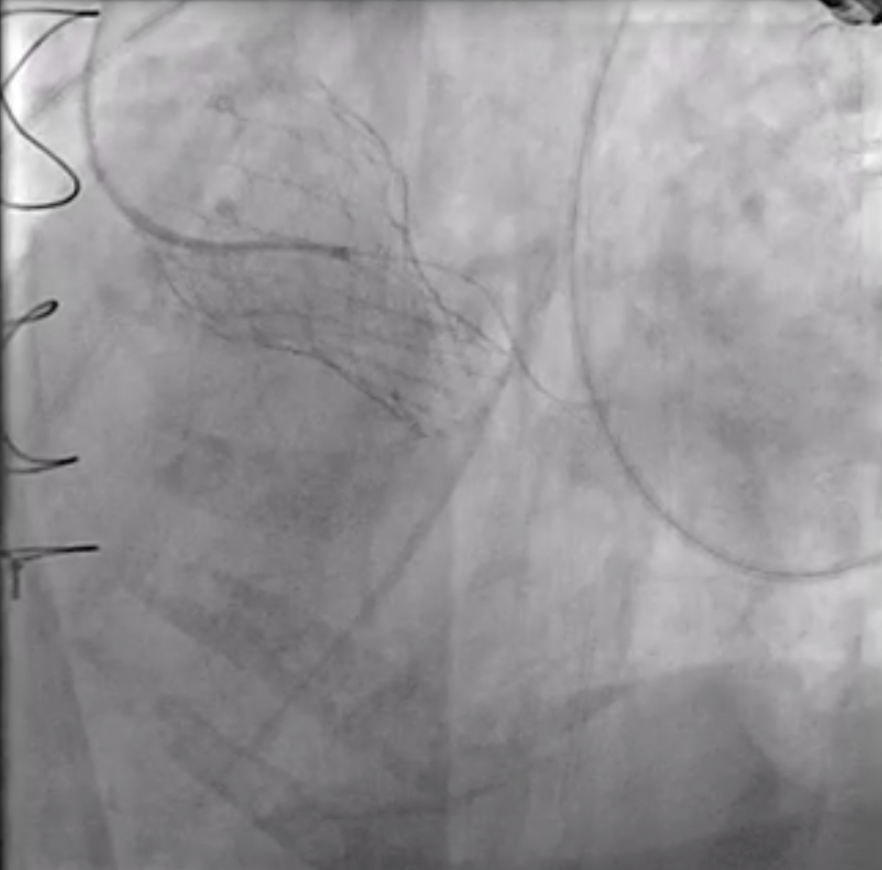
Relevant Catheterization Findings
Aortogram: a paravalvular leakage noted between SAVR and TAVR valveHemodynamic study:- Pulmonary wedge pressure = 18 mmHg- Pulmonary artery pressure = 58/19 mmHg (mean 37 mmHg)- RV pressure = 71/5 mmHg- RA mean pressure = 9 mmHg- IVC pressure = 9 mmHg- Cardiac output (thermodilution): 3.73 L/min- PVR = 5 woods (408 Dynes.sec.cm-5)
 Aortogram (5_17 angio).mp4
Aortogram (5_17 angio).mp4
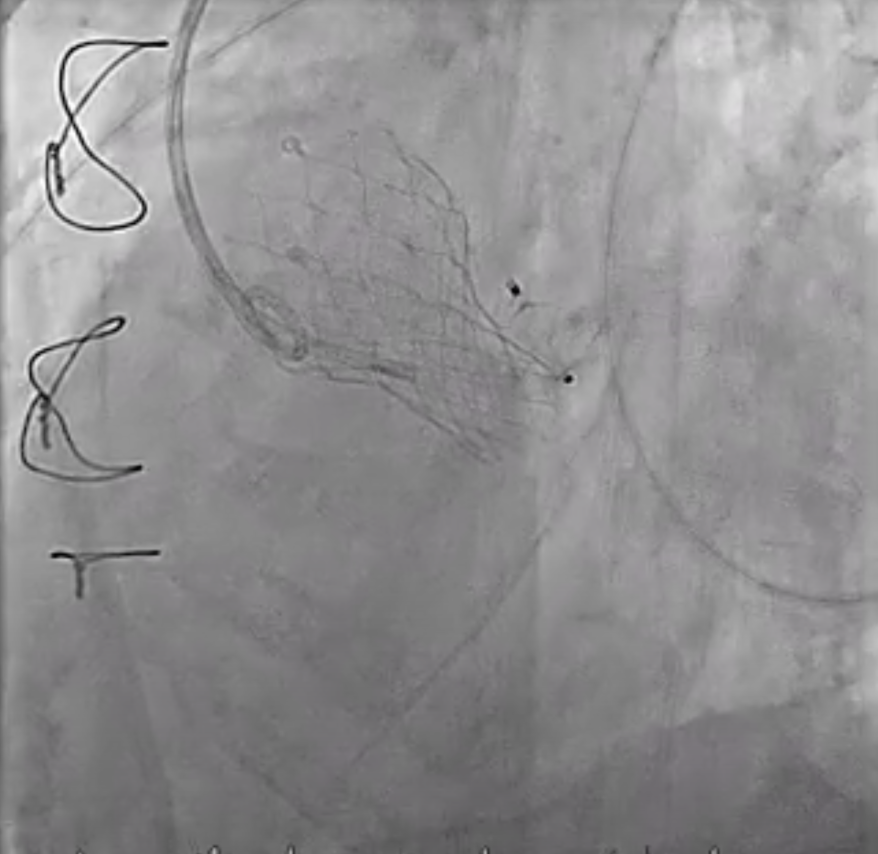
Interventional Management
Procedural Step
Under local anesthesia, the RFA was punctured, and a 6-Fr sheath was introduced. A 6-Fr pigtail catheter over a 0.035-inch J-tip wire was advanced into the ascending aorta, and an aortogram demonstrated a moderate PVL originating from the surgical valve ring and the aortomitral curtain.The pigtail catheter was replaced with a 6-Fr MPA2 catheter to delineate the anatomy of the transcatheter heart valves and PVL. A 6-Fr JL 3.5 catheter was then used for a nonselective left coronary angiogram, confirming the PVL adjacent to the aortic annulus. A Terumo guidewire was advanced through an Amplatz Left (AL1) catheter and successfully crossed the PVL into the left ventricle (LV).For device delivery, the LFA was also punctured, and a 6-Fr sheath was inserted. A pigtail catheter was placed in the ascending aorta to identify the left main ostium. Attempts