Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_048
Unusual Smooth Muscle Compression Causing Right Coronary Artery Ostial In-Stent Restenosis: A Successful Revascularization Case
By Chia-Han Tien, Hao-Yun Lo
Presenter
Chia-Han Tien
Authors
Chia-Han Tien1, Hao-Yun Lo1
Affiliation
Division of Cardiology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1
View Study Report
CASE20251106_048
Coronary - Complex PCI - In-Stent Restenosis
Unusual Smooth Muscle Compression Causing Right Coronary Artery Ostial In-Stent Restenosis: A Successful Revascularization Case
Chia-Han Tien1, Hao-Yun Lo1
Division of Cardiology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 71-year-old male with hypertension, hyperlipidemia, and diabetes presents with two months of worsening shortness of breath. He was diagnosed with left main and triple-vessel coronary artery disease in 2018 and declined bypass surgery, opting for percutaneous intervention. Drug-eluting stents were placed in the left main, left anterior descending, and in the totally occluded right coronary artery. Follow-up coronary angiography in 2025 showed severe right coronary ostial in-stent restenosis.


Relevant Test Results Prior to Catheterization
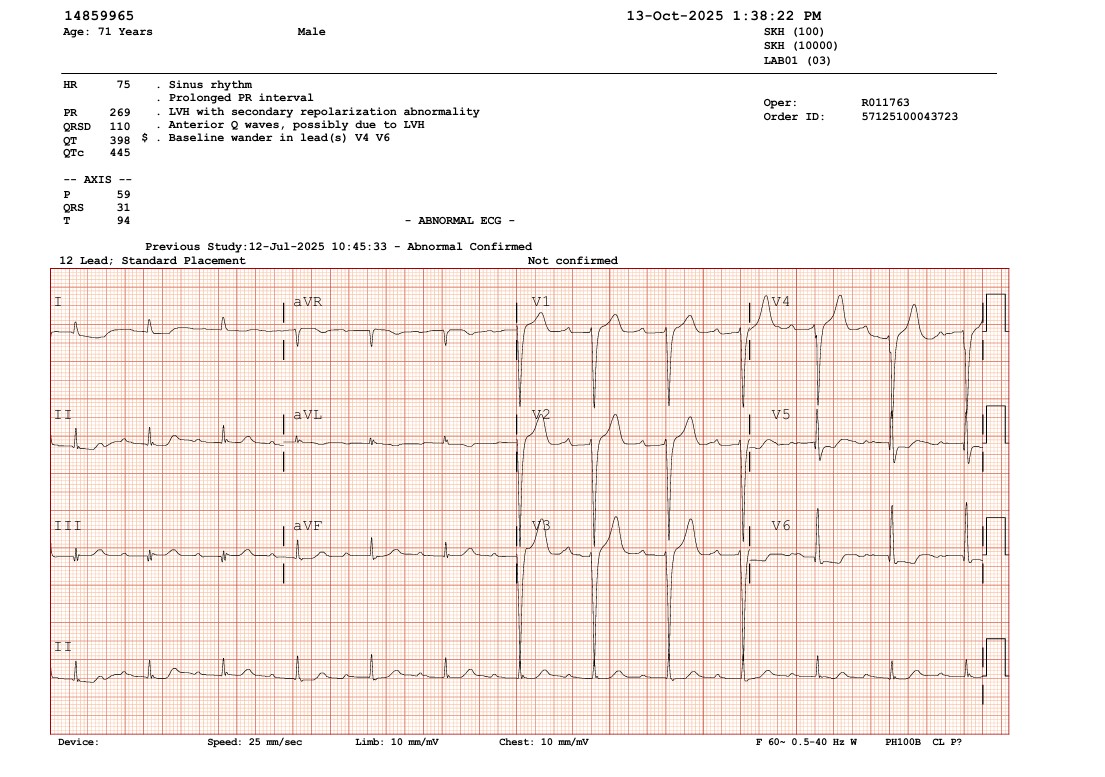
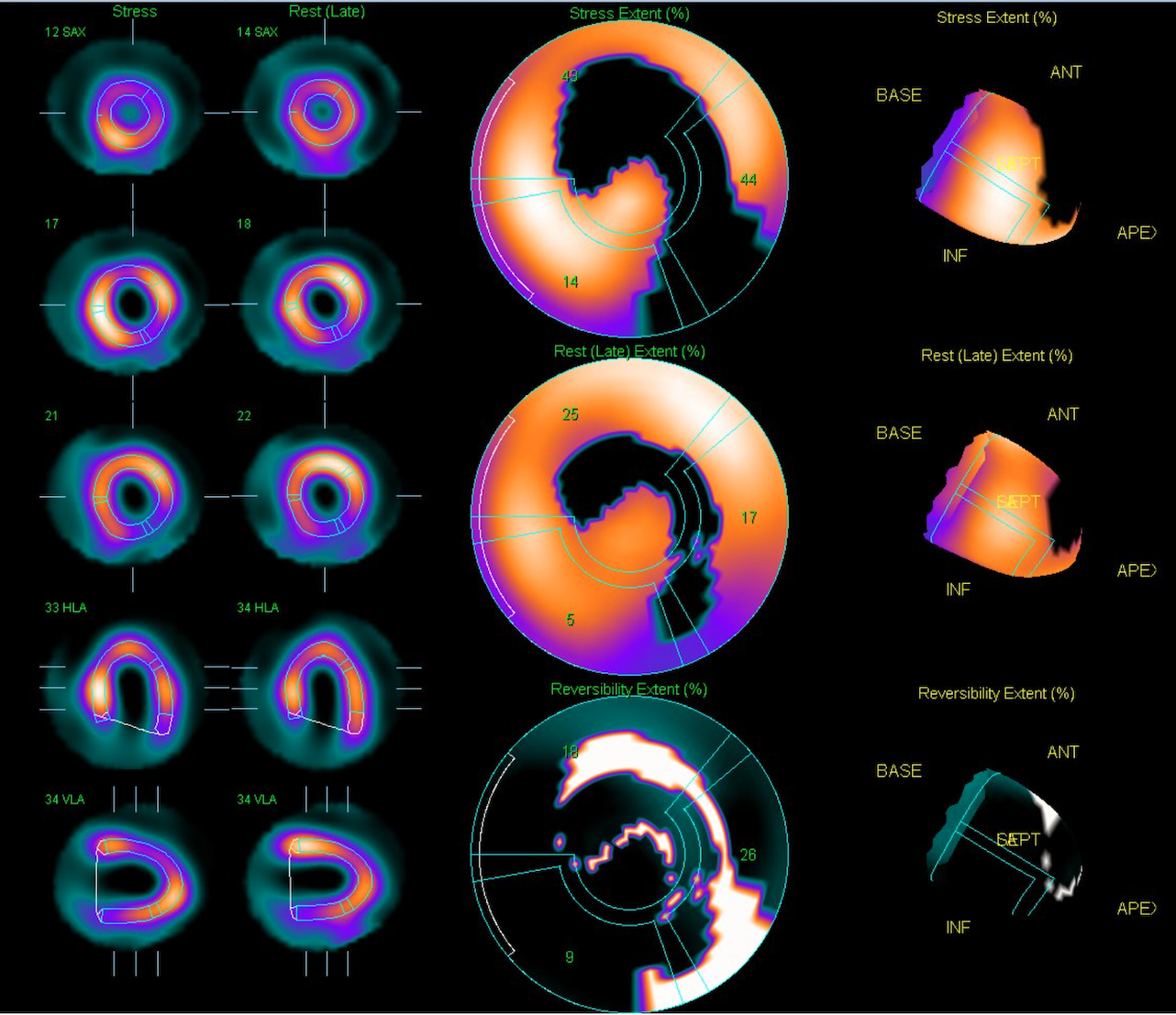
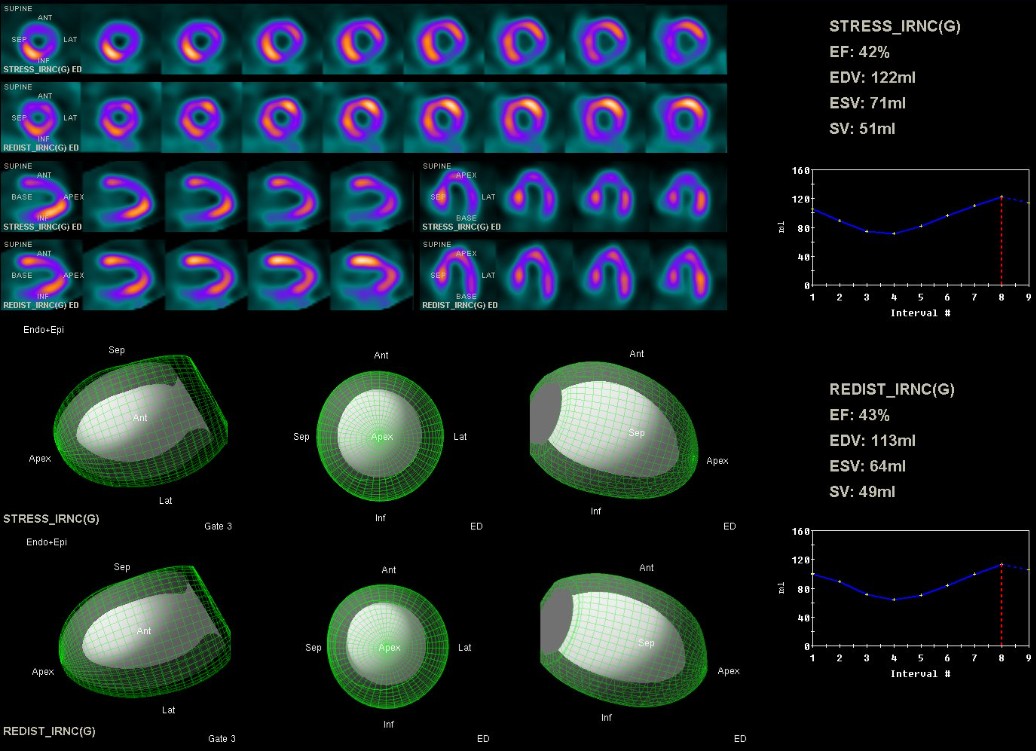
Echocardiography revealed inferior wall hypokinesis with a left ventricular ejection fraction of 47.1% by Simpson’s