Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_046
A Hole in the Heart’s Highway: LAD-LV Fistula After Repeat PCI and the Road to Recovery
By Taufik Hidayat, Hyung-Bok Park
Presenter
Taufik Hidayat
Authors
Taufik Hidayat1, Hyung-Bok Park1
Affiliation
International St. Mary's Hospital, Korea (Republic of)1
View Study Report
CASE20251106_046
Coronary - Surgical Therapy (Coronary)
A Hole in the Heart’s Highway: LAD-LV Fistula After Repeat PCI and the Road to Recovery
Taufik Hidayat1, Hyung-Bok Park1
International St. Mary's Hospital, Korea (Republic of)1
Clinical Information
Relevant Clinical History and Physical Exam
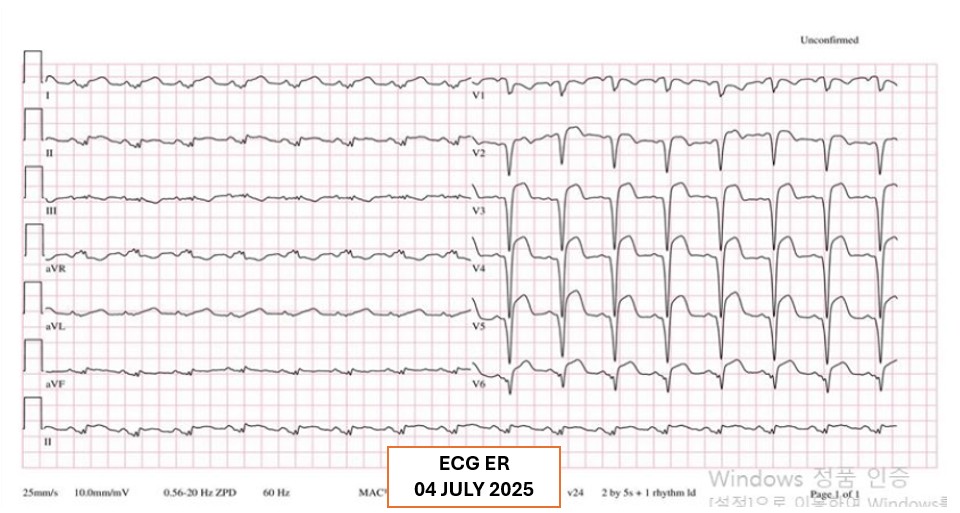
A 67-year-old woman arrived at the emergency department with chest pain. Just a month earlier, she had suffered an acute heart attack, an anterior STEMI, and underwent successful PPCI with a drug-eluting stent in the proximal LAD. Now, the familiar pain had returned. Initial evaluation in the ER revealed signs pointing to recurrent episode of acute coronary syndrome, raising concern that her heart was once again in danger.
