Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_006
A Case of Revascularization Using a Retrograde Approach in the Subacute Phase of an Acute Inferior Myocardial Infarction
By Yoshitomo Tsutsui, Yuta Nishimura, Kiwamu Sudo, Kota Tanaka, Masakazu Yasuda, Tomohiro Yamasaki, Satoshi Watanabe, Mutsumi Iwamoto, Atsunori Okamura, Heitaro Watanabe
Presenter
Yoshitomo Tsutsui
Authors
Yoshitomo Tsutsui1, Yuta Nishimura2, Kiwamu Sudo2, Kota Tanaka2, Masakazu Yasuda2, Tomohiro Yamasaki2, Satoshi Watanabe2, Mutsumi Iwamoto2, Atsunori Okamura2, Heitaro Watanabe2
Affiliation
Sakurabashi Watanabe Hospital, Japan1, Sakurabashi Watanabe Advanced Healthcare Hospital, Japan2
View Study Report
CASE20251107_006
Coronary - Complex PCI - CTO
A Case of Revascularization Using a Retrograde Approach in the Subacute Phase of an Acute Inferior Myocardial Infarction
Yoshitomo Tsutsui1, Yuta Nishimura2, Kiwamu Sudo2, Kota Tanaka2, Masakazu Yasuda2, Tomohiro Yamasaki2, Satoshi Watanabe2, Mutsumi Iwamoto2, Atsunori Okamura2, Heitaro Watanabe2
Sakurabashi Watanabe Hospital, Japan1, Sakurabashi Watanabe Advanced Healthcare Hospital, Japan2
Clinical Information
Relevant Clinical History and Physical Exam
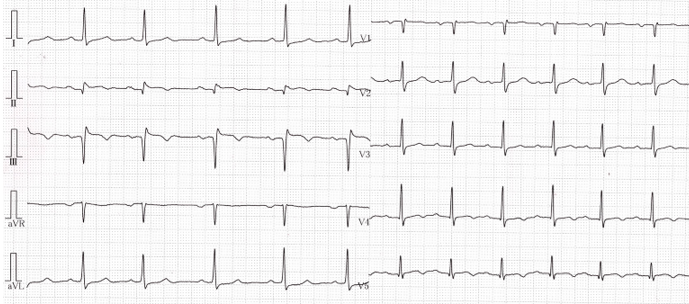
A 75-year-old male was admitted to another hospitalwith a rest chest pain. ST-segment elevation in the inferior leads indicatedacute myocardial infarction. Coronary angiography revealed two-vessel disease involvingthe RCA and the LAD. Revascularization was attempted on the culprit lesion of theRCA, but due to the forward origin of the RCA, guiding catheter could notmaintain coaxial position, resulting in procedural failure.
 2CAGLCA.mp4
2CAGLCA.mp4
2CARRCA.mp4
2PCIRCA.mp4
Relevant Test Results Prior to Catheterization
An electrocardiogram showed QS pattern in theinferior leads, and creatin kinase, as a cardiac enzyme, peaked at 951 U/L andsubsequently declined.
Relevant Catheterization Findings
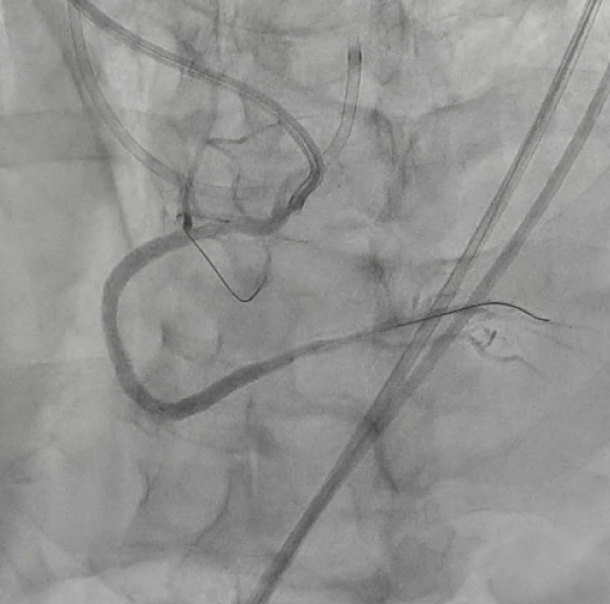
Coronary angiography revealed that the RCAof the middle-part was occluded. Additionally, a sub-total occlusion wasobserved in the middle-part of the LAD. An urgent PCI to the RCA was performed,but the backup force was also poor, so the procedure was so difficult. Weconsidered that PCI to the RCA was not essential in acute phase, so weperformed to PCI to the LAD, which was the donor artery for collateralcirculation to the RCA. After one month, re-PCI to RCA was performed.
4RCAPCI.mp4
4LADPCI3.mp4
Interventional Management
Procedural Step
An 8Fr guiding catheter was inserted intothe RCA from the right femoral artery. By performing the anchor balloontechnique, the guiding catheter became stable, and guidewire was advanced intothe occluded lesion. However, due to insufficient information of the distallesion, we switched to a retrograde approach to improve distal visualization.Tip injection through the microcatheter at the third septal branch showed aconnection to the distal RCA, and the floppy wire passed through to Seg4PD. Theretrograde wire which reached the distal end of the lesion was used as amarker, and the antegrade intermediate wire could be passed through the occludedlesion using the kissing wiring technique. After intravascular ultrasound observation,a drug-eluting stent was implanted from RCA distal to proximal, and normalantegrade blood flow was achieved.
5RCA2.mp4
5RCA4.mp4
5RCA7.mp4
Case Summary
We report a case in which revascularizationwas performed using a retrograde approach in the subacute phase of an acute inferiormyocardial infarction. Anatomical features such as the forward origin of theRCA and the coronary tortuosity made revascularization difficult using only theantegrade approach. The procedure was completed successfully by an anchorballoon technique and a distal visualization via a retrograde wire. Even in theacute phase of myocardial infarction, it is important to consider a retrogradeapproach if necessary.