Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_044
IVUS-Guided Drug-Coated Balloon Angioplasty: A Stent-Sparing Strategy for Severe Proximal Lad Stenosis Adjacent to the Left Main Stem
By Addi Bin Mokhtar, Wei Liang Lee, Afif Ashari
Presenter
Addi Bin Mokhtar
Authors
Addi Bin Mokhtar1, Wei Liang Lee1, Afif Ashari1
Affiliation
National Heart Institute Malaysia, Malaysia1
View Study Report
CASE20251106_044
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
IVUS-Guided Drug-Coated Balloon Angioplasty: A Stent-Sparing Strategy for Severe Proximal Lad Stenosis Adjacent to the Left Main Stem
Addi Bin Mokhtar1, Wei Liang Lee1, Afif Ashari1
National Heart Institute Malaysia, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 58-year-old man with underlying hypertension presented with chest discomfort during exertion and a positive stress test. Echocardiogram shows ejection fraction of 54% and no regional wall motion abnormalities. He underwent a coronary angiogram which showed severe stenosis of the proximal LAD and moderate disease of Left main stem. We proceeded with PCI of the proximal LAD using a drug-coated balloon (DCB). The final angiography showed TIMI 3 flow.
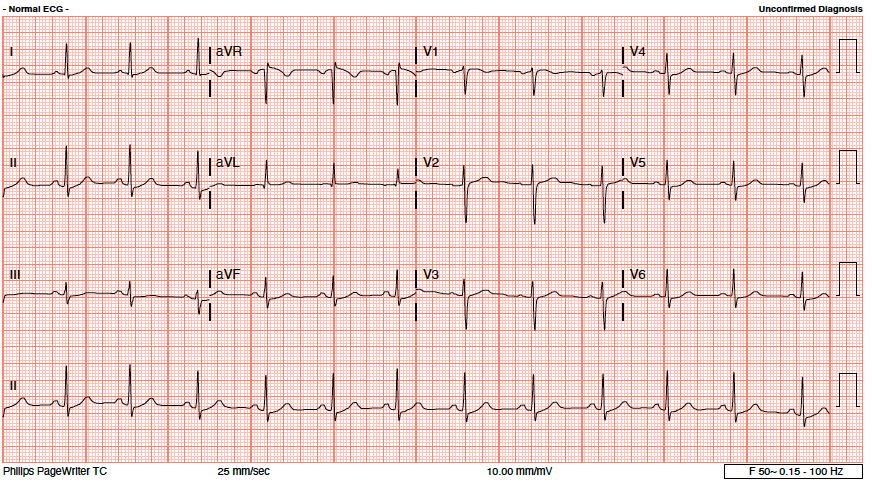
Relevant Test Results Prior to Catheterization
TG: 4.1 mmol/l (<2.3 mmol/l)HbA1c: 5.9% (<5.7%)
Relevant Catheterization Findings
Left Main: moderate distal stenosis 40%
LAD: severe stenosis proximal 95%, TIMI 3
LCx: Small, non-dominant, diffuse disease
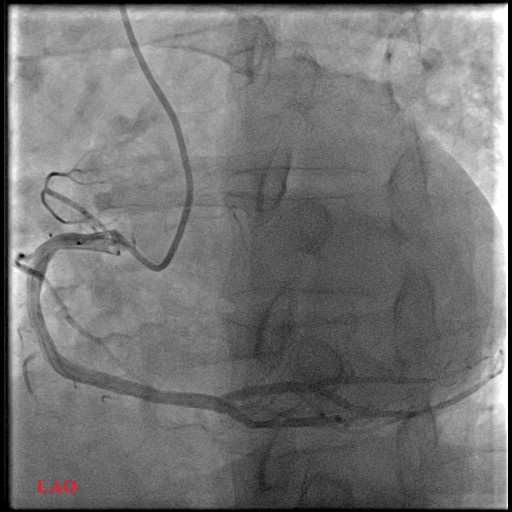
RCA: mild proximal disease 20%
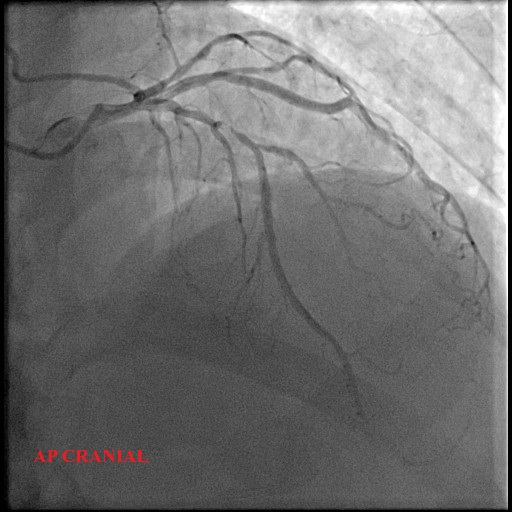
 ap cranial.avi
ap cranial.avi
ap caudal.avi
LAO RCA.avi
LAD: severe stenosis proximal 95%, TIMI 3
LCx: Small, non-dominant, diffuse disease
RCA: mild proximal disease 20%
Interventional Management
Procedural Step
The left coronary sinus was engaged with an EBU 3.5 /6F catheter.
