Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_042
Recanalization of Right Coronary Artery CTO Using Reverse Cart and Anchoring Balloon Technique
By Wei Hsu, Wei-Chieh Lee
Presenter
Wei Hsu
Authors
Wei Hsu1, Wei-Chieh Lee1
Affiliation
Chi Mei Medical Center, Taiwan1
View Study Report
CASE20251106_042
Coronary - Complex PCI - CTO
Recanalization of Right Coronary Artery CTO Using Reverse Cart and Anchoring Balloon Technique
Wei Hsu1, Wei-Chieh Lee1
Chi Mei Medical Center, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
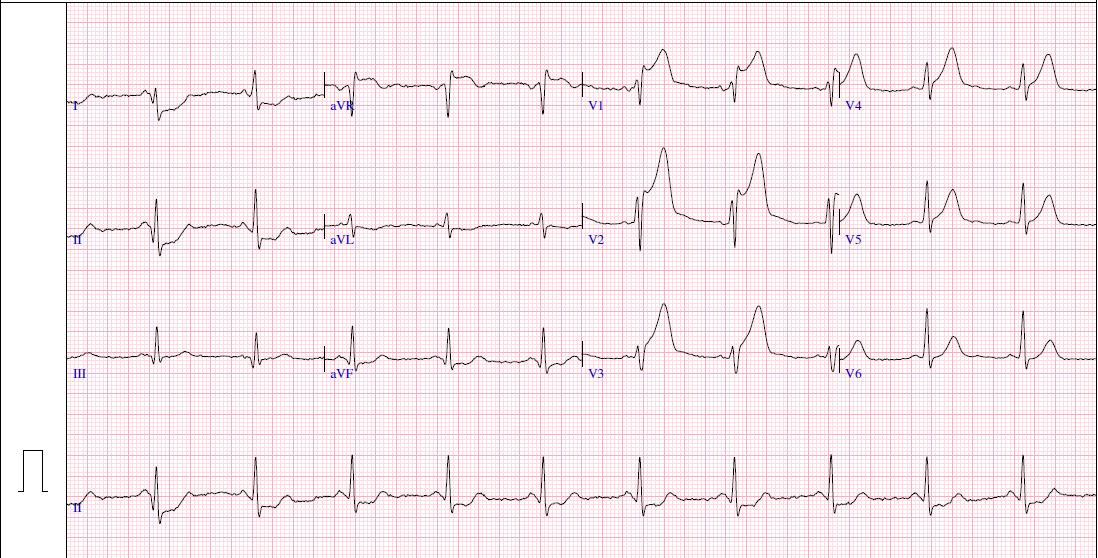
A 36-year-old man with dyslipidemia and schizophrenia, and a 10-year history of smoking (1 pack/day), presented with intermittent chest pain for several days. He initially visited the cardiology outpatient clinic for evaluation. Before his scheduled follow-up, he developed acute chest pain with ECG showing ST-elevation myocardial infarction (STEMI) and was referred to the emergency department for primary PCI.
