Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_007
The Road Not Taken-RCA CTO Coronary Perforation and Retrograde Salvage via LAD Epicardial Collateral
By Boon Cong Beh, Kazi Majidur Rahaman, Mohd Asyio Al Fard Bin Mohd Raffali, Noor Diyana Binti Mohamad Farouk, Mohd Haidir Bin Roslan, Hamat Hamdi Bin Che Hassan, Mohd Shawal Faizal Bin Mohamad
Presenter
Boon Cong Beh
Authors
Boon Cong Beh1, Kazi Majidur Rahaman1, Mohd Asyio Al Fard Bin Mohd Raffali1, Noor Diyana Binti Mohamad Farouk1, Mohd Haidir Bin Roslan1, Hamat Hamdi Bin Che Hassan1, Mohd Shawal Faizal Bin Mohamad1
Affiliation
Hospital Canselor Tuanku Muhriz UKM (HCTM), Malaysia1
View Study Report
CASE20251107_007
Coronary - Complex PCI - CTO
The Road Not Taken-RCA CTO Coronary Perforation and Retrograde Salvage via LAD Epicardial Collateral
Boon Cong Beh1, Kazi Majidur Rahaman1, Mohd Asyio Al Fard Bin Mohd Raffali1, Noor Diyana Binti Mohamad Farouk1, Mohd Haidir Bin Roslan1, Hamat Hamdi Bin Che Hassan1, Mohd Shawal Faizal Bin Mohamad1
Hospital Canselor Tuanku Muhriz UKM (HCTM), Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
63 years old gentleman, active smoker, with co-morbid of hypertension and ischemic heart disease (had previous LAD stenting 7 years ago), who was medically managed for NSTEMI recently at district hospital.
Relevant Test Results Prior to Catheterization
His serum Troponin level was raised. He was referred to our center for coronary angiogram.
Relevant Catheterization Findings
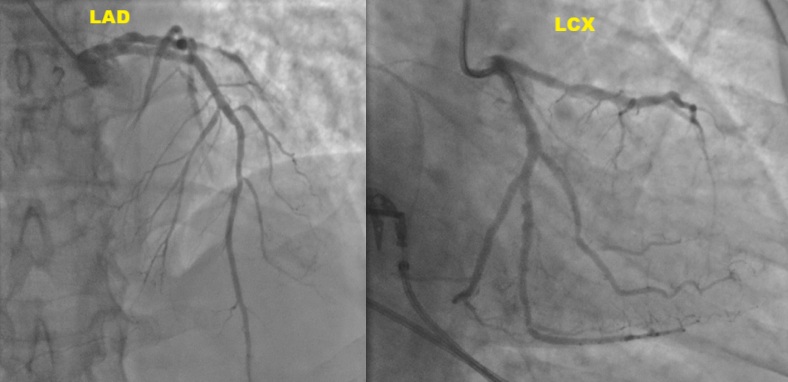
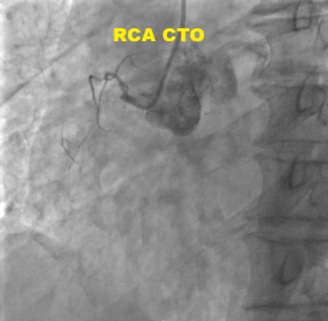
Coronary angiogram revealed mild LAD stent ISR, RCA CTO and severe obtuse marginal (OM) branches disease. PCI of the OM branches with drug-coated balloons was performed. Subsequently electively admitted for stage PCI to RCA CTO.
Interventional Management
Procedural Step
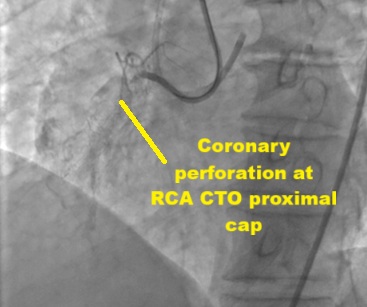
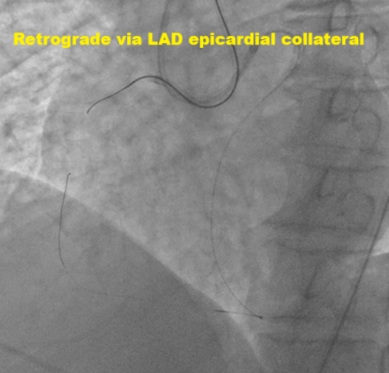
Dual access via right radial and femoral arteries. Failed to cross antegradely the proximal cap CTO using UltimateBros3 and Fielder XT-R guidewires / Corsair Pro, and retrogradely via septals collateral. Initially decided to abandon the procedure as deem small RCA vessel size. Unfortunately noted coronary perforation at proximal RCA CTO site, temporary tamponade with microcatheter. Retrograde Suoh3 wire via LAD epicardial collateral successfully crossed the distal cap of proximal RCA CTO, however, Caravel microcatheter unable to pass through the distal RCA branch for better support. Gladius EX14 guidewire supported with Corsair Pro microcatheter swiftly crossed the proximal cap antegradely (using the Suoh3 as the guide from retrograde) successfully till distal RCA branch. Caravel and Suoh3 removed retrogradely without complication. Predilate the RCA (prolonged balloon inflation) using SC 2.0x15mm (6-8atm, 3mins each) - to facilitate the plaque sealing of the perforation site. IVUS performed confirmed the wire in the true lumen. Stented with 2 overlapping DES 2.25x33mm (nominal) and 3.0x33mm (nominal). Noted the stent was from RCA-acute marginal branch, distal RCA was smaller vessel. Post-dilated distal stent with NC 2.5x15mm (nominal) while proximal stent with NC 3.0mm and NC 4.0mm. IVUS performed good stent apposition/expansion, with satisfactory MSA. Good angiographic result, TIMI 3 flow, no dissection/perforation noted. No pericardial effusion from echocardiography.
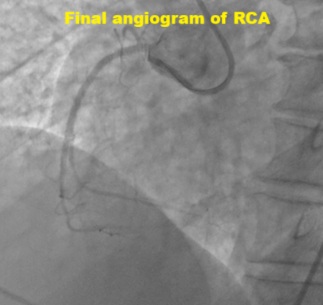
Case Summary
His hemodynamic was stable throughout the procedure. He was discharged from ward the next day. Clinical follow in clinic, he remained asymptomatic. Retrograde approach via the epicardial collateral remained a high risk route for PCI. Precaution to prevent untoward complication. This case demonstrated the salvage of the coronary perforation at RCA CTO via the LAD epicardial collateral.