A RUNTHROUGH Floppy wire was advanced across the lesion in LAD. A SION BLUE wire was placed into the Diagonal branch for protection.
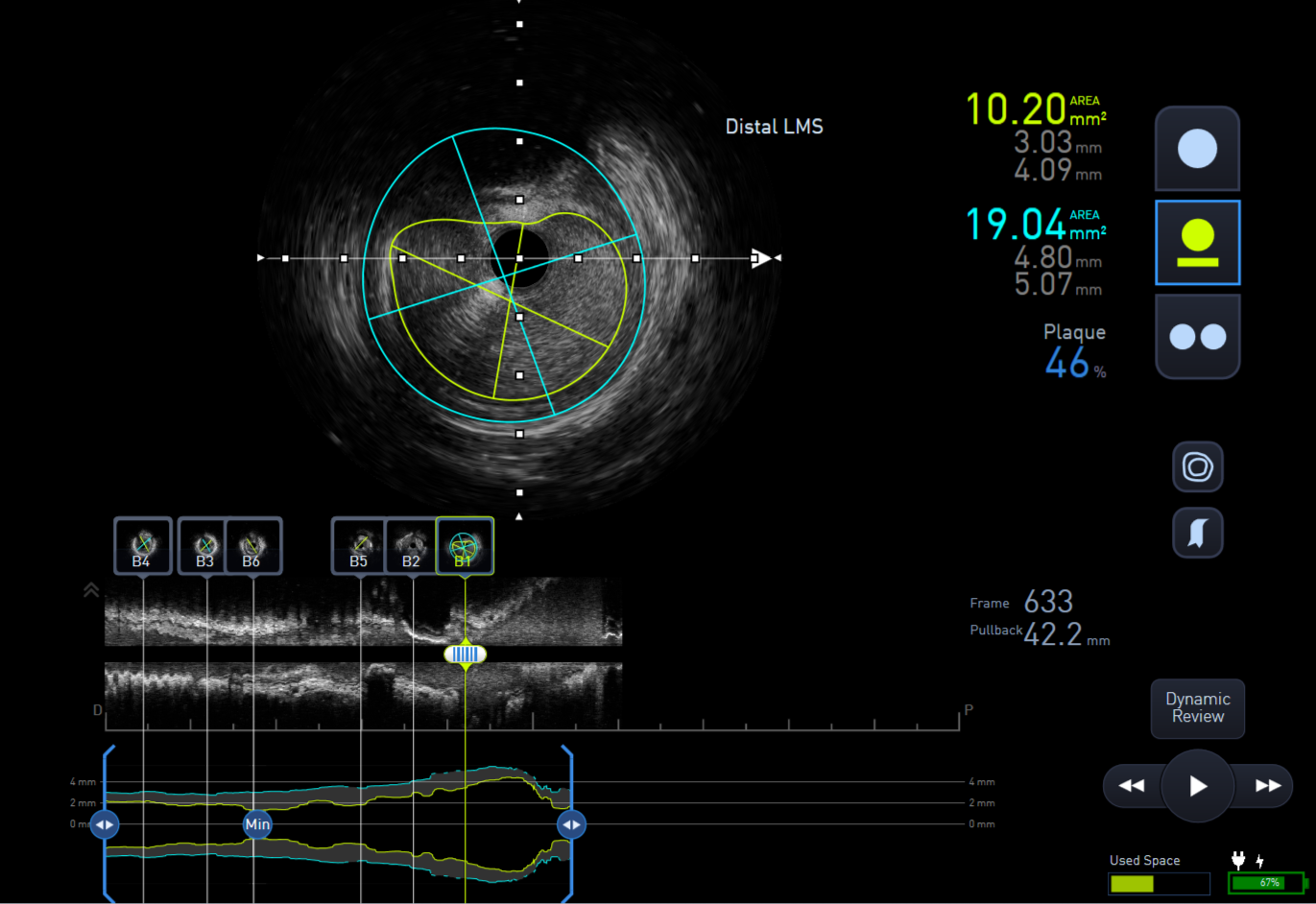
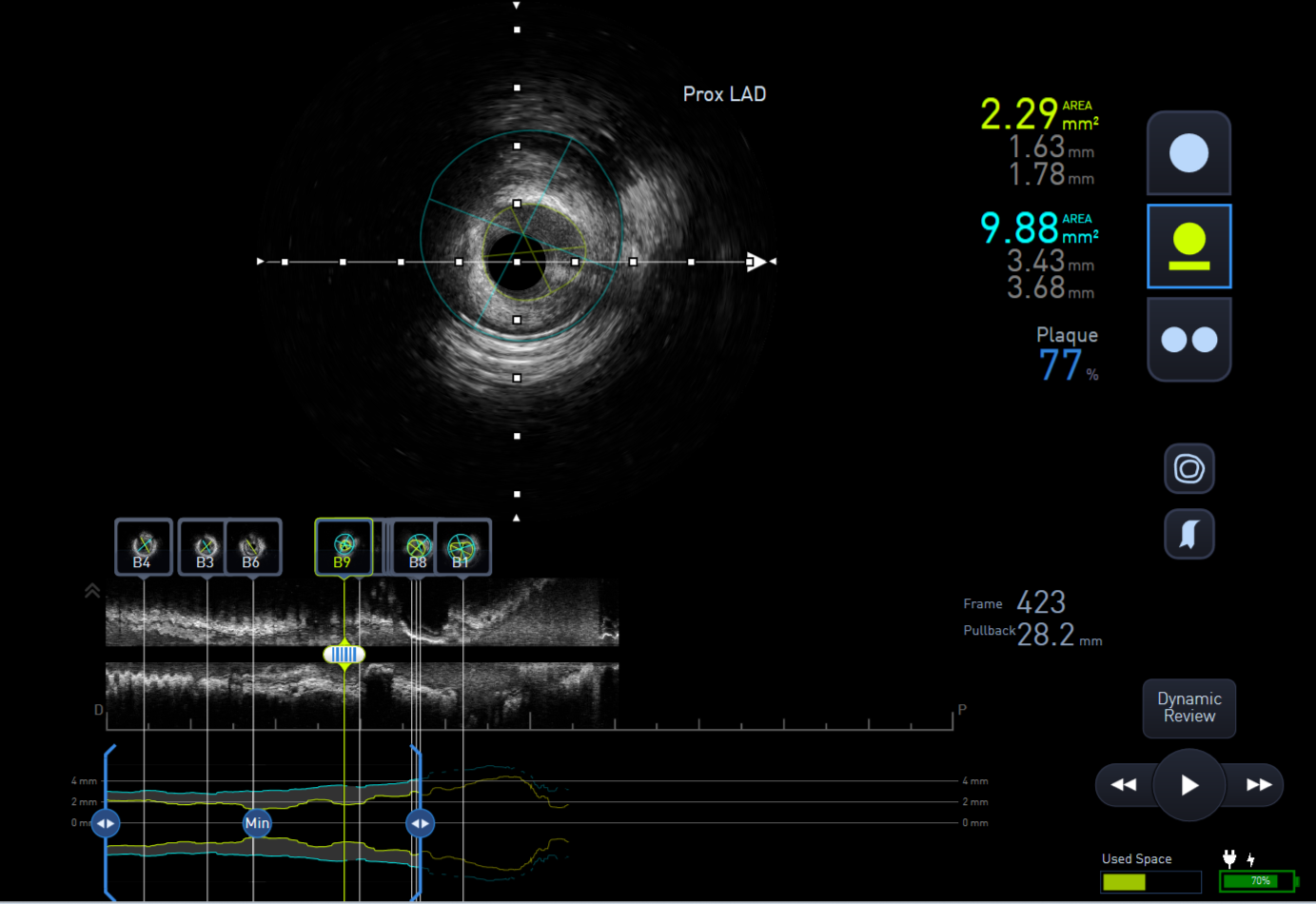
The lesion was predilated with a 2.0x15mm semi-compliant balloon to facilitate IVUS passing through the lesion. IVUS assessment showed distal Left main stem minimal lumen area (MLA) of 10mm2, proximal LAD 3.5mm2 and mid LAD 2.75mm2.