 04072025(4).avi
04072025(4).avi
04072025(41).avi
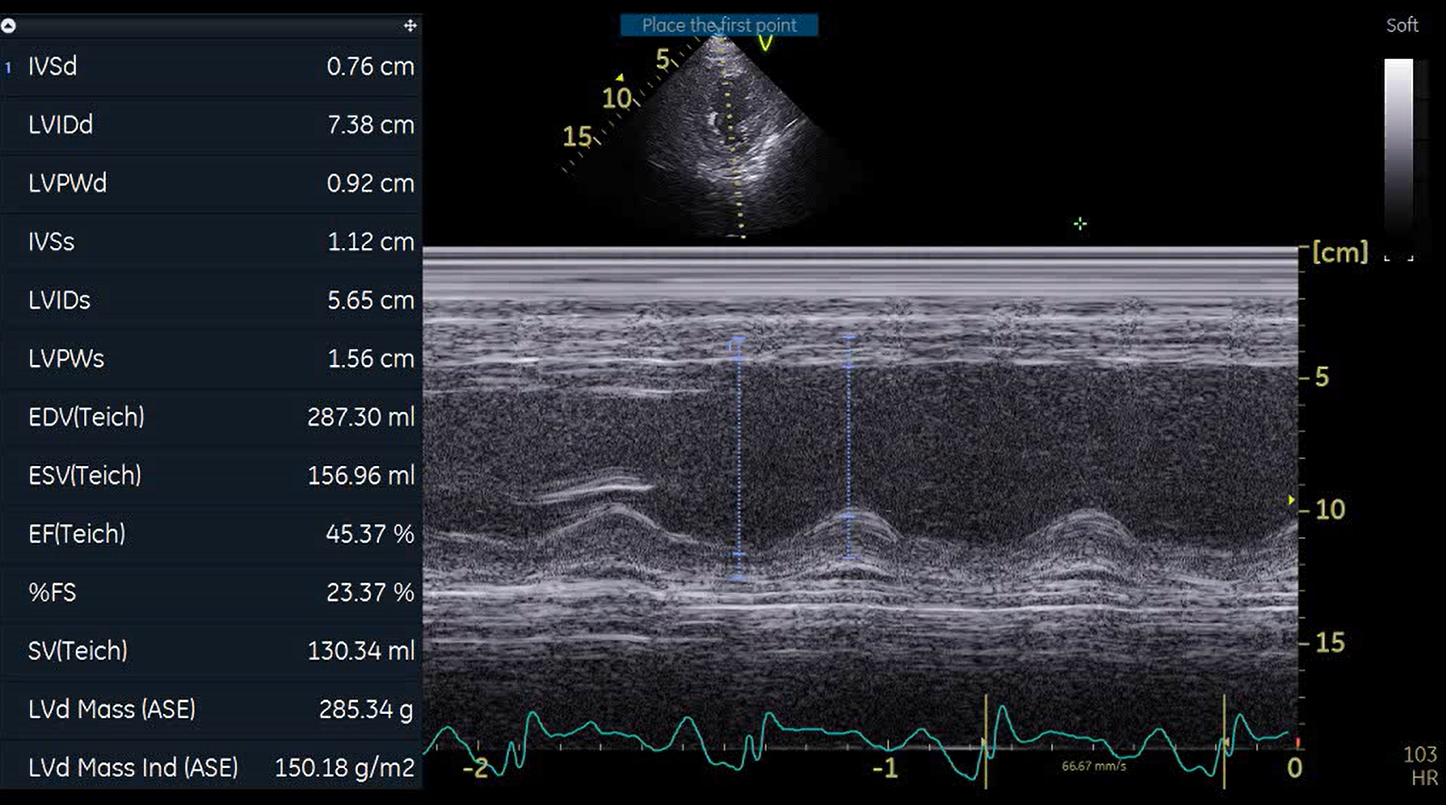
Relevant Test Results Prior to Catheterization
Several investigations were performed to prepare the 67-year-old patient for repeat coronary angiography, with plan for DCB or PCI if required. The team carefully reviewed her clinical stability, cardiac enzymes and imaging results to decide the safest path forward. Each step reflected both urgency and hope to restore her coronary flow and prevent another critical cardiac event from threatening her recovery.

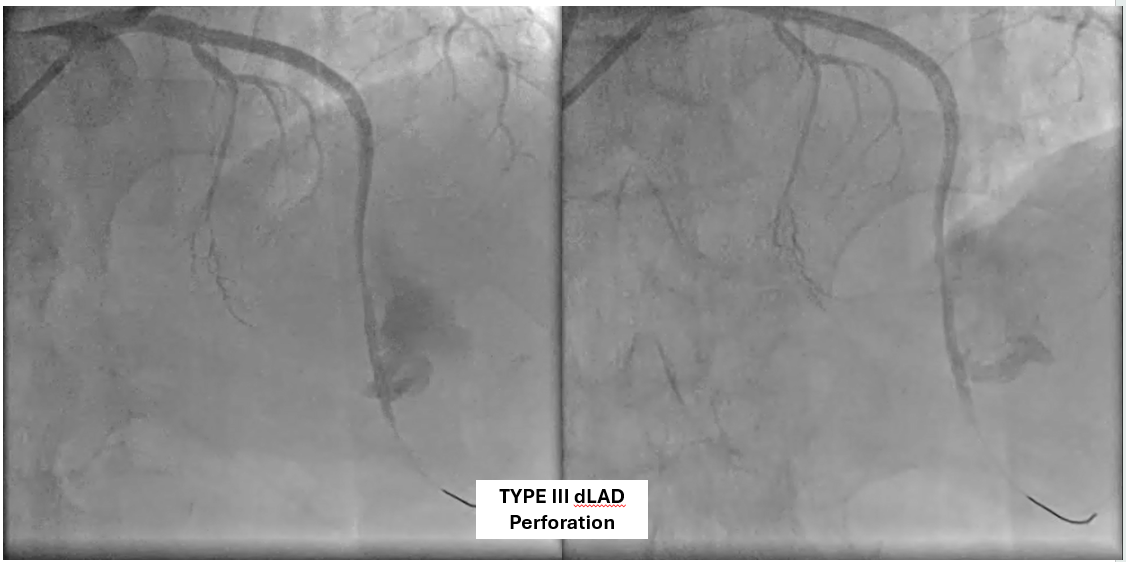
Relevant Catheterization Findings
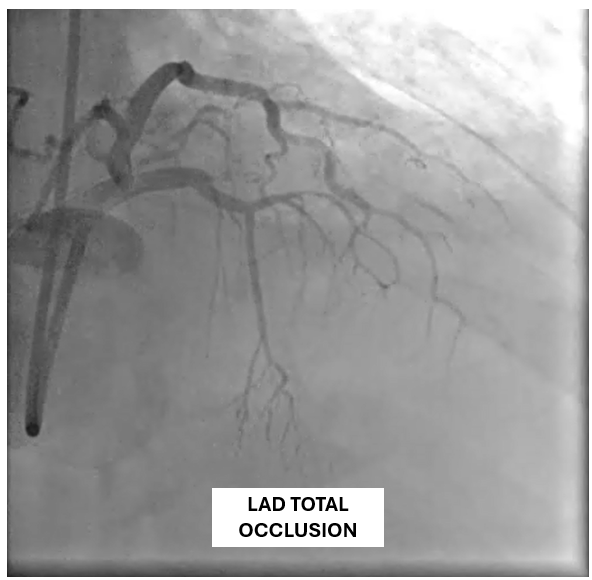
The patient underwent coronary angiography, where the team attempted to reopen the previously stented proximal mid LAD that had become occluded. After multiple revascularization efforts from ballooning to placing a ne DES in the mid LAD. A type III perforation occurred in