Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_004
Calcified Triple-Vessel Disease With Balloon Uncrossable Lesion
By Chun Yu Fung
Presenter
Chun Yu Fung
Authors
Chun Yu Fung1
Affiliation
Tuen Mun Hospital, Hong Kong, China1
View Study Report
CASE20251107_004
Coronary - Complex PCI - Calcified Lesion
Calcified Triple-Vessel Disease With Balloon Uncrossable Lesion
Chun Yu Fung1
Tuen Mun Hospital, Hong Kong, China1
Clinical Information
Relevant Clinical History and Physical Exam
78/MBackground of hypertension, poorly controlled diabetes mellitus and hyperlipidemia. Paroxysmal AF on NOAC Admitted for acute pulmonary oedema.Required 5L O2 on admission. Started lasix and TNG infusion.Coronary angiogram: calcified triple vessels disease.Consulted CTS and turned down for CABG.
Relevant Test Results Prior to Catheterization
ECG: no acute ischemic change Echo: LVEF 63%. No RWMA. Valves unremarkable NTproBNP: 6020TnI 71 > 126
Relevant Catheterization Findings
•Very calcified vessels •LM: diffuse disease •LAD: pLAD and mLAD severe stenosis •LCx: mLCx critical stenosis •RCA: dominant, mRCA critical lesion
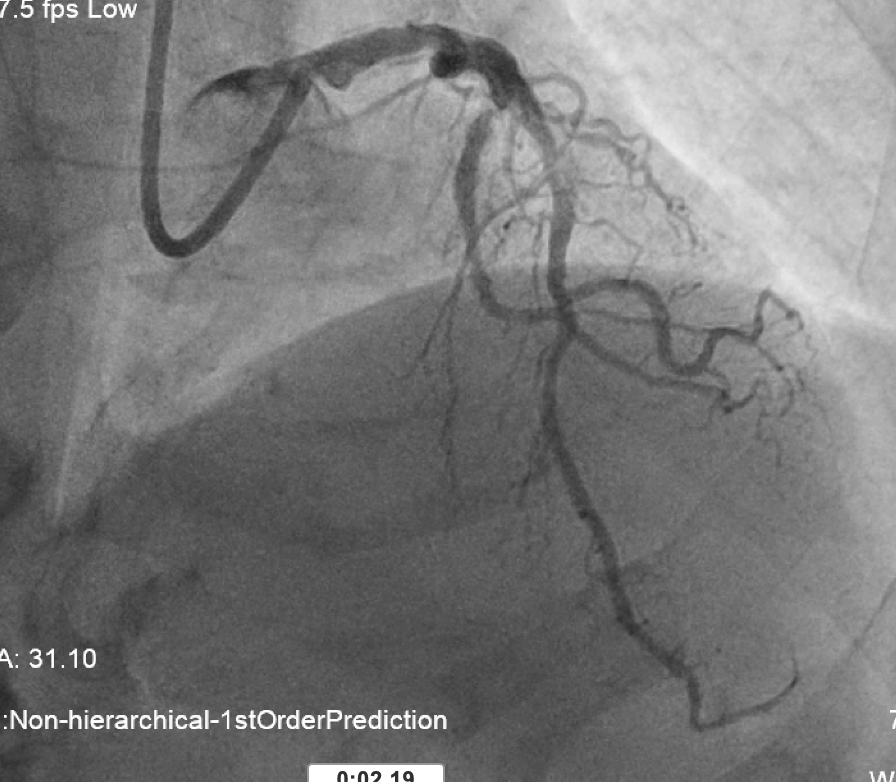
 L system coro 2.mov
L system coro 2.mov
L system coro 1.mov
Interventional Management
Procedural Step
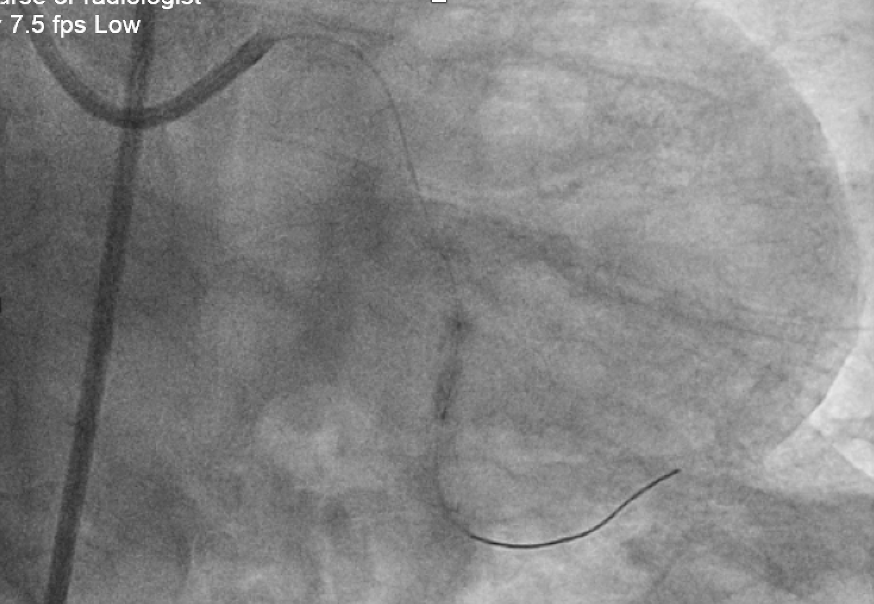
Rotablation assisted PCI to p-dRCA and shockwave assisted PCI to p-mLAD done. Attempted to predilated lesion with semi-compliant 1.5 and 1.0 balloon, both balloons ruptured, unable to deliver NC 1.5/10 across lesion.Arranged stage procedure
