Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_041
Double Culprit Lesions in a Patient With ST-Segment Elevation Myocardial Infarction
By Rizka Audiva Iqbal, Muhammad Iqbal, David Almeidi
Presenter
Rizka Audiva Iqbal
Authors
Rizka Audiva Iqbal1, Muhammad Iqbal1, David Almeidi1
Affiliation
Pertamina Hospital Balikpapan, Indonesia1
View Study Report
CASE20251106_041
Coronary - ACS/AMI
Double Culprit Lesions in a Patient With ST-Segment Elevation Myocardial Infarction
Rizka Audiva Iqbal1, Muhammad Iqbal1, David Almeidi1
Pertamina Hospital Balikpapan, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
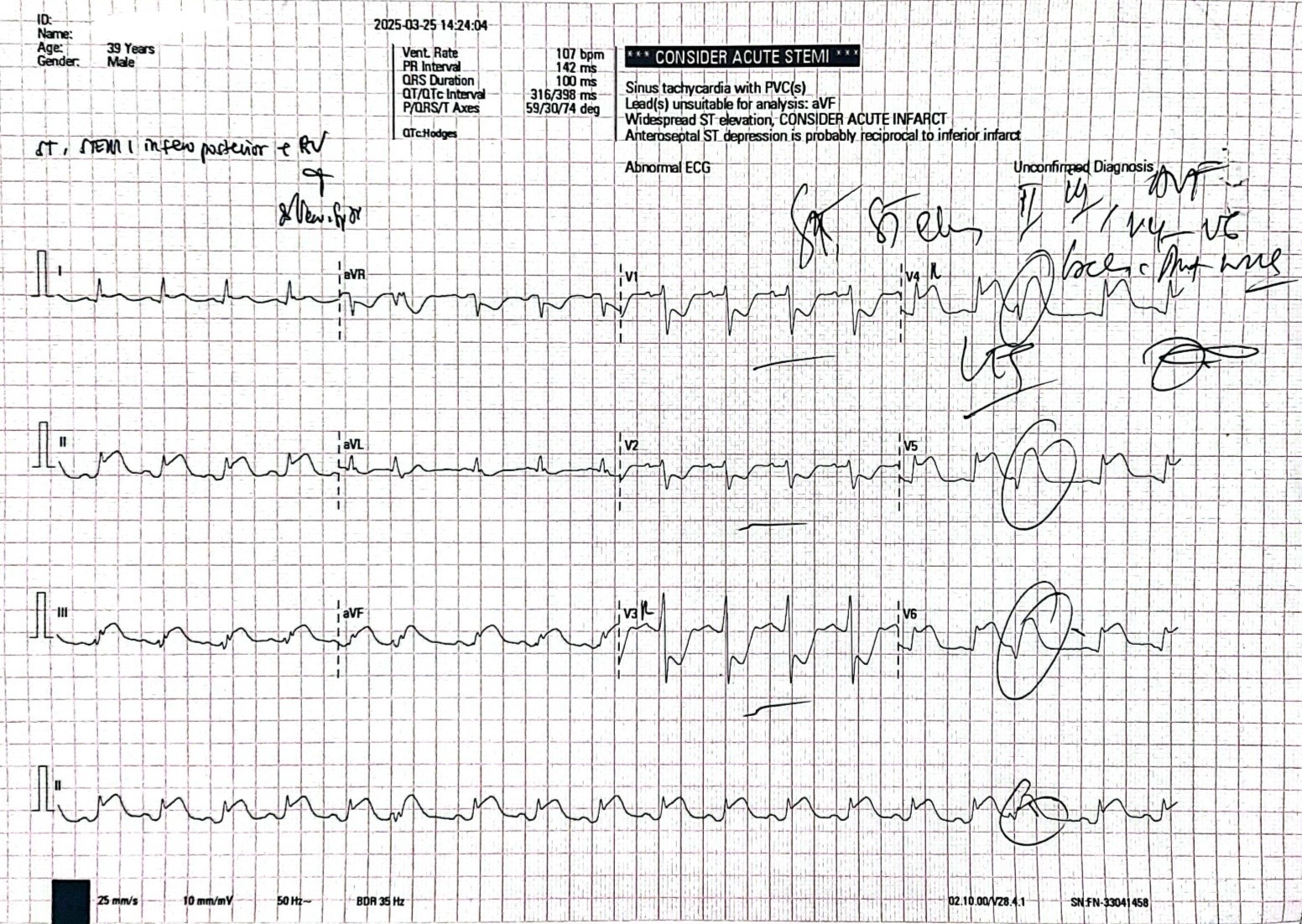
A 39YO male with risk factor of smoking was referred to our hospital with acute extensive infero-postero lateral and RV infarction. He experienced severe chest pain radiating to the back 2 hours before admission. A few weeks before, he had several episodes of angina. In the ER, his BP was 80 / 50 mmHg and HR was 110x / minute. His physical examination was within normal limit except for cool extremities. He developed ventricular fibrillation which was successfully defibrillated to sinus rhythm.
