Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_005
Simple Thrombectomy and Catheter-Directed Thrombolysis for Acute Upper Extremity Limb Ischemia: A Single-Center Case Series
By Imam Kukuh Darmawan, Gagah Buana Putra, Firman Tedjasukmana, Dian Larasati Munawar, Agus Riawan, Muhammad Munawar
Presenter
Imam Kukuh Darmawan
Authors
Imam Kukuh Darmawan1, Gagah Buana Putra1, Firman Tedjasukmana1, Dian Larasati Munawar1, Agus Riawan1, Muhammad Munawar1
Affiliation
Binawaluya Cardiac Center, Indonesia1
View Study Report
CASE20251107_005
Endovascular - Thrombus Removal Devices and Techniques
Simple Thrombectomy and Catheter-Directed Thrombolysis for Acute Upper Extremity Limb Ischemia: A Single-Center Case Series
Imam Kukuh Darmawan1, Gagah Buana Putra1, Firman Tedjasukmana1, Dian Larasati Munawar1, Agus Riawan1, Muhammad Munawar1
Binawaluya Cardiac Center, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
This case series describes two complex presentations of acute upper limb ischemia;Case 1: A 87-year-old female with atrial fibrillation, dual-chamber pacemaker, developed sudden pain and classic ischemic features.Case 2: A 58-year-old male with heart failure-reduced ejection fraction, pre-existing apical LV thrombus, coronary intervention history, diabetes, and renal dysfunction presented with acute limb symptoms.Both patients manifested classic “5 P’s” of ALI and Rutherford Class IIa.

Relevant Test Results Prior to Catheterization
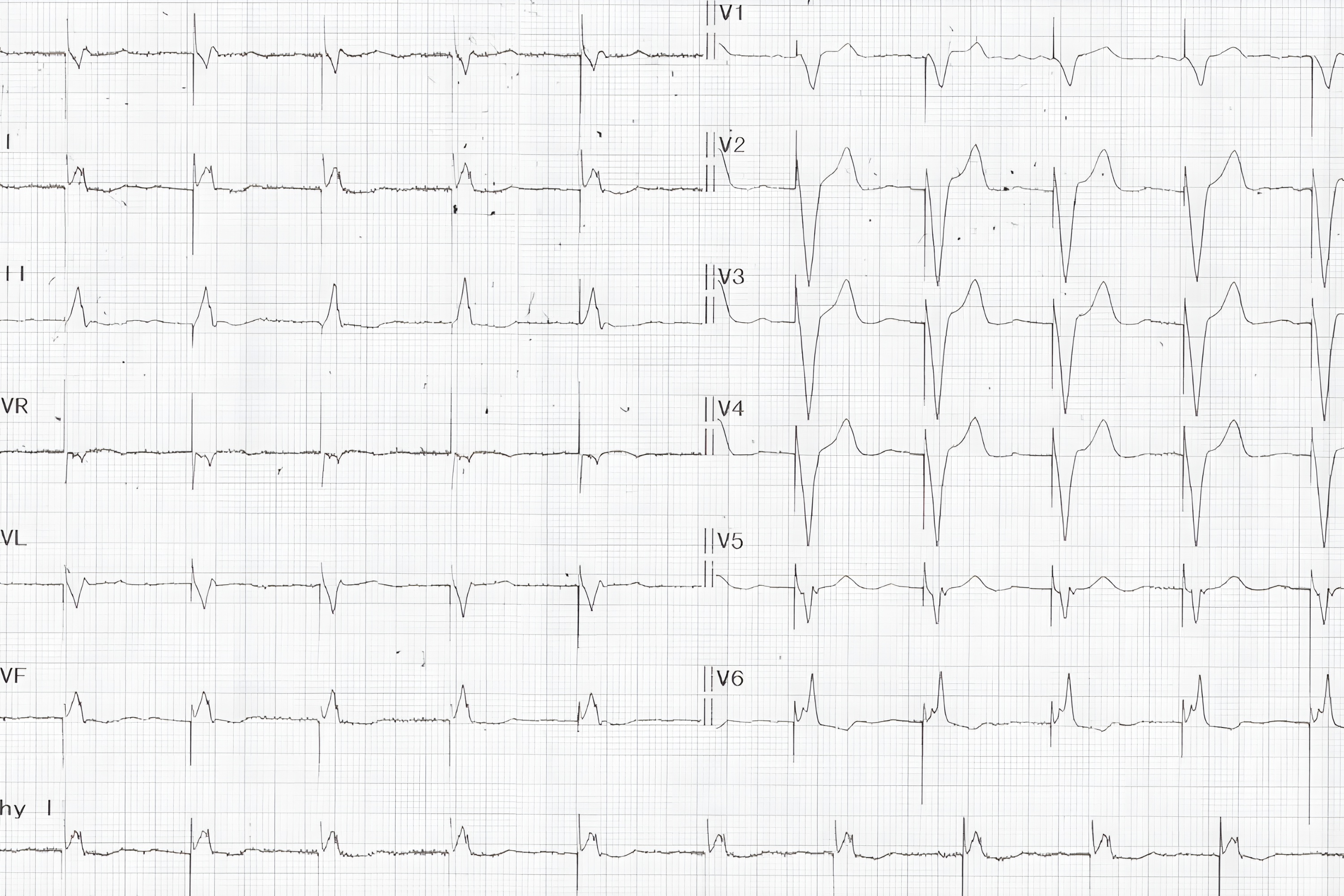
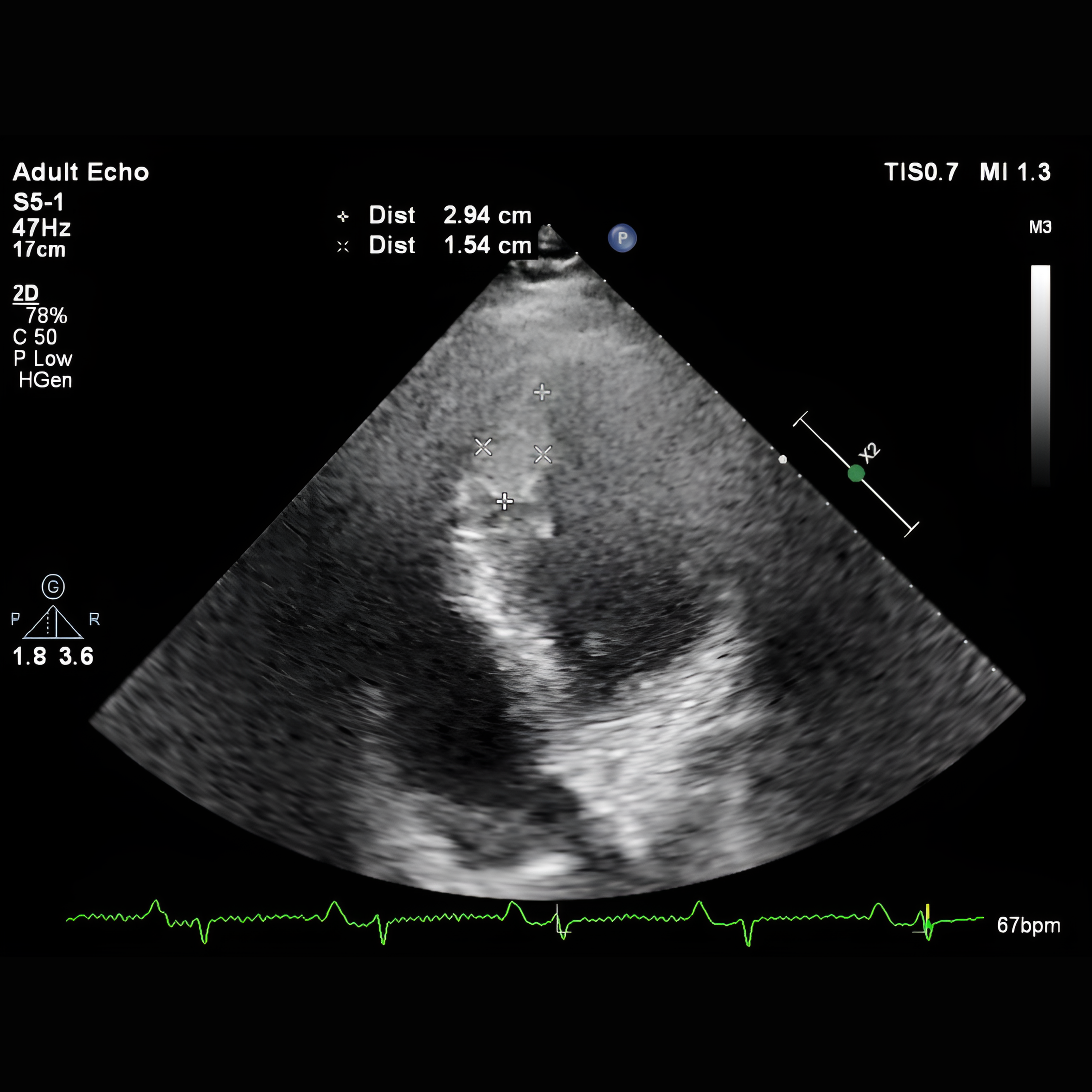
