Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251107_002
When Success Turns Risky: An Unexpected Complication in RCA CTO PCI
By Hung Chi Su, Hsin-Fu Lee
Presenter
Hung Chi Su
Authors
Hung Chi Su1, Hsin-Fu Lee1
Affiliation
New Taipei Municipal Tucheng Hospital, Taiwan1
View Study Report
CASE20251107_002
Coronary - Complication Management
When Success Turns Risky: An Unexpected Complication in RCA CTO PCI
Hung Chi Su1, Hsin-Fu Lee1
New Taipei Municipal Tucheng Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
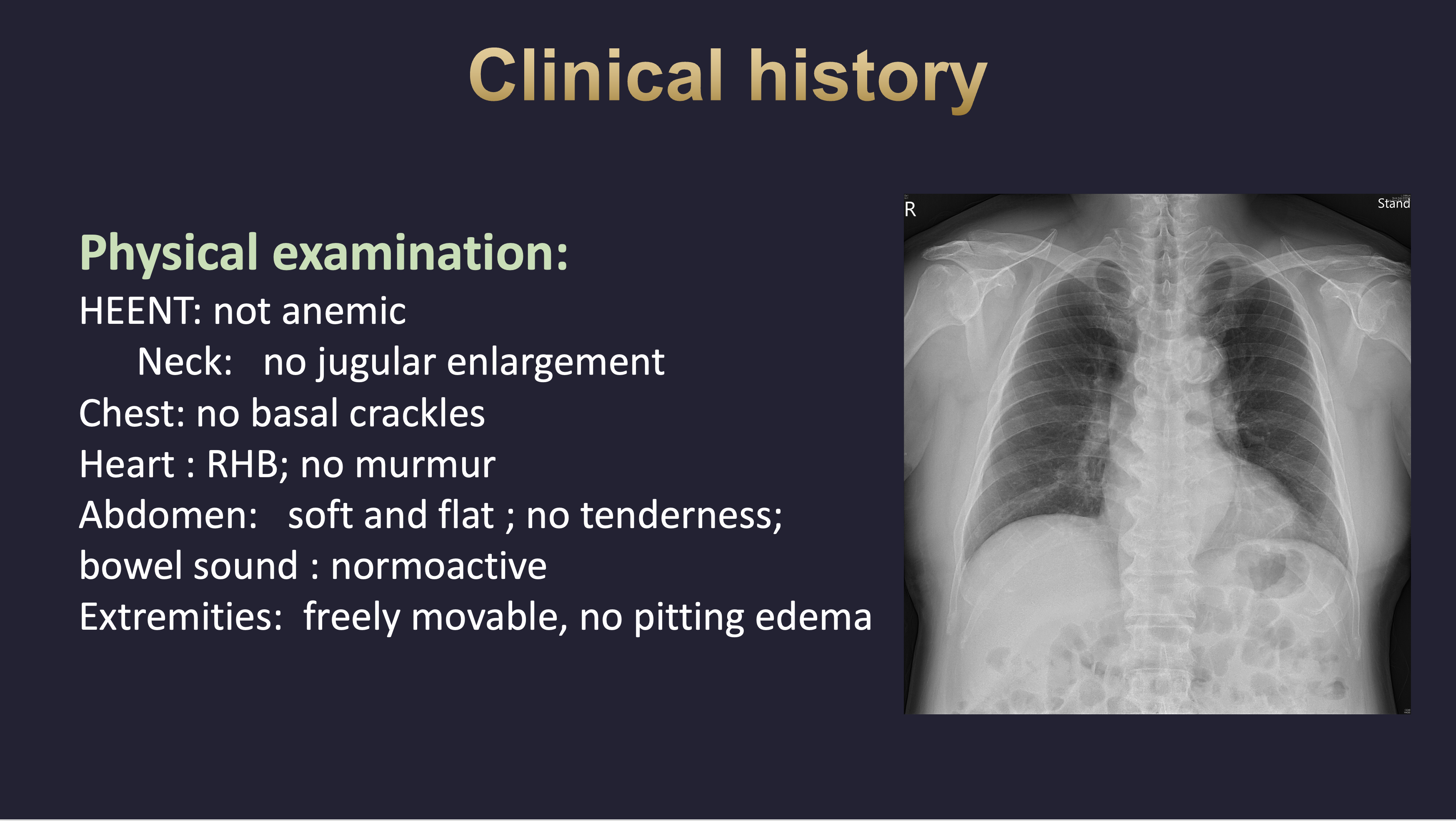
A 69-year-old man with type 2 diabetes mellitus, hypertension, and a history of right internal carotid aneurysm treated with a Flow Diverter presented with progressive dyspnea on exertion for several months. He visited our cardiovascular outpatient clinic, where physical examination revealed no cardiac murmur and no basal rales on auscultation.