method. Admission electrocardiogram showed normal sinus rhythm without significant ST-T changes. Thallium-201 myocardial perfusion scan demonstrated ischemia in the apical, inferior, anterior, apical/mid-lateral, apical-anteroseptal, and basal-inferolateral walls, with a total ischemic extent of 38%.
Relevant Catheterization Findings
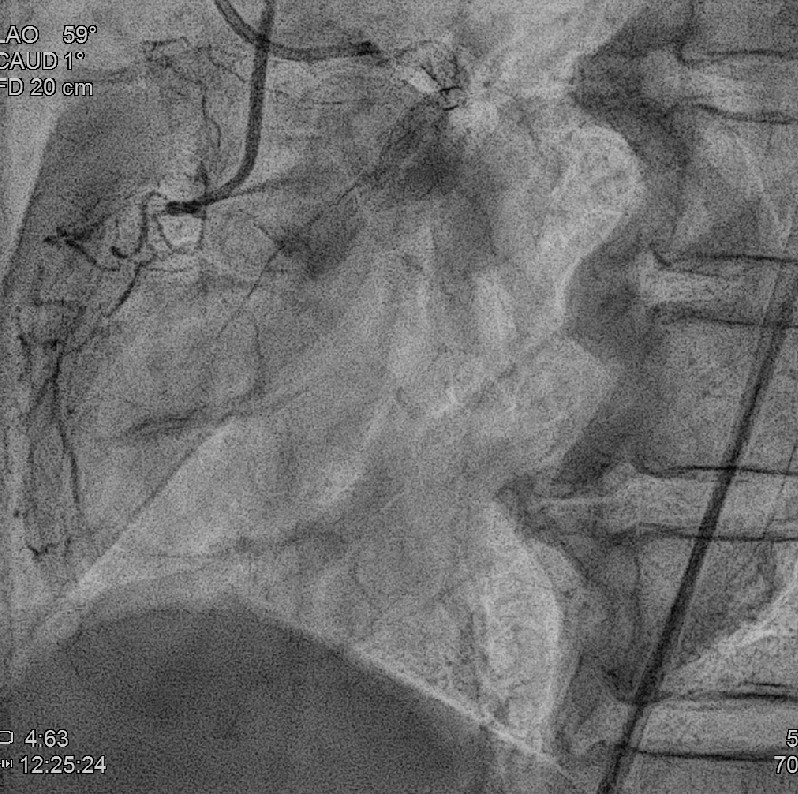
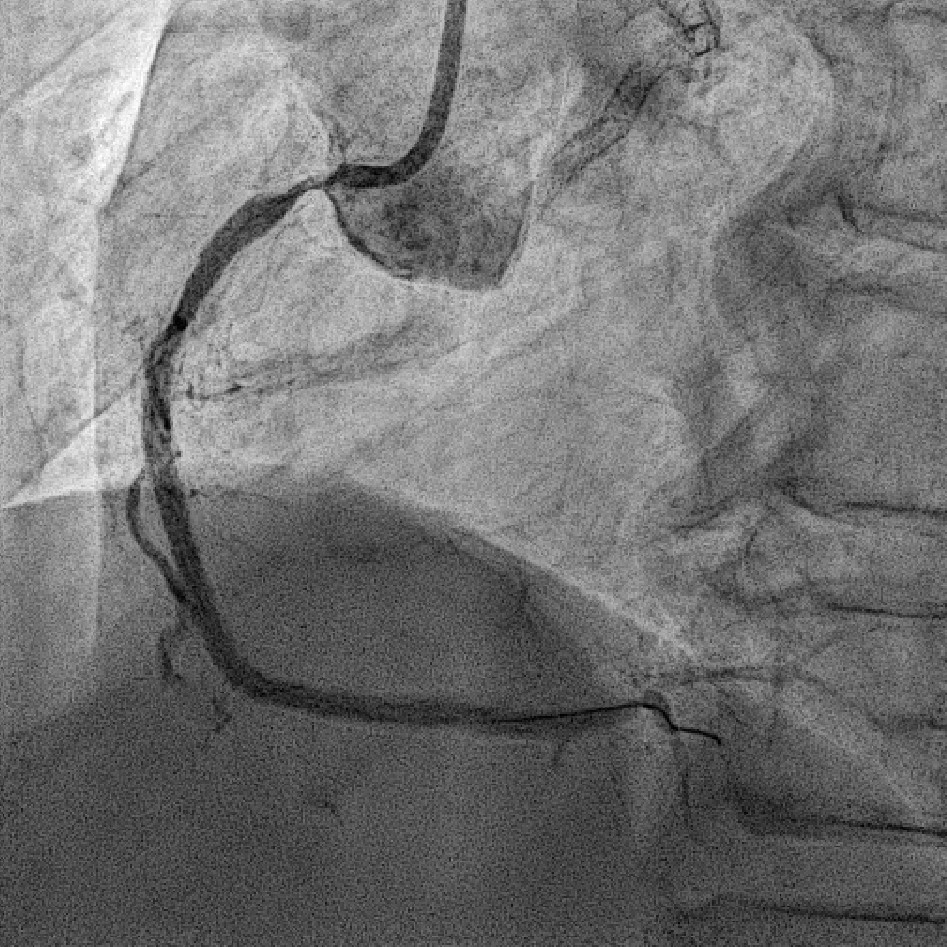
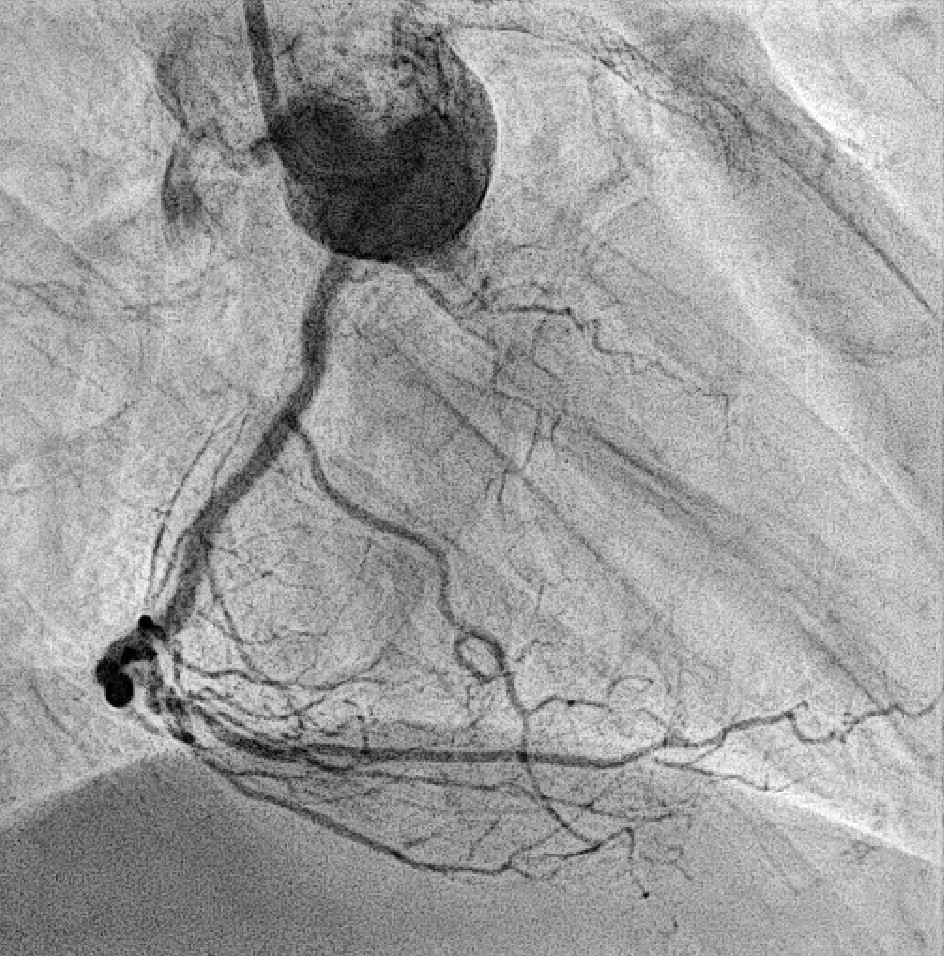
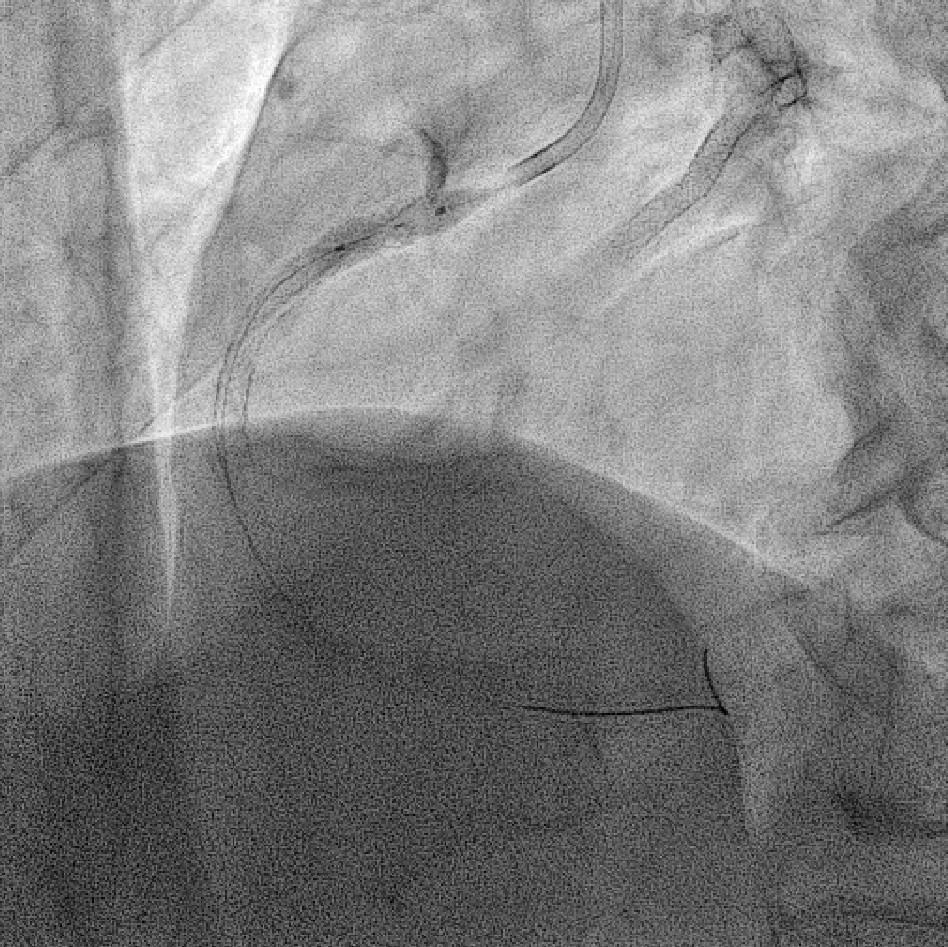
Coronary angiography revealed 81% in-stent restenosis at the right coronary artery ostium, worsened since February 2025. Proximal and mid RCA stents were patent; distal RCA was patent but smaller in caliber . Left main and LAD stents showed no progression, though 30–60% restenosis was seen in proximal to mid LAD. Left circumflex artery was nearly totally occluded from ostium to proximal segment, with preserved flow in mid and distal segments, similar to prior study.