Relevant Test Results Prior to Catheterization
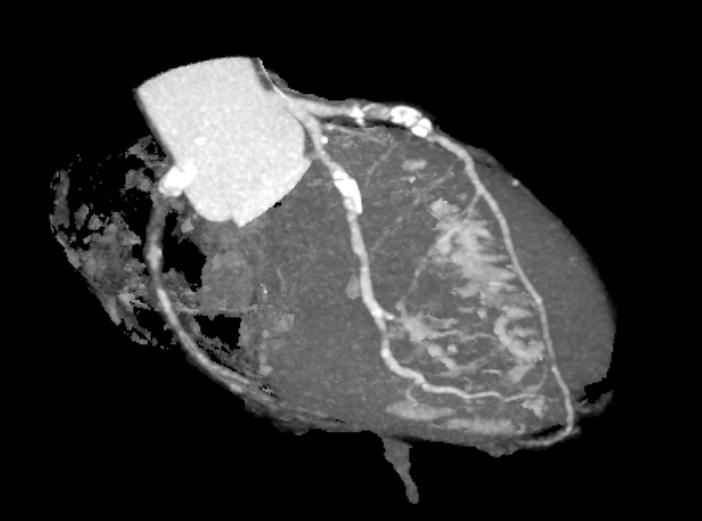
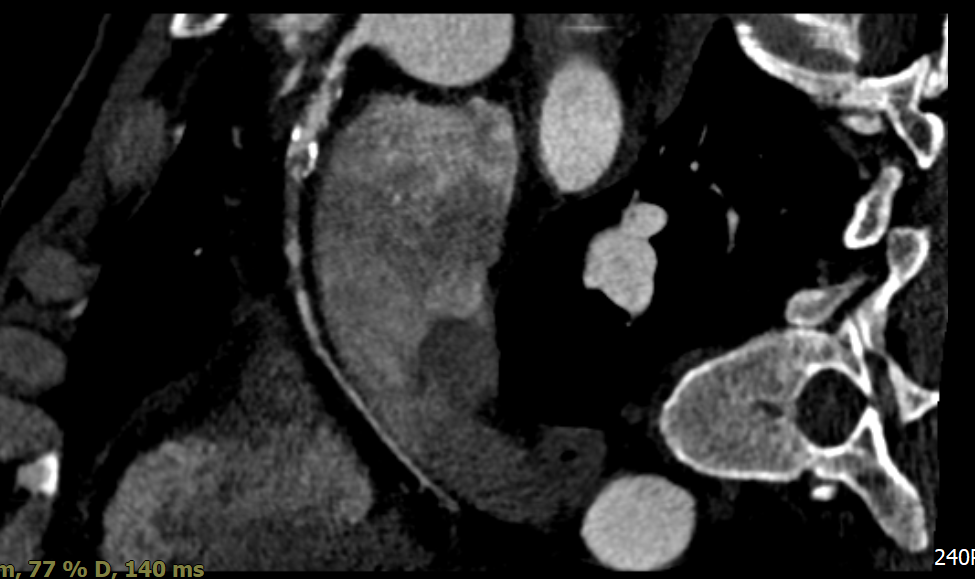
Coronary computed tomography angiography revealed a high calcium score of 1204.3 with focal occlusion and stenosis at the proximal LAD and proximal to mid RCA segments. Transthoracic echocardiography demonstrated preserved left ventricular systolic function (LVEF 61%) with mild hypokinesis of the basal anteroseptal wall.
Relevant Catheterization Findings
Coronary angiography revealed three-vessel disease (SYNTAX score 29) with total occlusion of the proximal to mid LAD, 50% stenosis at the proximal LCX, and 70% stenosis at the distal LCX. The RCA showed chronic total occlusion from the proximal segment with collateral filling from both the LCX and LAD. The findings were consistent with acute anterior STEMI.
Interventional Management
Procedural Step
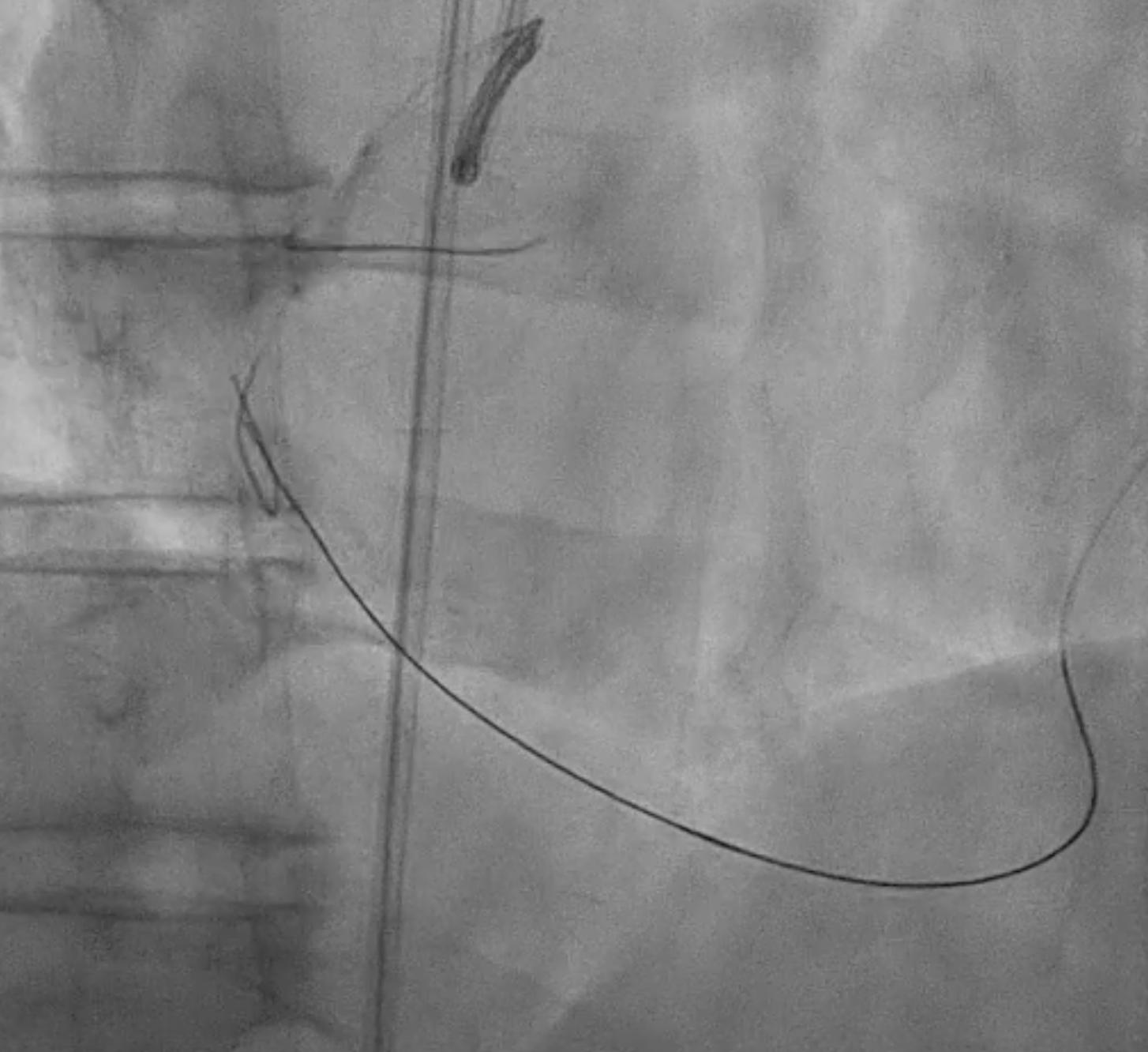
Because the patient presented with acute coronary syndrome, primary PCI was first performed for the culprit lesion, and a drug-eluting stent (DES) was implanted in the proximal LAD. A staged PCI with DES implantation to the proximal LCX was later performed. The initial antegrade attempt for RCA chronic total occlusion (CTO) failed despite wire escalations, as the guidewires could not cross the lesion. Considering the patient’s intolerance and high contrast volume, the procedure was terminated. One month later, the patient was readmitted for complete revascularization. Antegrade wiring with a microcatheter and multiple guidewires (Fielder FC, ULTIMATEbros3, Conquest Pro) again failed to cross the RCA CTO. A retrograde approach using a SION wire via a septal collateral successfully reached the distal RCA. As the retrograde wire could not smoothly re-enter the true lumen, an antegrade wire was used to create a controlled subintimal hematoma, followed by the reverse CART technique. Anchoring balloon support then facilitated microcatheter advancement into the proximal RCA. The rendezvous technique achieved externalization with an ASAHI RG3 330 cm wire, and two Runthrough wires were advanced antegradely into the PDA and PL branches. After sequential balloon dilatation, two DESs (XIENCE Skypoint 2.75 × 48 mm and 3.5 × 38 mm) were deployed from the distal to the ostial RCA under IVUS guidance. Final angiography showed successful recanalization with TIMI 3 flow.