to advance an AGA Amplatzer Vascular Plug (AVP) 10/7 mm through the PVL were made using multiple guiding systems, including AL and JR4 catheters, a 6-Fr Shuttle sheath, and a Superstiff 0.035-inch wire, but initial passage into the LV was unsuccessful.Balloon sizing was performed using a Boston Scientific Mustang balloon (4.0 mm × 20 mm × 75 cm) inflated to 4 atm. The 6-Fr sheath was exchanged for a 7-Fr sheath, and a 7-Fr Boston MP 90-cm guiding catheter was advanced into the LV. An AGA Amplatzer Vascular Plug 10/7 mm was successfully deployed across the PVL. Final aortography confirmed successful occlusion of the PVL.
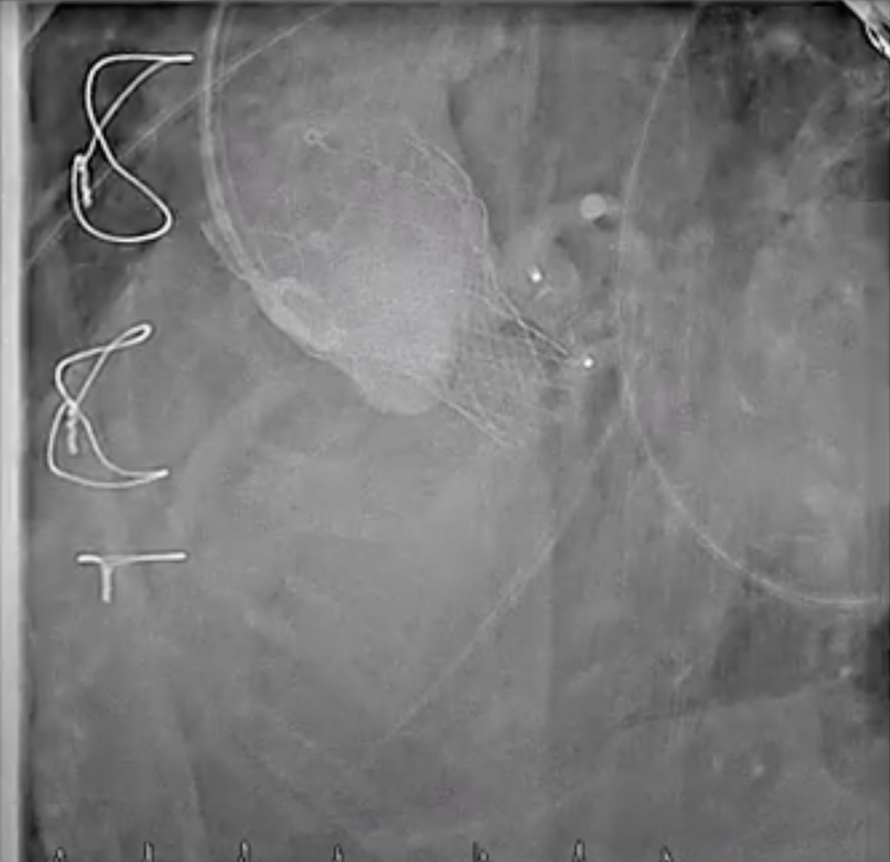
Final (5_17 angio).mp4
Case Summary
Traditionally, surgical repair has been the treatment of choice for clinically significant PVL. However, repeat surgery in elderly patients with multiple prior valve interventions carries substantial morbidity and mortality risks. In recent years, transcatheter PVL closure has emerged as a less invasive and effective alternative. The Amplatzer Vascular Plug is among the most commonly used devices for this purpose due to its flexibility, controlled deployment, and ability to conform to irregular defects.In this case, the patient’s PVL was successfully closed using an AVP 10/7 mm after multiple catheter exchanges and balloon sizing. Post-procedural imaging confirmed trivial residual PVL.