Relevant Test Results Prior to Catheterization
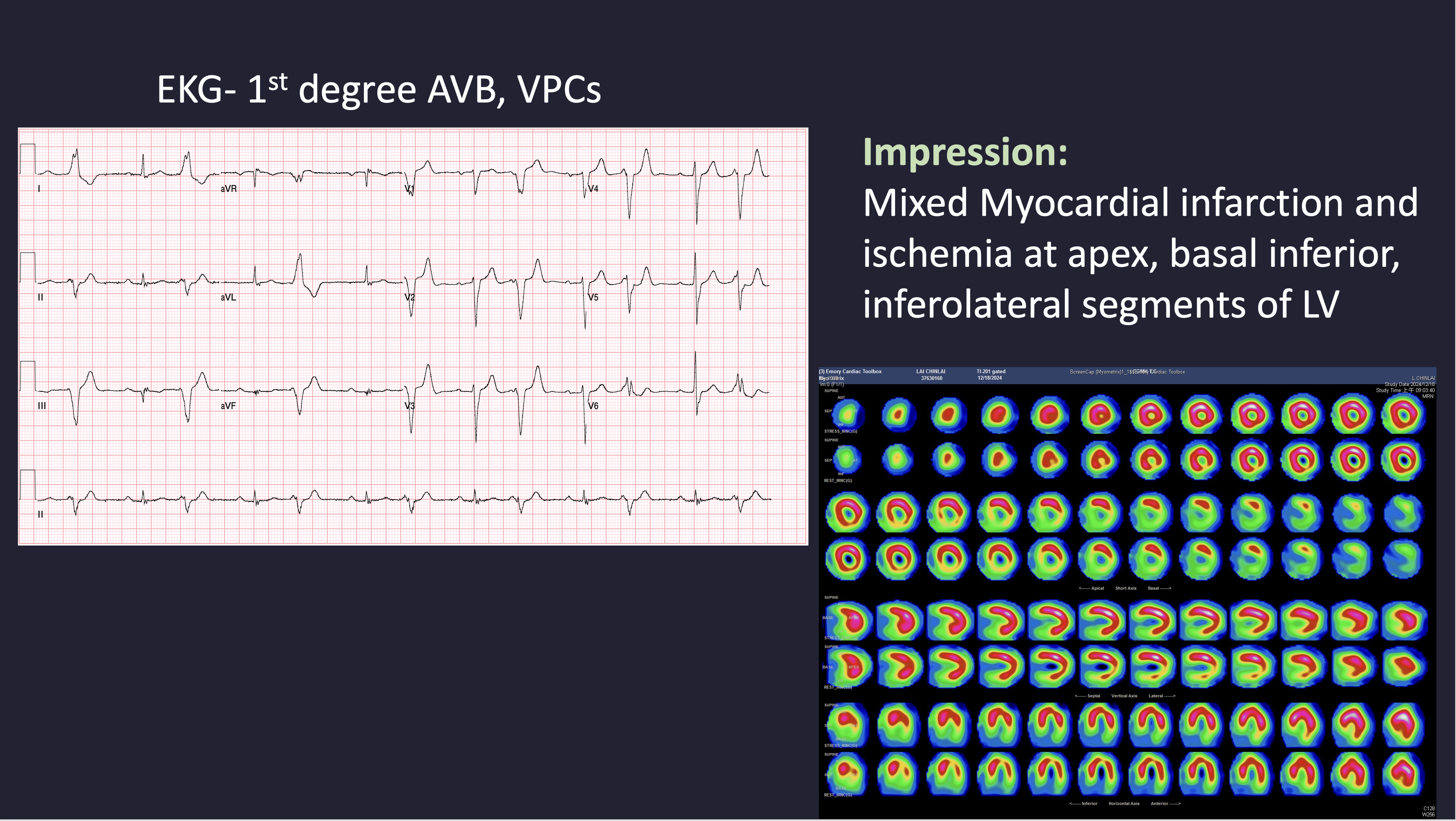
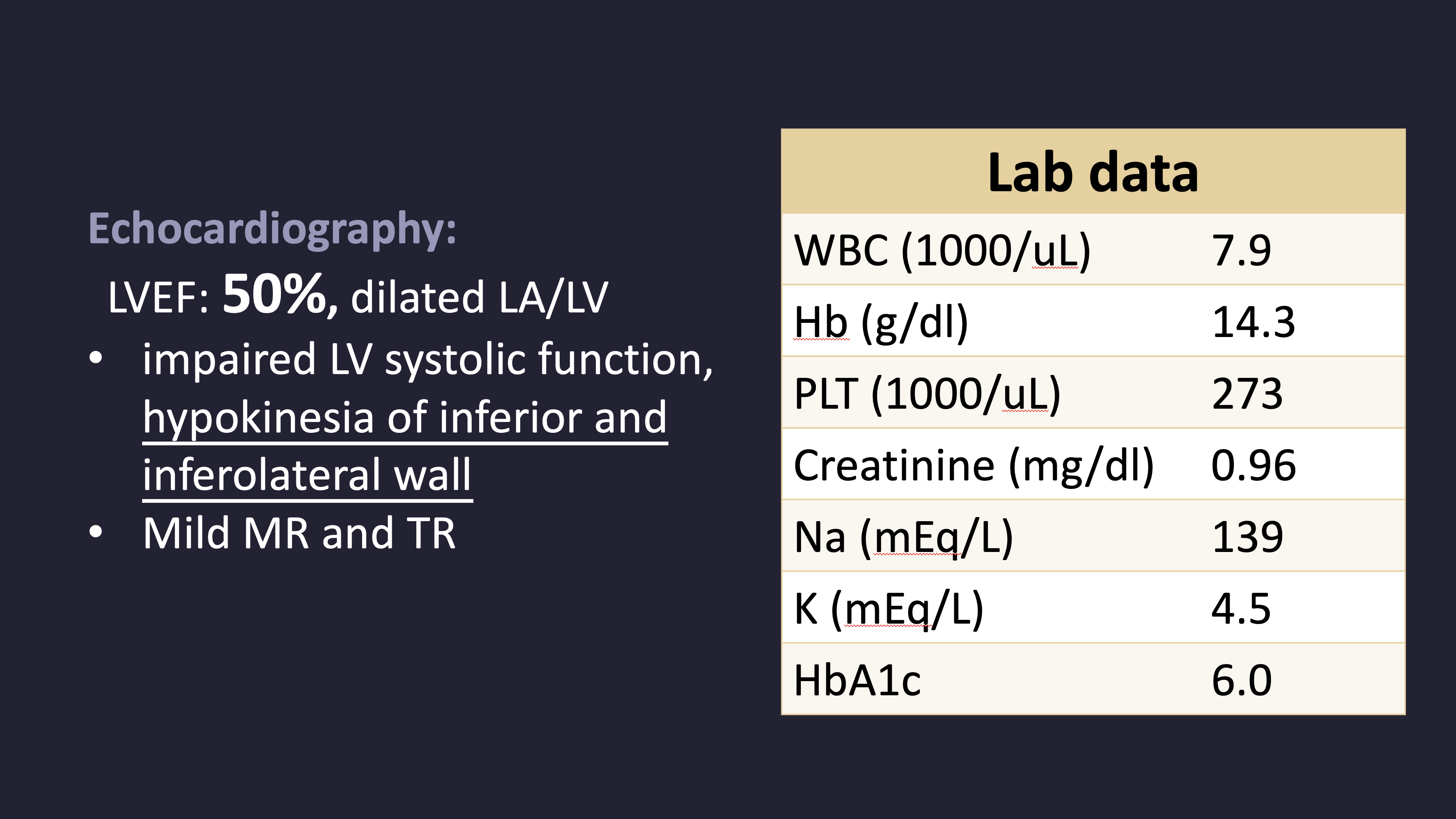
ECG revealed 1st degree atrioventricular block and frequent ventricular premature complexes. Echocardiography showed a LVEF of 50%, with dilation of the left atrium and ventricle, and hypokinesia of the inferior and inferolateral walls. Myocardial perfusion imaging demonstrated mixed infarction and ischemia involving the apex, basal inferior, and inferolateral segments. Laboratory tests showed creatinine 0.96 mg/dL, hemoglobin 14.3 g/dL, and platelet count 273 × 10³/μL.