Left femoral access EBU 3.5 7Fr GCSion Blue + microcatheter (Corsair Pro XS) wired to LCx Fail to advance microcatheter
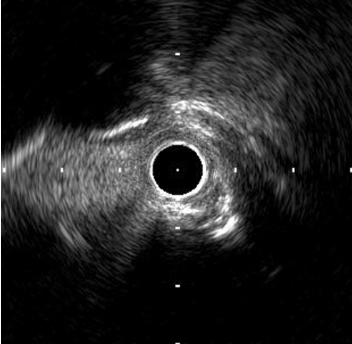
ivus to LAD.mov
ivus to LCx.mov
rotablation to LCx.mov
Left femoral access EBU 3.5 7Fr GCSion Blue + microcatheter (Corsair Pro XS) wired to LCx Fail to advance microcatheter
Microcatheter placed as distal as possible, free hand wiring with Rotafloppy wire
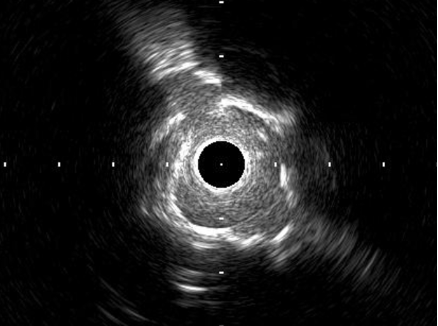
Rotational atherectomy with 1.25mm burr to LCxPoor expansion of NC balloon Further prepare lesion with shockwave 3.0.IVUS shows evidence of calcium fracture 3.0/15 stent deployed, followed by PSHP with NC 3.0 balloon Sion Blue redirected to LAD IVUS: concentric LM and pLAD calcification, 10 mm from mid LAD stent deployed 12 days ago
Rotational atherectomy with 1.75mm burr
Further prepare lesion with shockwave 3.5 and NC 3.5 balloon3.5 stent deployed at LM-mLAD
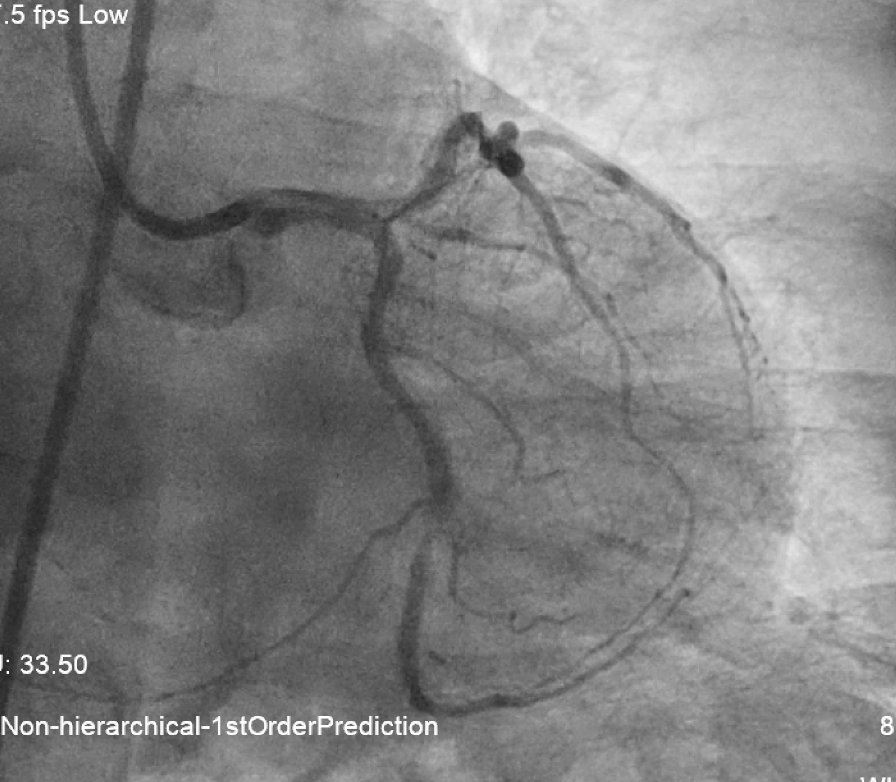
IVUS and angiogram show satisfactory stent expansion.
IVUS and angiogram show satisfactory stent expansion.
Case Summary
1. Algorithm for dealing with balloon uncrossable lesion. From serial balloon dilatation, plaque modification with microcathter to rotablation with free hand wiring2. Management of calcified lesion. Combination of rotablation with shockwave lithotripsy for extreme calcification. Assessment of lesion preparation with NC balloon expansion and IVUS