Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_043
A Complication That Became the Key to Completion
By Jayanta Saha, Arindam Mitra
Presenter
Arindam Mitra
Authors
Jayanta Saha1, Arindam Mitra1
Affiliation
Medical College, Kolkata, India1
View Study Report
CASE20251106_043
Coronary - Complex PCI - CTO
A Complication That Became the Key to Completion
Jayanta Saha1, Arindam Mitra1
Medical College, Kolkata, India1
Clinical Information
Relevant Clinical History and Physical Exam
65 years old male, Hypertensive, Non-Diabetic, Smoker with dyslipidemia presented with exertional chest pain for last 6 months (CCS II). Associated with shortness of breath. No history of palpitations, pre-syncope, syncope. He underwent coronary angiography elsewhere and a failed attempt at PTCA.
Relevant Test Results Prior to Catheterization
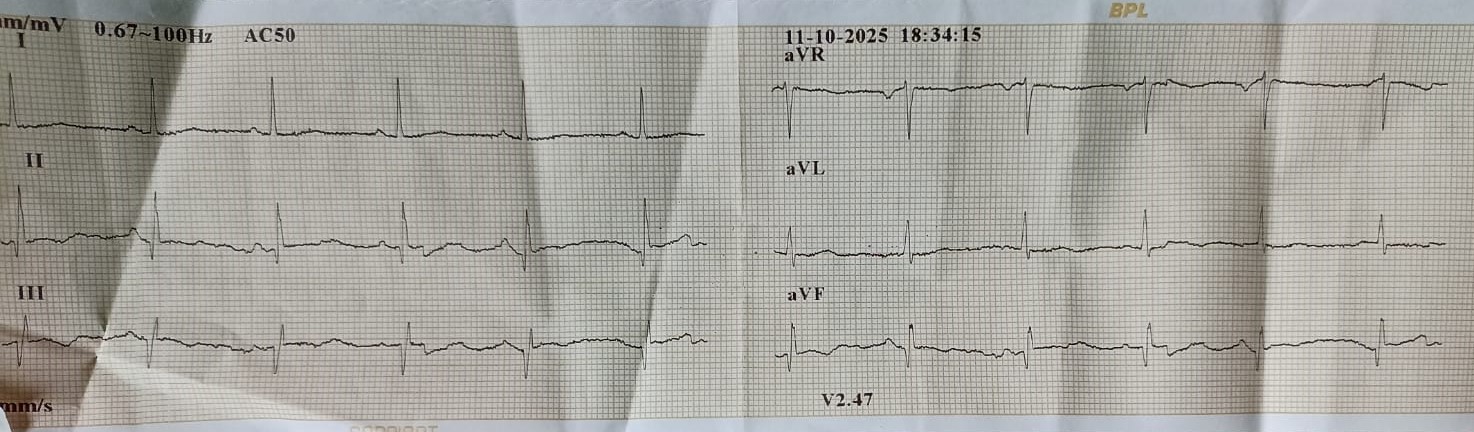
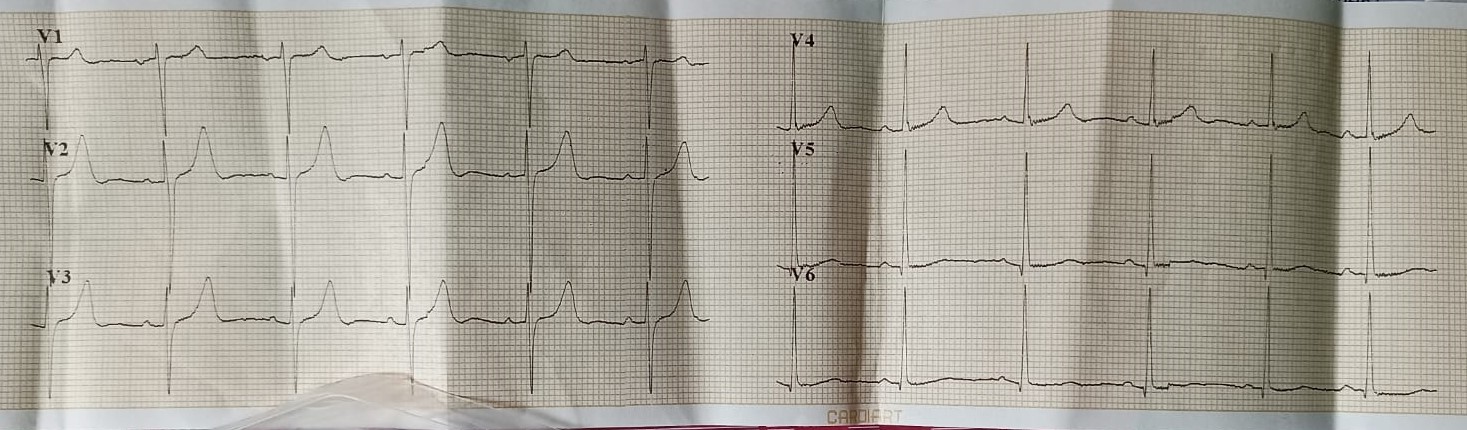
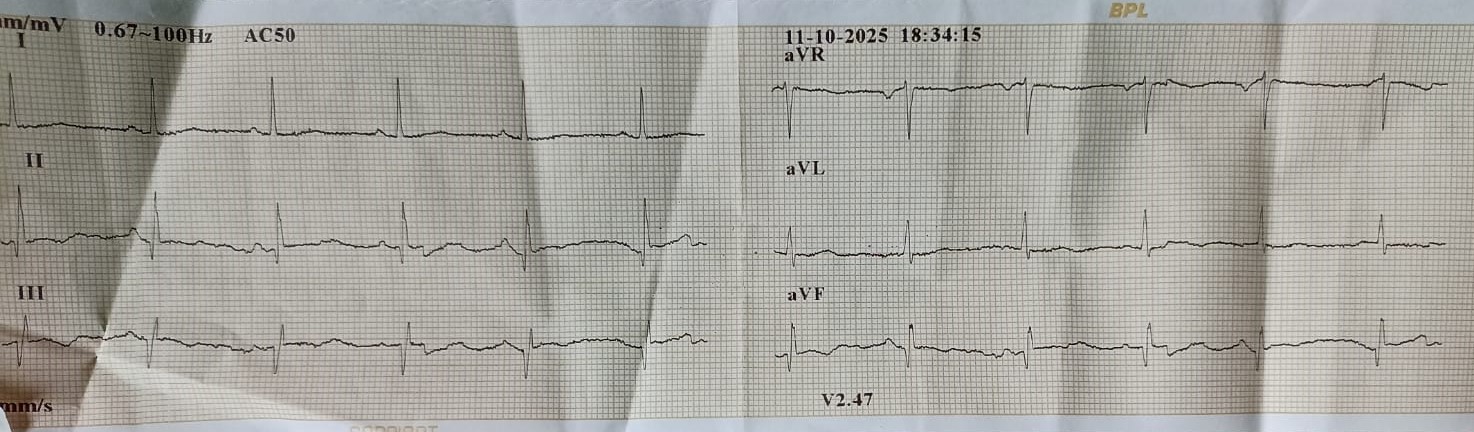
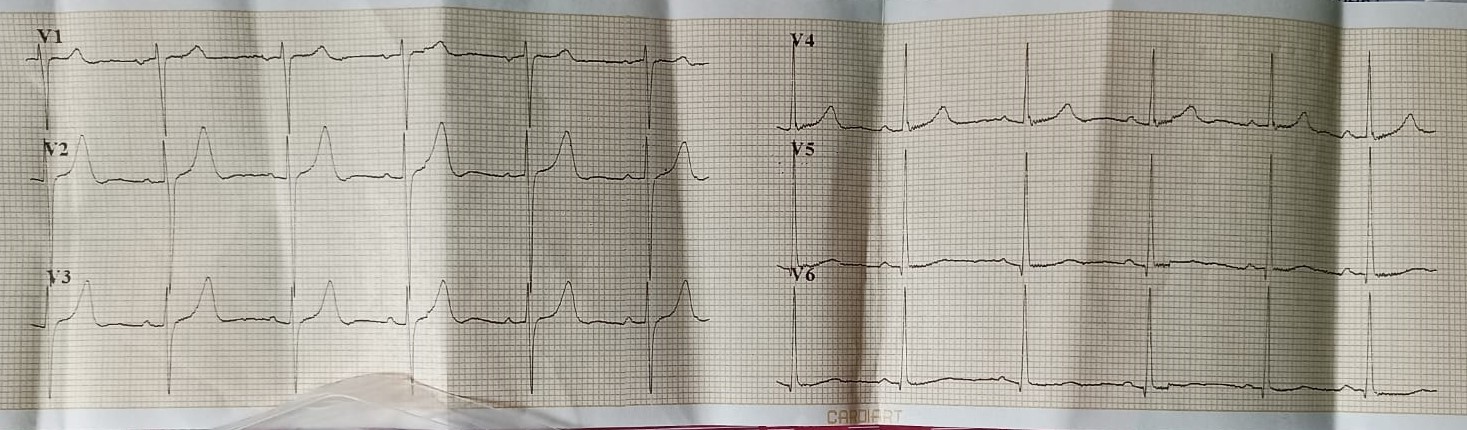
Hemoglobin: 14.6 gm/dLFasting Blood Glucose: 98 mg/dLS. Creatinine: 1.2 mg/dLLDL-C: 121 mg/dLECG: sinus rhythm, Q in lead III, aVF, LVH2D Echo: Inferobasal wall hypokinesia, LVEF 48%
Relevant Catheterization Findings
