Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_003
Take a Detour in Critical LM Disease and Long Calcified LAD
By Yen-Lien Chou
Presenter
Yen-Lien Chou
Authors
Yen-Lien Chou1
Affiliation
Tri-Service General Hospital, Taiwan1
View Study Report
CASE20251107_003
Coronary - Complex PCI - Calcified Lesion
Take a Detour in Critical LM Disease and Long Calcified LAD
Yen-Lien Chou1
Tri-Service General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
64-year-old man, ex-smoker, Hx ofspontaneous ICH, HTN, and BPH
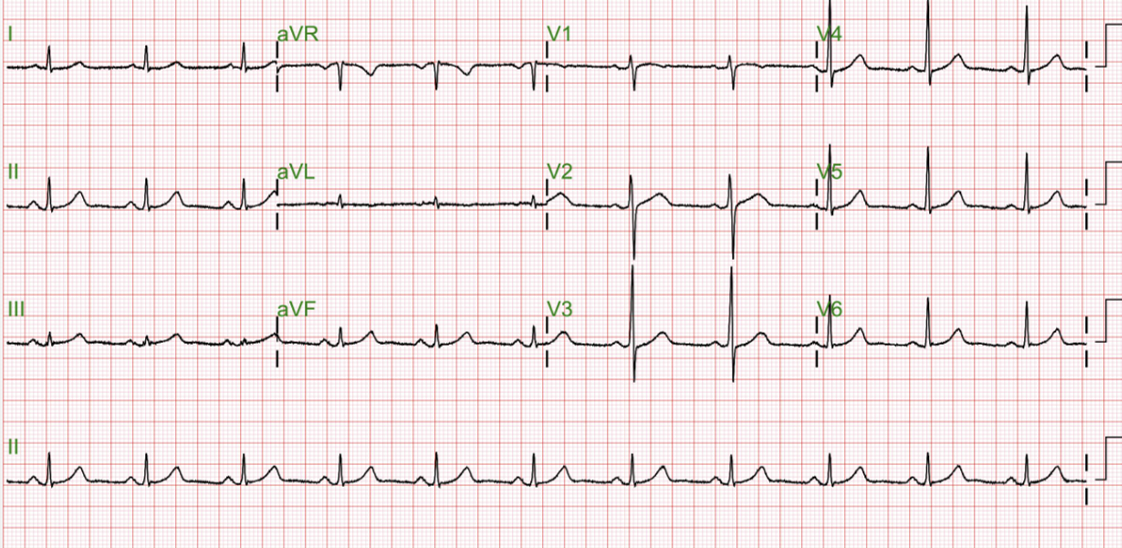
Relevant Test Results Prior to Catheterization
HDLC 44;LDLC 101;GLU 93; HBA1C5.5; CREA 0.9;AST 19;ALT 13
Relevant Catheterization Findings
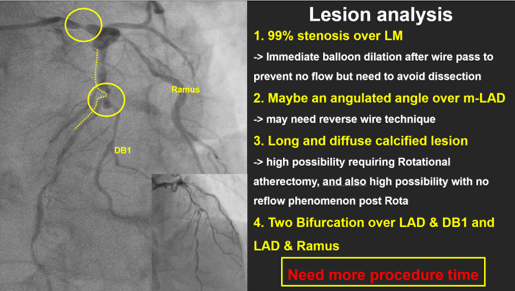
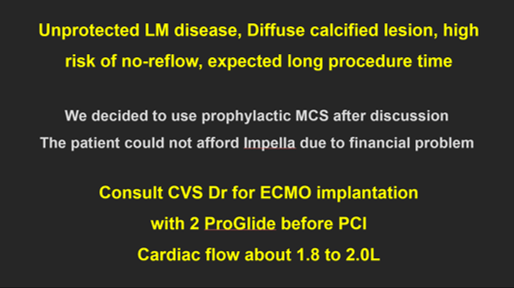
LM: D/3:discrete 99% stenosis, Medina (1,0,0) with LAD and LCx
 媒體1.mp4
媒體1.mp4
媒體2.mp4
媒體3.mp4
Interventional Management
Procedural Step
1. V-A mode ECMO was used for CHIP PCI
媒體4.mp4
媒體5.mp4
媒體6.mp4
Case Summary
*. Critical LM disease with longcalcified lesion may need more procedure time, prophylactic MCS should beconsidered