Relevant Test Results Prior to Catheterization
The laboratory findings showed increased level of Troponin T ( 0.037 ng/ml ). Electrocardiogram revealed ST elevation in lead II, III, AVF, V4R, V5 and V6, and deep ST depression in lead V1, V2 and V3R.
Relevant Catheterization Findings
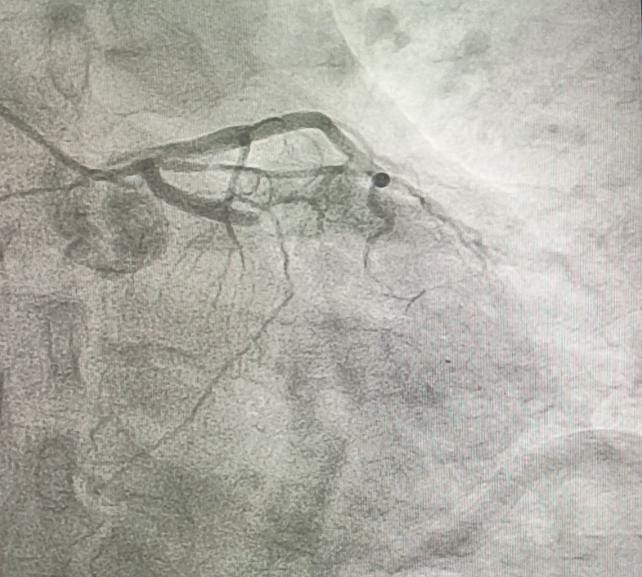
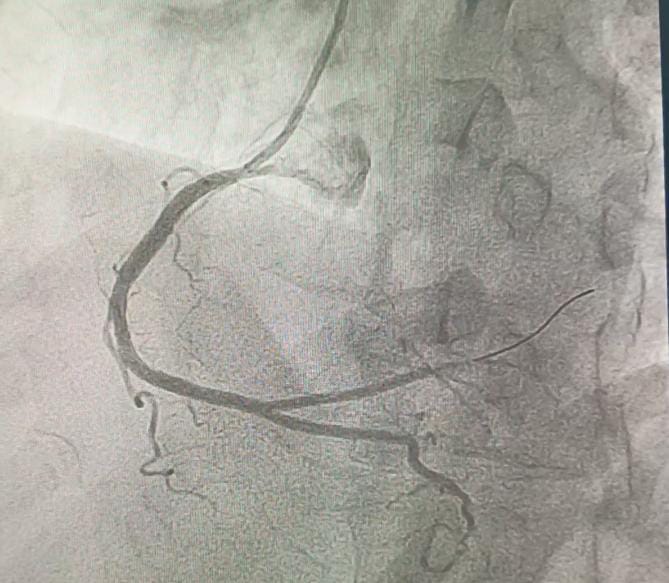
Coronary angiography revealed total occlusion of the proximal LCx and a sub totally occluded RCA with thrombus.

Interventional Management
Procedural Step
Both RCA and LCx were considered as the culprit lesion. We decided to addressed the lesion in RCA first, since the flow is still TIMI III. RCA was engaged with 6F JR guiding catheter. Run through wire was advanced distally to RCA. After pre dilatation with NC balloon 3.5 / 18 mm the thrombus disappeared. A 3.5 / 22 mm stent was implanted in RCA at 18 atm. Post dilatation with stent balloon at maximum pressure 20 atm. Final angiogram showed TIMI 3 flow. Then we intervene the LCx. We used BL guiding catheter to engage the LCx. Run through NS floppy wire was advanced to distal LCx. Coronary angiogram showed good contrast flow to distal LCx. Pre dilatation at proximal LCx with NC balloon 3.5 / 18 mm at 18 atm. DES was implanted at LCx at 20 atm. We did post dilatation at LCx with NC balloon up to 24 atm. Final angiogram showed TIMI III flow.

Case Summary
ECG finding in double culprit STEMI may be more diffuse than in single vessel STEMI. The challenge lies in identifying both culprit lesions during acute phase STEMI. In our case the lesions are more obvious. The lesion in RCA was addressed first because the distal flow was still good and we did not want any abrupt closure of the vessel since there were a large amount of thrombus in the lesion.