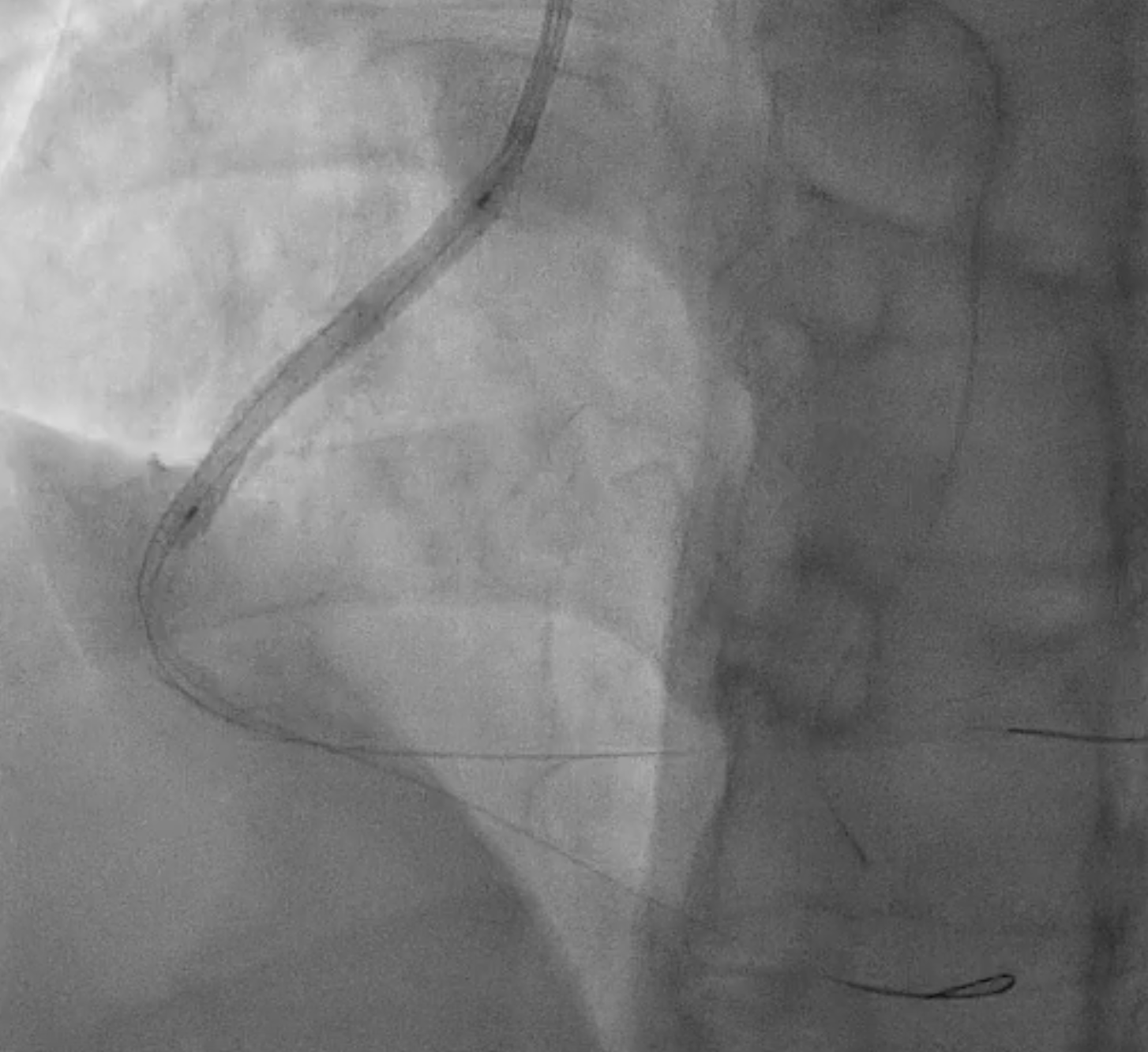
Case Summary
This case demonstrates the standard workflow of a retrograde CTO approach.