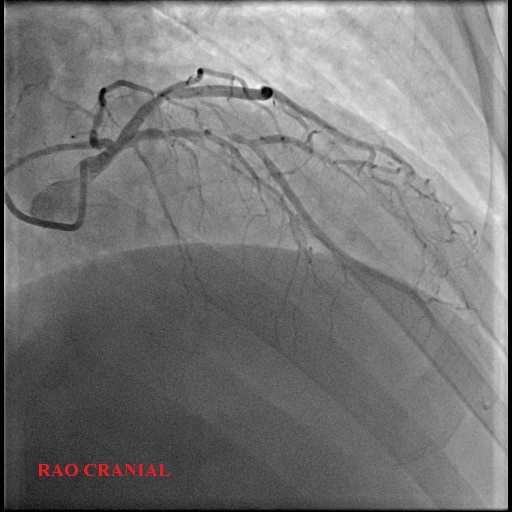
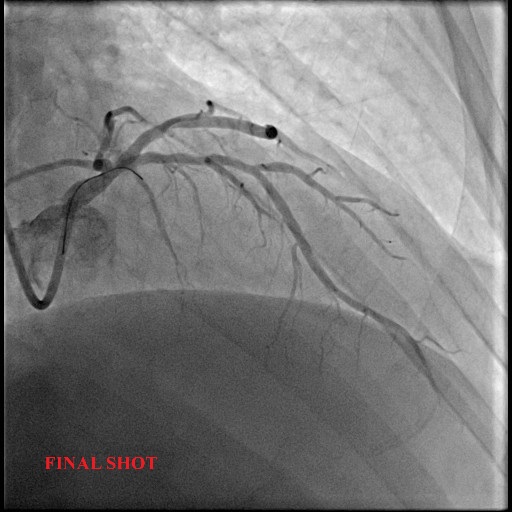
The lesion was predilated again with a 2.5x15mm and subsequently was treated with a drug-coated balloon 2.75x30mm. Final result showed good luminal gain and TIMI 3 flow.
post dilate balloon.avi
Run 1 - Pre LAD.mp4
final shot RAO cranial.avi
A RUNTHROUGH Floppy wire was advanced across the lesion in LAD. A SION BLUE wire was placed into the Diagonal branch for protection.
The lesion was predilated with a 2.0x15mm semi-compliant balloon to facilitate IVUS passing through the lesion. IVUS assessment showed distal Left main stem minimal lumen area (MLA) of 10mm2, proximal LAD 3.5mm2 and mid LAD 2.75mm2.
The lesion was predilated again with a 2.5x15mm and subsequently was treated with a drug-coated balloon 2.75x30mm. Final result showed good luminal gain and TIMI 3 flow.
Case Summary
This case demonstrates that DCB angioplasty for severe de novo proximal LAD stenosis near a moderate LMS lesion is a viable and successful strategy when combined with rigorous lesion preparation and IVUS guidance to confirm an acceptable LMS minimal lumen area and optimal LAD result. The successful outcome without the need for a stent in the proximal LAD mitigates the potential for stent-related complications and compromising the Left Main or LCx from a cross-over stenting technique. This approach aligns with the "leave nothing behind" philosophy and should be considered for patients with proximal coronary lesions adjacent to the LMS.