Laboratory testing revealed markedly elevated D-dimer (>3 g/mL). In case 1, the electrocardiogram (ECG) revealed atrial fibrillation accompanied by ventricular pacing spikes (Figure 2). CT angiography showed a total occlusion in the right brachial artery, which wasn’t done in case 2 to prevent a higher contrast exposure. Echocardiography was performed to determine the source of embolism and found a large LV thrombus in the apical segment (Figure 3).
Relevant Catheterization Findings
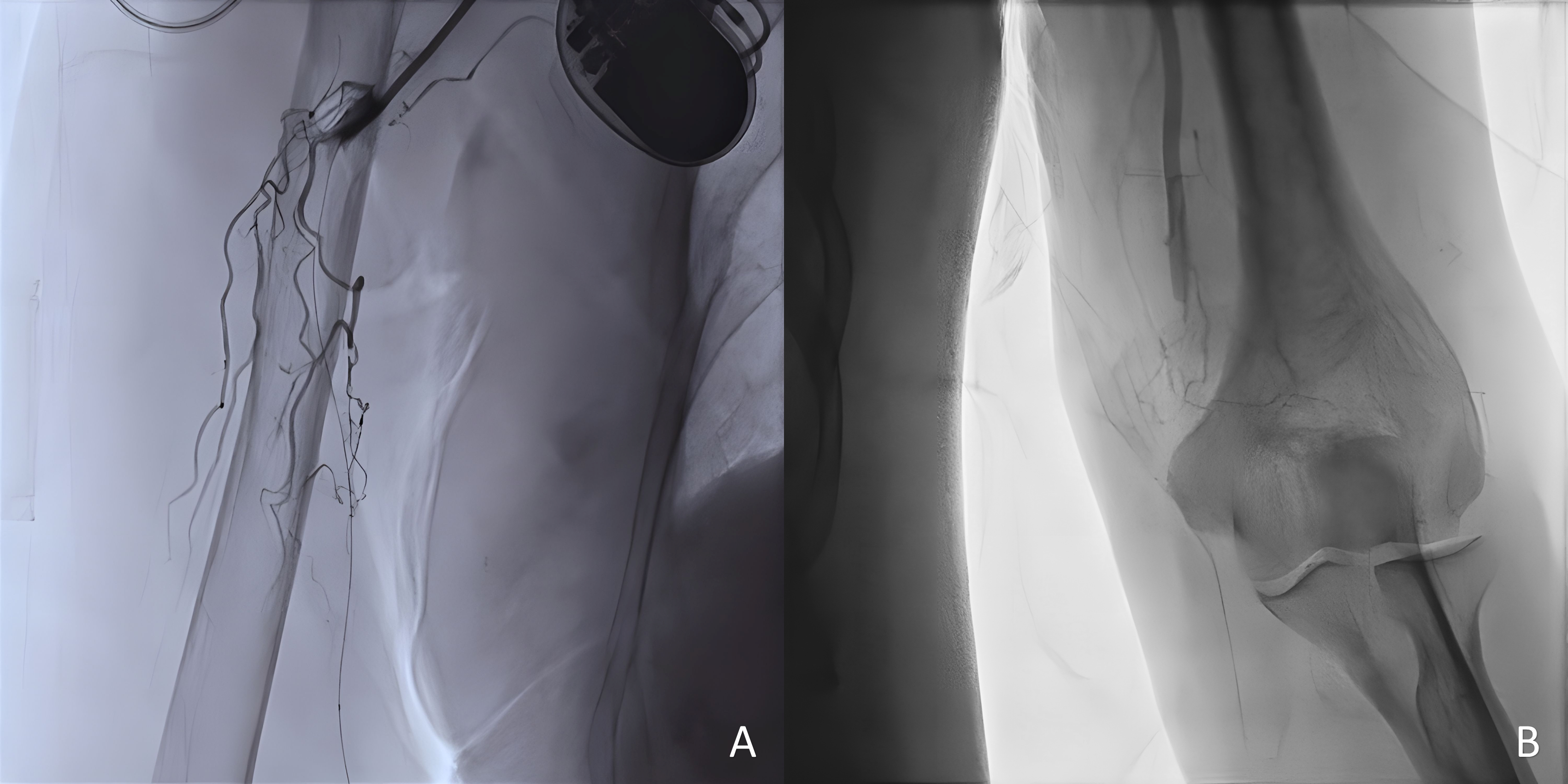
AP-frontal angiography in all of the cases confirmed mid-distal brachial artery occlusion, alongside an existing collateral vessel, with a difference in the affected arm side; left (Figure 4A) and right (Figure 4B).