Relevant Catheterization Findings
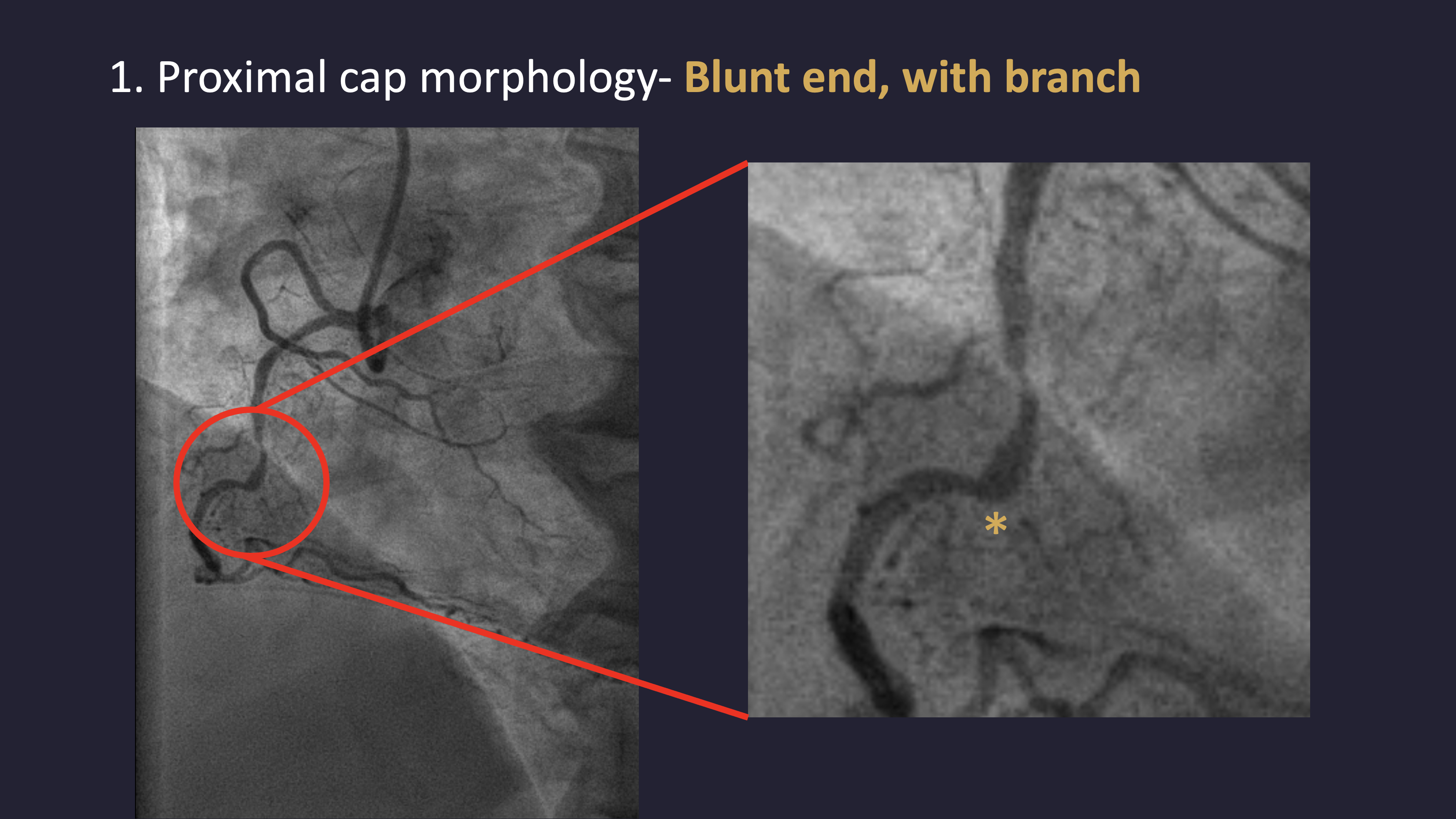
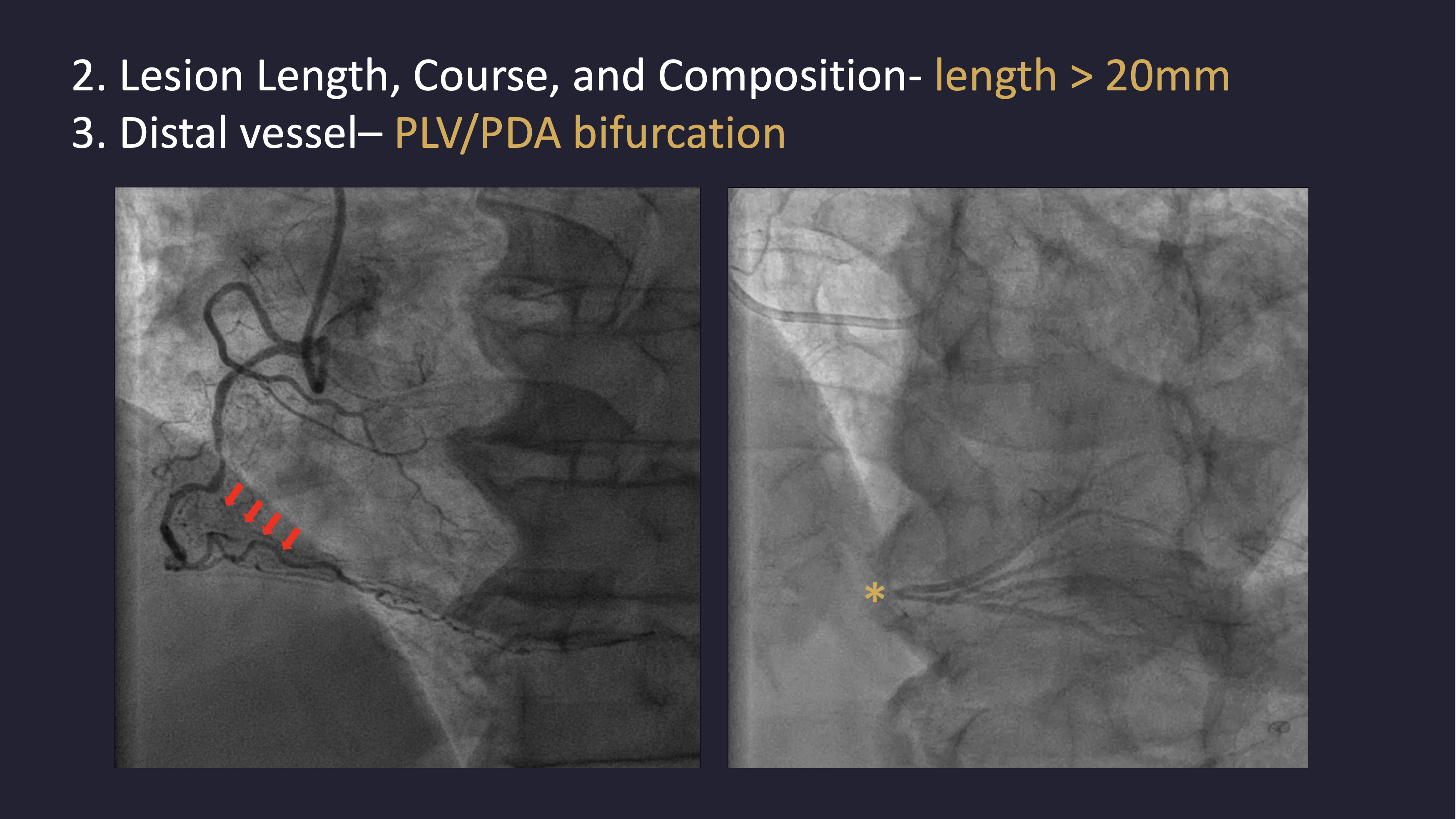
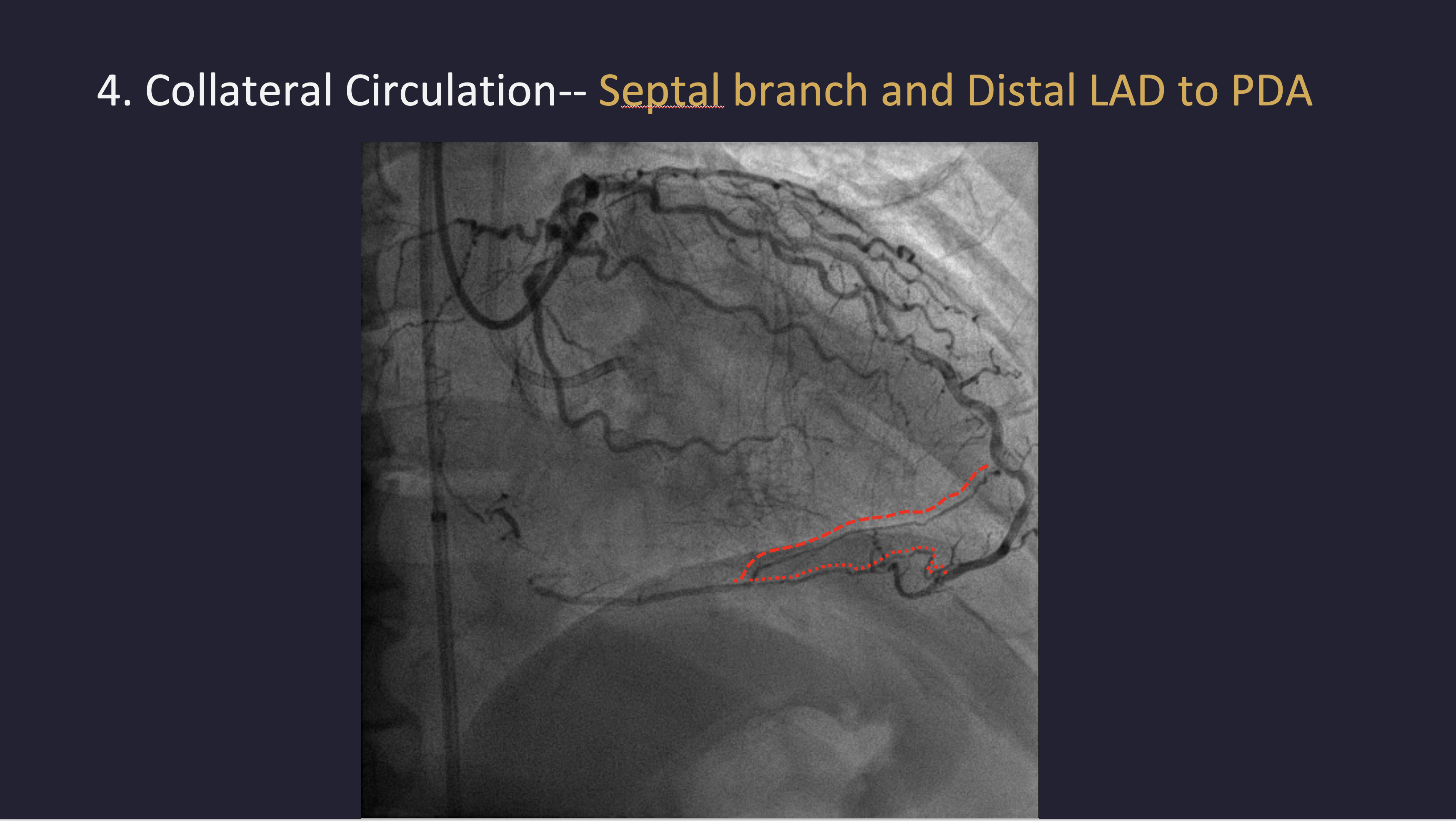
Left coronary angiography revealed mild plaquing in the LAD without significant stenosis and a critical lesion in the LCX. RCA angiography demonstrated a chronic total occlusion with a blunt proximal cap, lesion length greater than 20 mm, and distal bifurcation into the PLV and PDA. Collateral circulation from septal branches and the distal LAD to the PDA was identified.