the distal LAD during balloon inflation. Despite immediate measures including balloon tamponade and covered stent deployment, the perforation remained visible on follow-up angiography.
31072025(104).avi
31072025(126).avi
MRI.mp4
Interventional Management
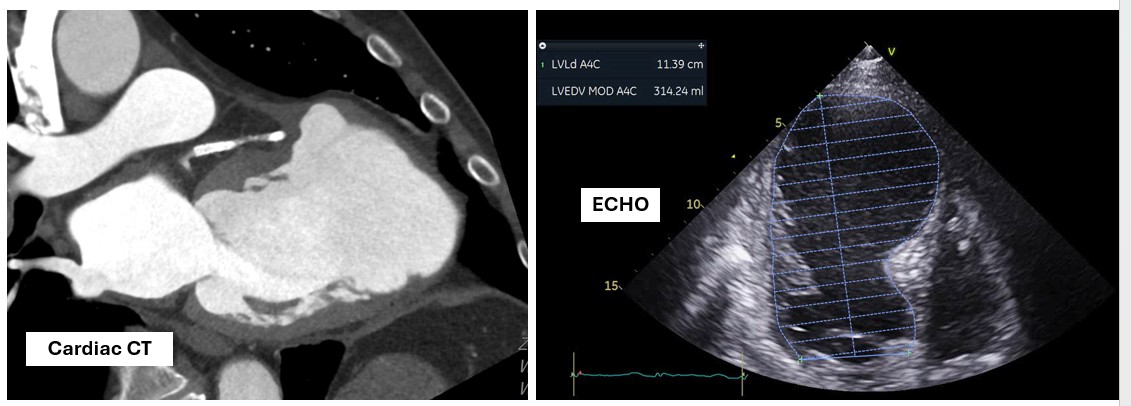
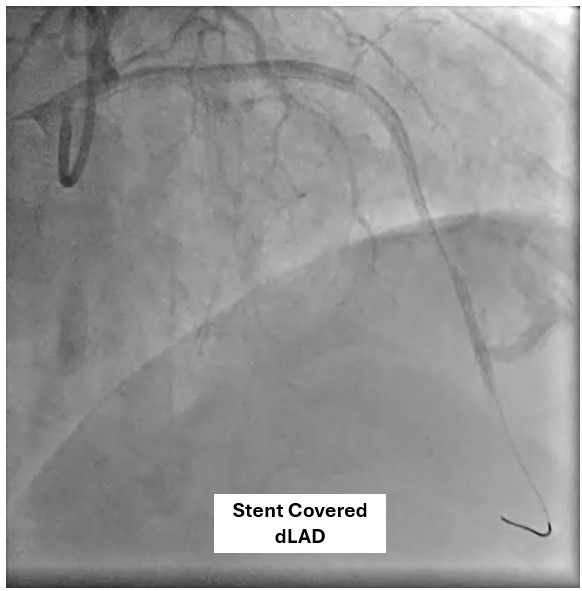
Procedural Step
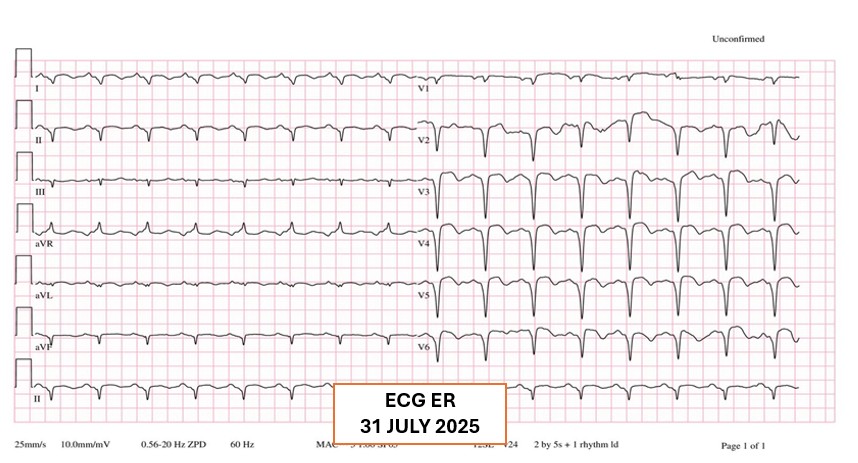
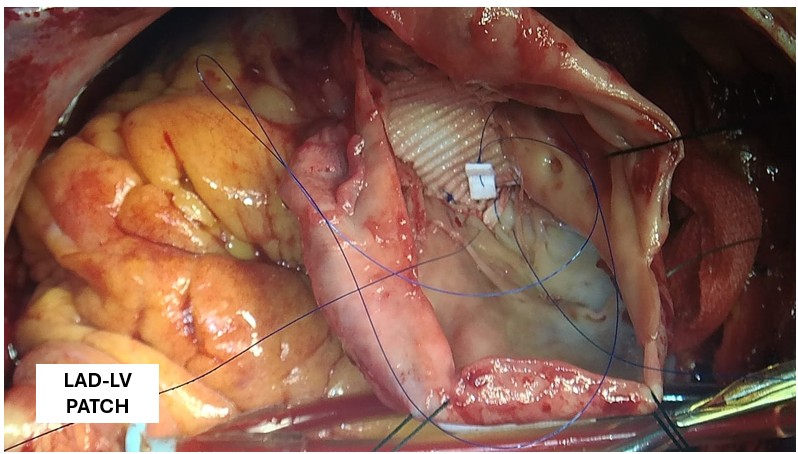
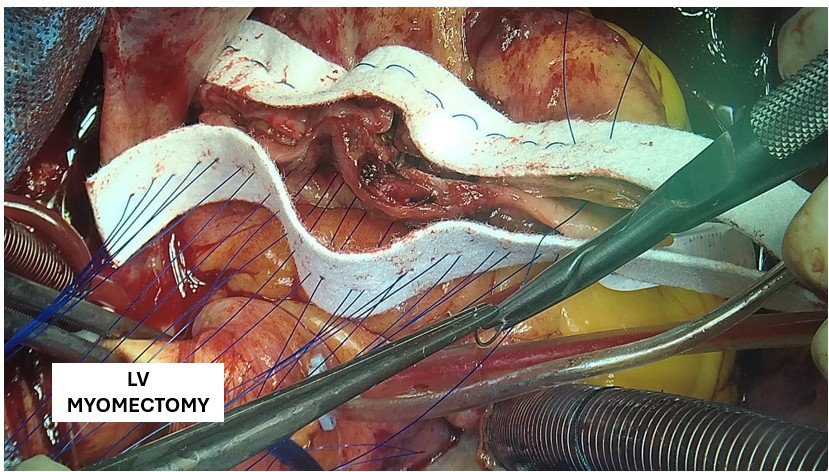
A covered stent was deployed in the distal LAD in an attempt to seal the coronary perforation; however, angiography showed that the Type III perforation persisted despite the intervention. Additional balloon inflation within the stent was performed, but the leakage could not be completely sealed. The patient remained hemodynamically stable without signs of cardiac tamponade or pericardial effusion. The following day, repeat coronary angiography was conducted to reassess the condition, which confirmed persistent contrast extravasation from the LAD into the left ventricular cavity, indicating the formation of a coronary–ventricular fistula. Given the hemodynamic significance and the risk of progressive left ventricular dysfunction due to continuous shunting, a multidisciplinary decision was made to proceed with surgical correction. The patient subsequently underwent successful LAD–LV fistula patch repair combined with. Surgical repair remains the definitive management for such cases, and early recognition with timely intervention is crucial to restore cardiac function and prevent irreversible myocardial damage.
Stent Covered.avi
Case Summary
The patient underwent successful surgical patch closure of the LAD–LV fistula along with ventricular reconstruction to restore myocardial integrity. The postoperative recovery was smooth and uneventful, with stable hemodynamics throughout hospitalization. Follow-up echocardiography demonstrated significant improvement in LVEF to 53%, and she remained asymptomatic during subsequent outpatient follow-up