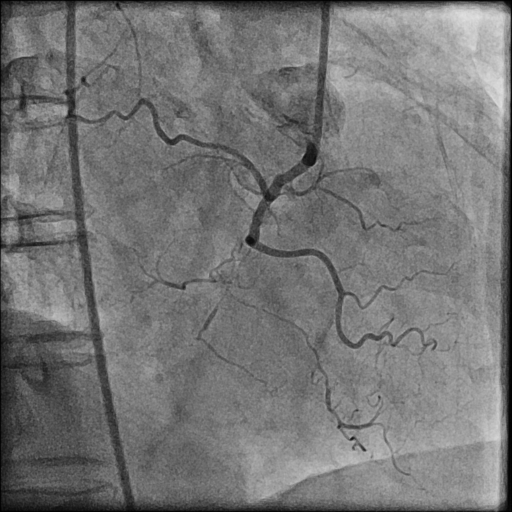
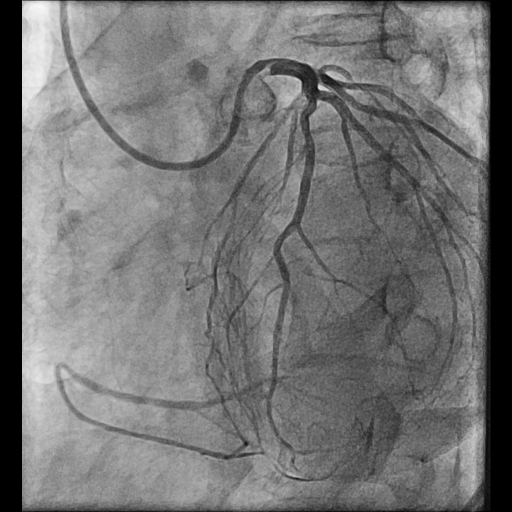
Coronary Angiogram done elsewhere via right femoral artery with JR and AL 1.0LMCA NormalLAD Type III Vessel. Normal. LCx: Non dominant, NormalRCA: Chronic Total Occlusion from midpart. Distal filling by retrograde from Left system.J-CTO score 3

 CAG Video 1.mp4
CAG Video 1.mp4
CAG Video 2.mp4
CAG Video 3.mp4
Interventional Management
Procedural Step
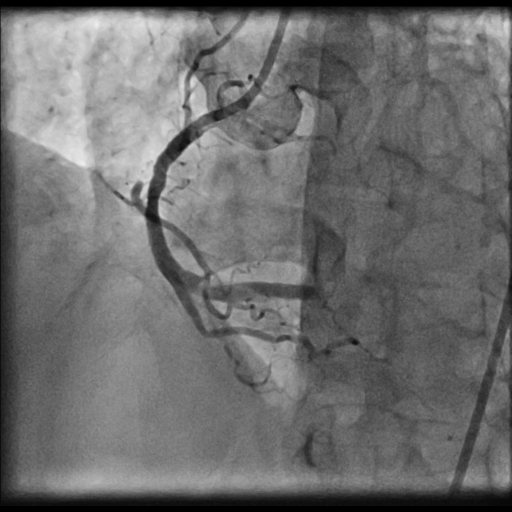
LMCA was engaged with JL 4.0 7 Fr. catheter. First septal collateral was used to reach the distal cap of the lesion using Sion black, Runthrough extrafloppy and Fielder XT-R wire with microcatheter but could not penetrate the distal cap. The lesion could not be crossed with Gaia second and Gladius® Mongo® wire. Antegrade approach was decided to a cross the lesion with Gaia second wire. Antegrade approach caused a dissection resulting in a sub intimal hematoma which extended into the Posterolateral branch. This dissection and the hematoma straightened the vessel near the distal cap. Now this straightening allowed the ASAHI Gladius® Mongo® wire to cross the distal cap retrogradely. The Gladius® Mongo® wire could not be positioned into the true lumen. Now to avoid further dissection proximally the Mongo wire was exchanged with Pilot 150 wire. This wire could cross the proximal cap and finally into the guide catheter. Pilot 150 wire was exchanged with Choice Floppy LS 300 cm which was externalized. A finecross microcatheter was advanced over this wire antegradely. Retrograde microcatheter removed and rest of the case was completed via antegrade approach over Runthrough NS Floppy wire. Lesion was predilated with 2.5x12 mm NC balloon @ 12 atm. Promus Elite 2.75x38 mm DES deployed in mid to distal RCA @ 12 atm. An overlapping stent Xience Xpedition 3.0x28 mm DES deployed from ostium to mid RCA @ 11 atm. Post dilatation with 3.25x10 mm NC balloon @ 11 atm. Distal TIMI III flow achieved.


PTCA 1.mp4
PTCA 2.mp4
PTCA 3.mp4
Case Summary
Retrograde CTO is a technically challenging procedure which requires meticulous planning and hardware support. Sometimes complications may facilitate the procedure as in our case the dissection caused while attempting to cross the lesion antegradely allowed retrograde crossing by altering the shape of the vessel. So complications, though not desirable may help in the completion of the procedure.