Interventional Management
Procedural Step
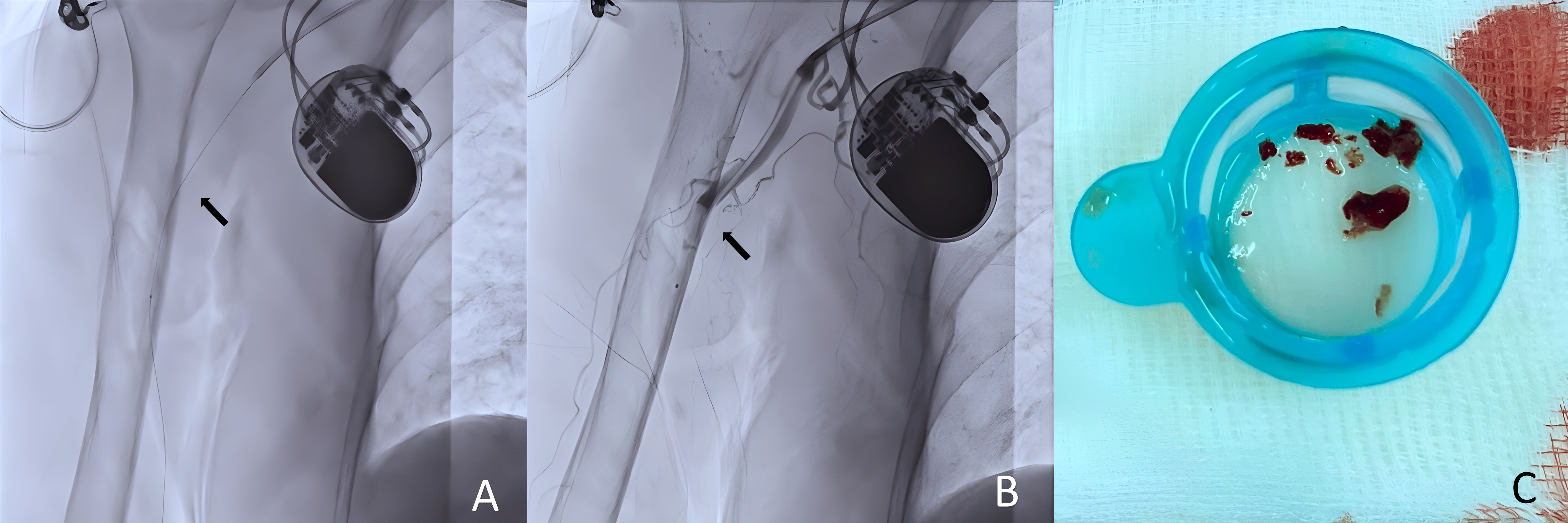
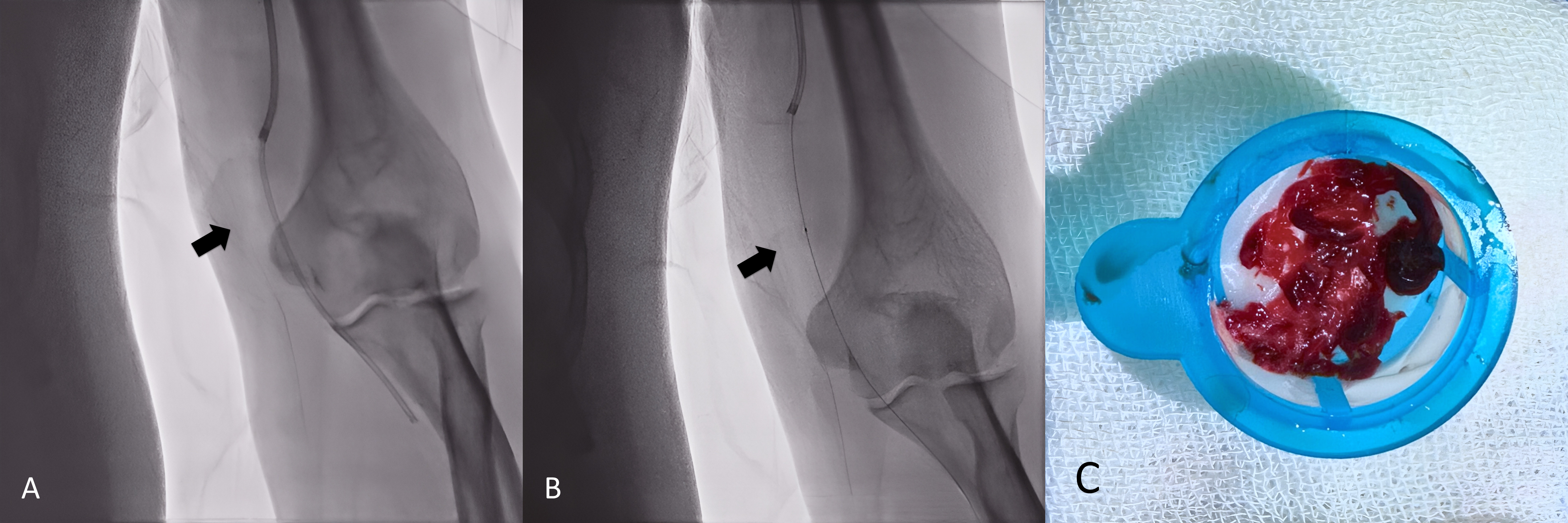
Interventions utilized a 6 Fr JR 3.5 guiding catheter via the left femoral artery, avoiding double-puncture access to minimize bleeding. Simple manual thrombus aspiration employed a 7 Fr Thrombuster II and 5 Fr Heartrail II ST01 for efficient removal. Catheter-directed thrombolysis employed alteplase (initial 4 mg bolus, followed by 1 mg/h over 24 hours) delivered directly into the thrombus via coronary thrombosuction or a guiding catheter (Figure 5-6.A), tailored for renal function preservation, with <20 mL of contrast used in one case. Serial angiography confirmed successful restoration of brachial, radial, and palmar arch flow, with TIMI-3 grade patency (Figure 5-6.B), with thrombus particles collected after thrombus retrieval (Figure 5-6.C). Only minimal transient bleeding occurred in the elderly case. Both patients were discharged on appropriate oral anticoagulation.
Case Summary
This combined approach, simple thrombus aspiration followed by catheter-directed, targeted thrombolysis, is simple, safe, and effective for ALI in patients with high thrombotic risk and comorbidities, including heart failure, diabetes, and renal dysfunction. It enables minimal contrast exposure and low complication rates. Individualized anticoagulation and dose adjustments are critical, particularly in elderly patients. Early diagnosis and intervention are vital for limb salvage and favorable outcomes.