 1.mov
1.mov
2.mov
3.mov
Interventional Management
Procedural Step
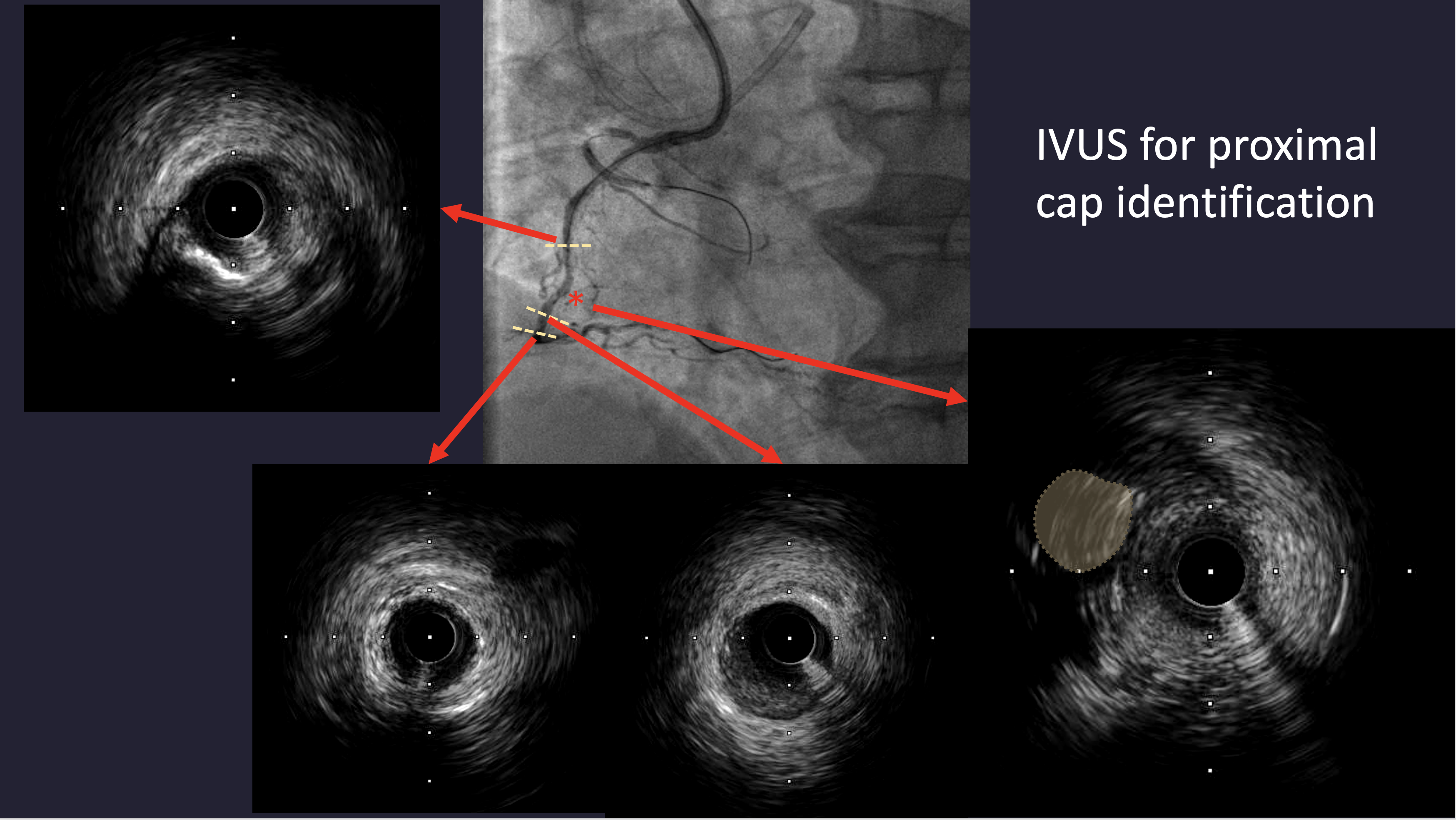
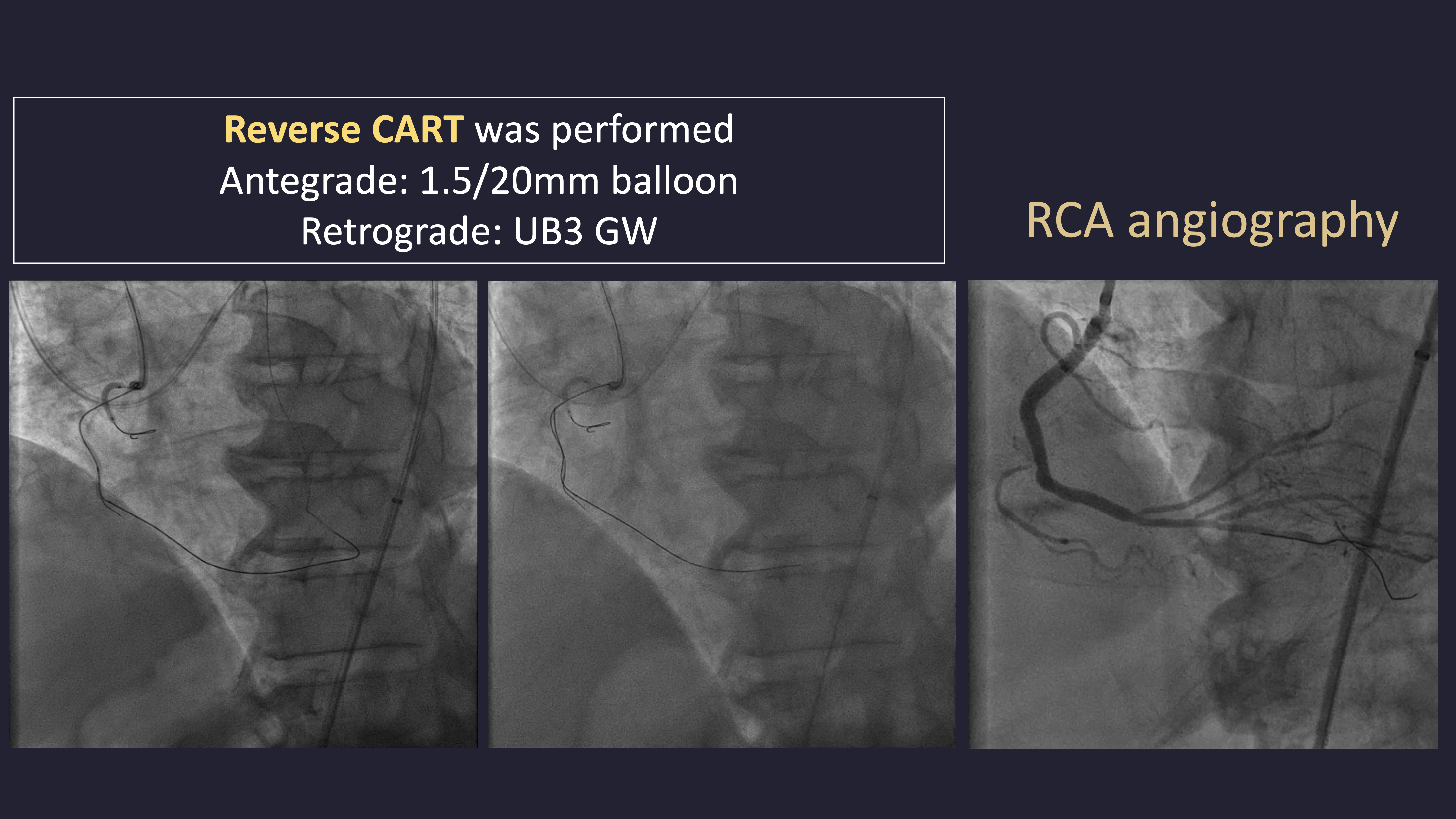
Dual arterial access was obtained for dual injection. The initial antegrade approach was attempted using a SION Blue wire and a 2.0 × 20 mm anchor balloon under IVUS guidance to identify the proximal cap, but antegrade wiring with UB3, Gaia Second, and Gaia Third failed to reach the distal cap. A retrograde approach through the distal septal branch to the PDA was then performed using a Finecross microcatheter and SION Black wire, followed by UB3 and Gaia Second/Third wires. Reverse CART was successfully achieved with a 1.5 × 20 mm balloon at the mid RCA, and wire externalization with RG3 was performed through a Guide Extension Catheter. POBA was done with 1.5 and 2.0 mm balloons, followed by DES implantation (2.5 × 48 mm and 3.5 × 33 mm). After the final RCA angiogram, the patient developed severe hypotension. Echocardiography revealed minimal pericardial effusion and LAD territory akinesia. LAD angiography showed acute total occlusion. Immediate balloon angioplasty and aspiration thrombectomy were performed, and IVUS was used to identify the cause of LAD closure. IVUS revealed a dissection flap in the mid LAD, suspected to be iatrogenic due to the cutting effect of the externalized RG3 wire despite microcatheter protection. An additional DES (3.0 × 48 mm) was deployed in the LAD, restoring TIMI 3 flow. The patient stabilized hemodynamically after intervention.

1.mov
2.mov
Case Summary
This case emphasizes the utility of IVUS in identifying the CTO proximal cap and confirming true lumen after Reverse CART. However, it also demonstrates a rare but serious complication—iatrogenic coronary dissection likely caused by the cutting effect of the externalized RG3 wire, even when protected by a retrograde microcatheter. Operators should remain vigilant for hemodynamic instability following complex CTO procedures and promptly evaluate for potential non-target vessel injury to ensure rapid management and optimal outcomes.