Interventional Management
Procedural Step
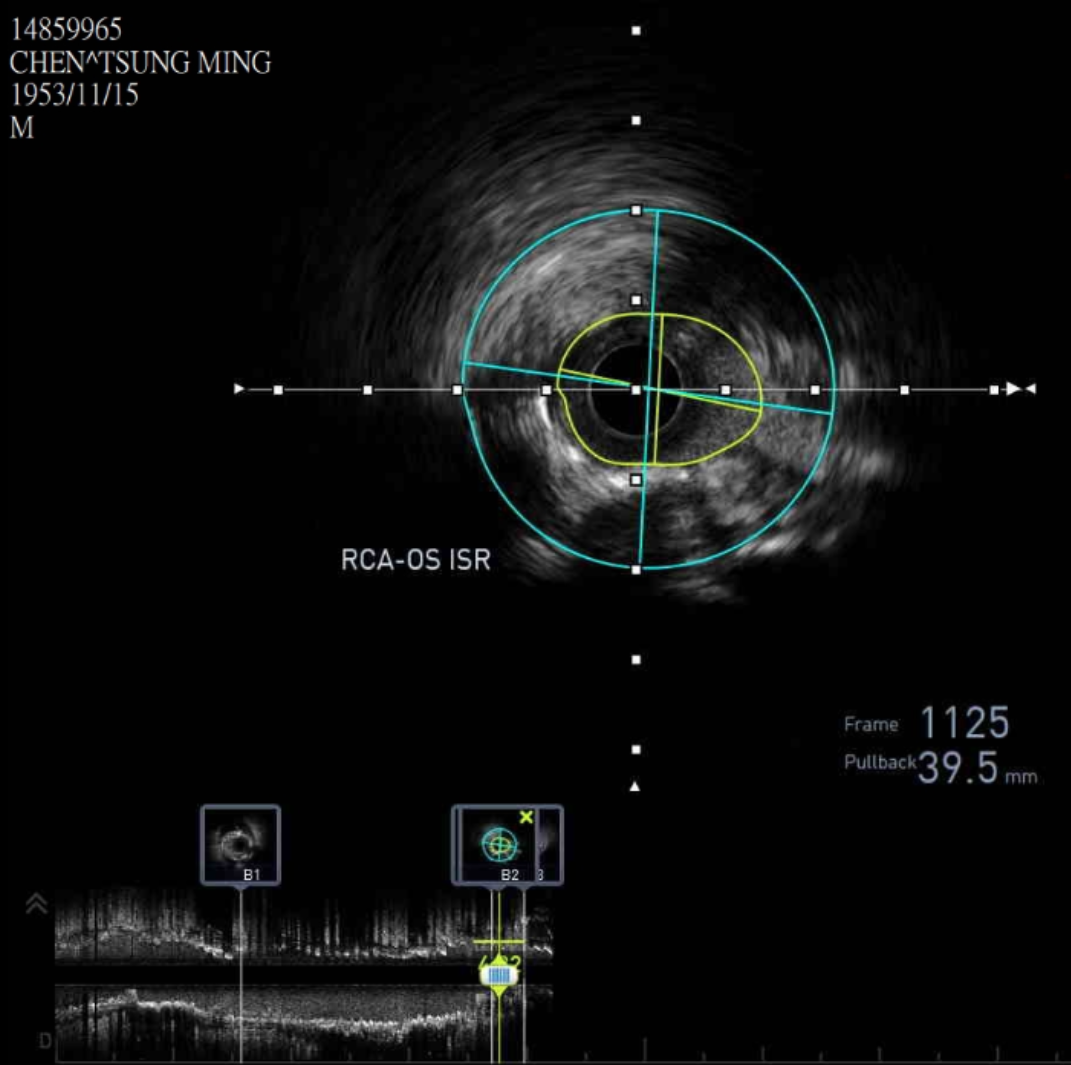
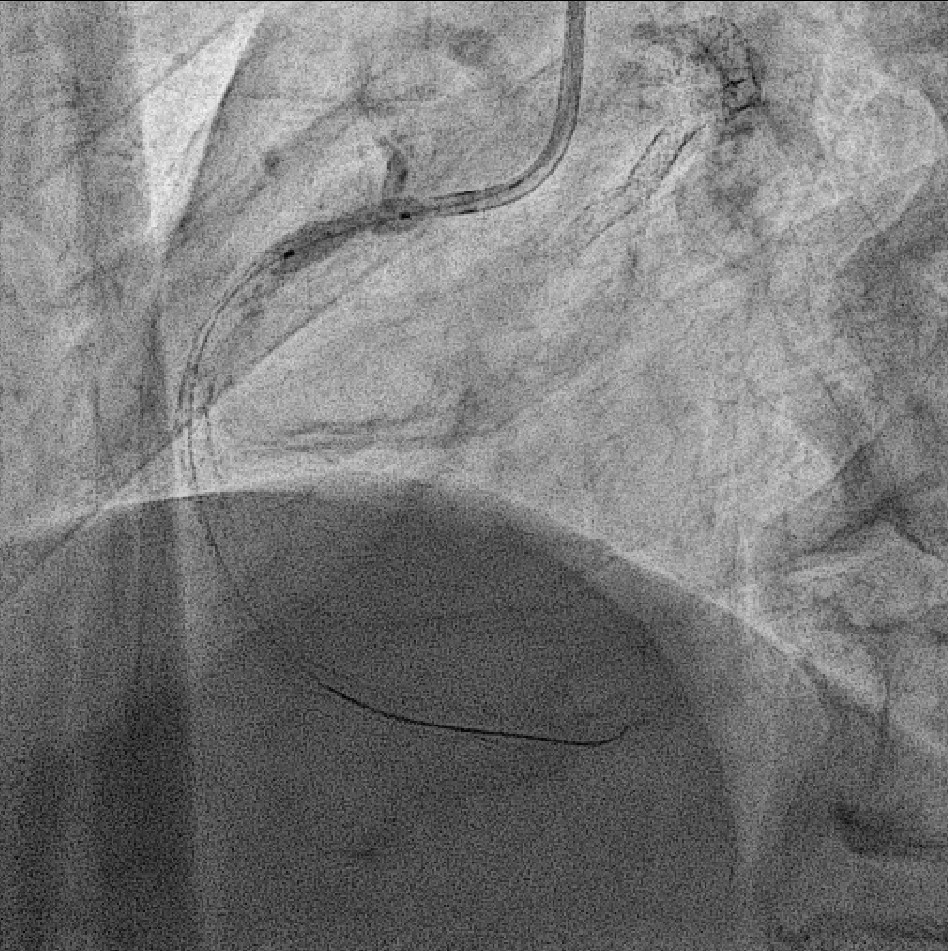
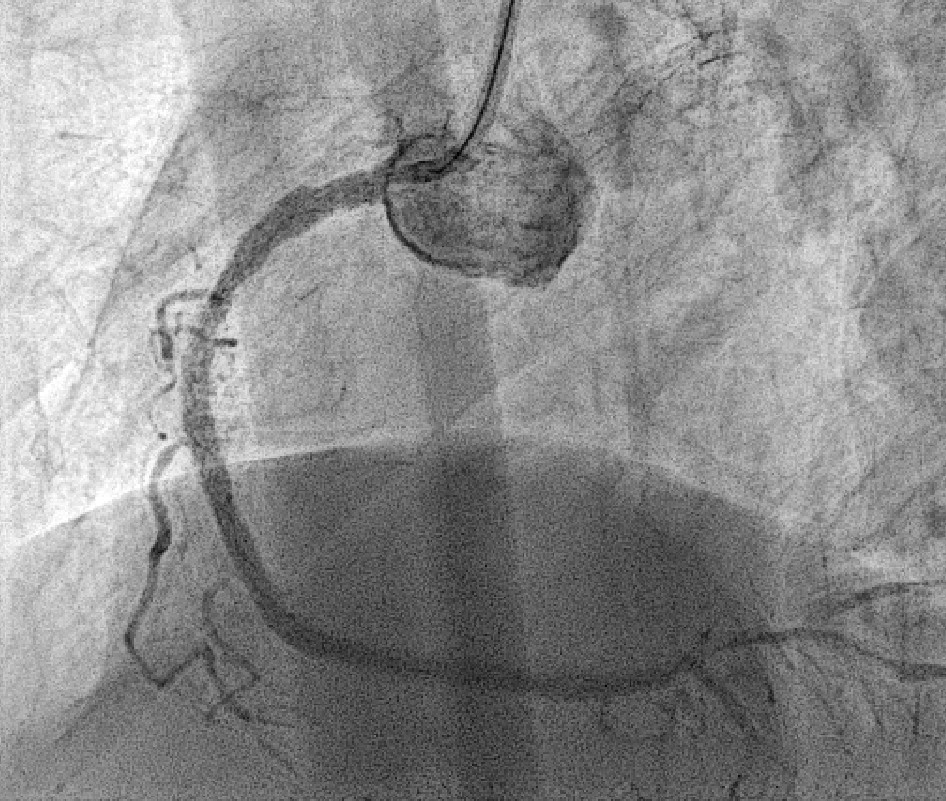
We advanced a 6F JR 4.0 SH 100cm guiding catheter and crossed the RCA ostial lesion using a Fielder FC guidewire. Pre-dilatation was performed with Ryurei 1.5×15mm balloon. IVUS was then performed, revealing a patent stent in the proximal to mid RCA. However, the ostial RCA stent was under-expanded, with smooth muscle compressing the stent from outside. Balloon pre-dilatation was carried out using an NC Euphora 4.0×12mm balloon, inflated up to 22 bar. However, the lesion was resistant and could not be fully dilated. We then applied a 4.0mm intravascular lithotripsy balloon with a total of 100 shocks delivered. But the effect was still minimal. The IVUS showed limited additional plaque fracture or vessel expansion. We tried NC Sapphire II 4.5×8 mm balloon inflation to 18 bar, but it was ineffective due to balloon slippage. The angiogram after oversized NC dilation showed residual stenosis of 59%. We then selected a Wolverine Cutting Balloon 4.0×10 mm and initiated dilation to 6 bar, which resulted in easy slippage again. Subsequent oversized dilations were performed at 18 bar, after which the lesion was successfully dilated. Using a Runthrough Floppy guidewire with the floating wire technique, a drug-eluting stent Biofreedom Ultra 4.0×14 mm was deployed in the ostial RCA ISR. We inflated at 14 bar for 14 seconds, repeated twice. Final post-dilatation was performed with an Accuforce 4.0×15mm balloon. The final IVUS showed good stent placement and expansion. We closed the procedure.
 PRE.AVI
PRE.AVI
POST.AVI
Case Summary
Mechanical causes of in-stent restenosis include stent underexpansion, fracture, deformation, and, less commonly, external compression from calcified nodules or smooth muscle hypertrophy. Previous studies have recommended high-pressure balloon angioplasty, cutting balloons, or repeat drug-eluting stent implantation for focal ISR, while reserving intravascular lithotripsy for complex or recurrent lesions. In our case, initial high-pressure balloon angioplasty and intravascular lithotripsy produced limited vessel expansion, but subsequent cutting balloon angioplasty achieved satisfactory results, likely due to its mechanical advantage or the sequential synergy of these modalities.