Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_040
Severe Consequence of Calcified Coronary Lesion Procedure: When Coronary Fenestration and Stenting Strategy Is a Rescue Option
By Teuku Rahadiyan
Presenter
Teuku Rahadiyan
Authors
Teuku Rahadiyan1
Affiliation
Raden Mattaher General Hospital, Indonesia1
View Study Report
CASE20251106_040
Coronary - Complication Management
Severe Consequence of Calcified Coronary Lesion Procedure: When Coronary Fenestration and Stenting Strategy Is a Rescue Option
Teuku Rahadiyan1
Raden Mattaher General Hospital, Indonesia1
Clinical Information
Relevant Clinical History and Physical Exam
A 66-year-old woman complained of recurrent typical chest pain with Canadian Classification Score of 3. There was progressive worsening symptom of angina in recent days before procedure. The patient had hypertension and hyperlipidemia as risk factors, a history of previous unstable angina pectoris and had been hospitalized at another hospital several months ago. Vital sign and physical examination were stable during pre-procedure hospitalization and during follow-up at the outpatient clinic
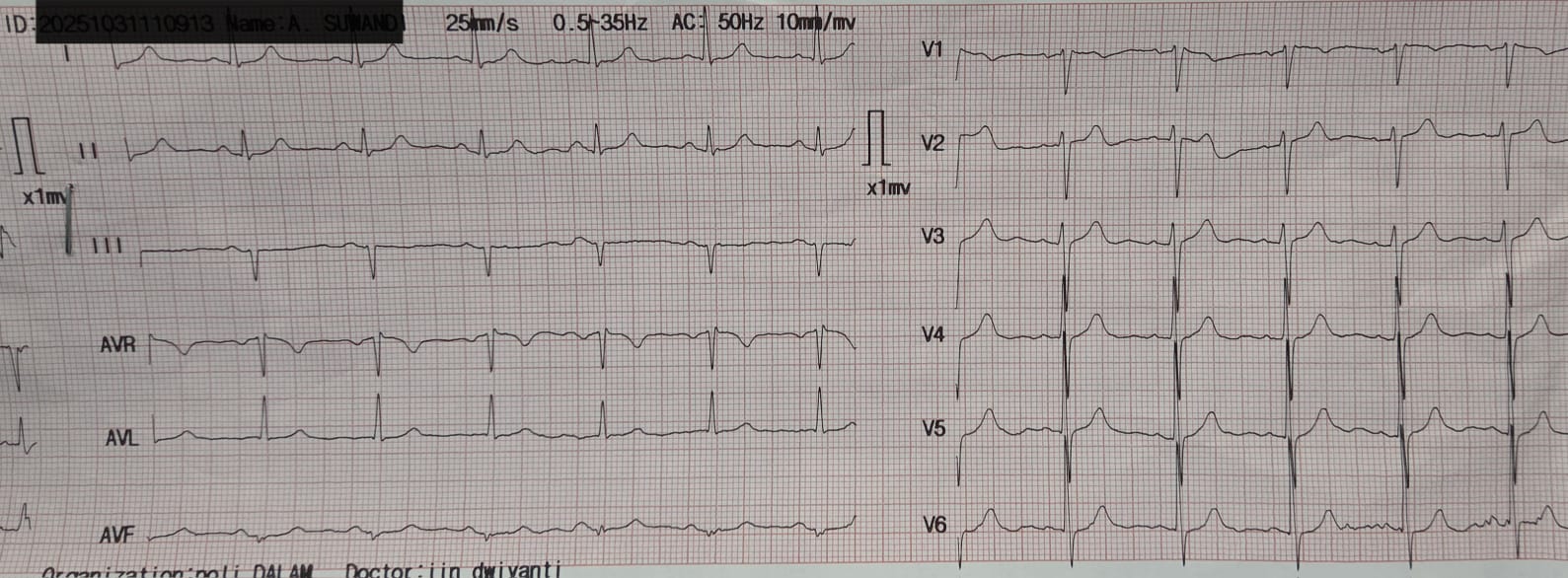
Relevant Test Results Prior to Catheterization
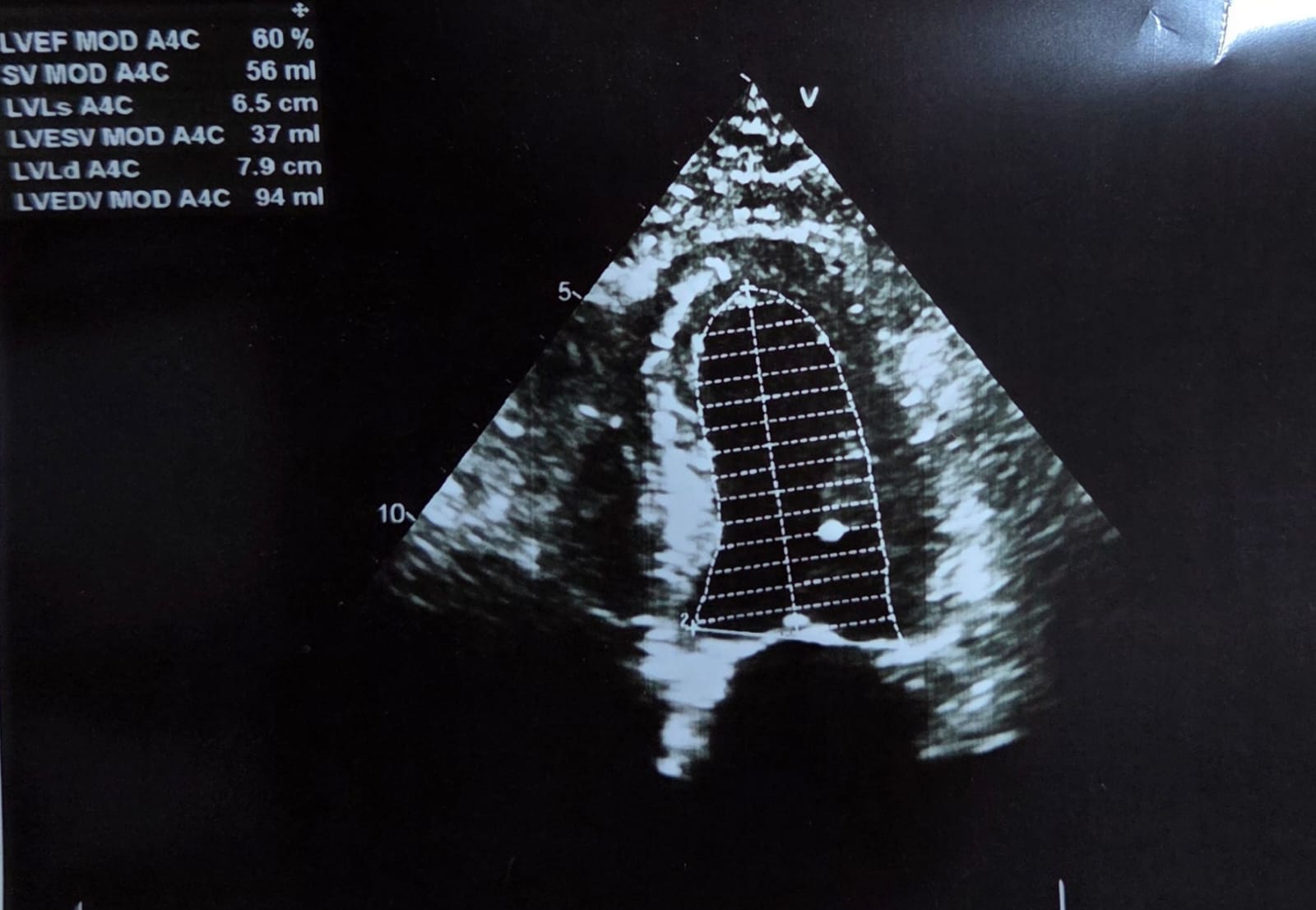
An electrocardiogram showed sinus rhythm with slight ST-segment depression in leads II, III, and AVF. An echocardiogram revealed normal left ventricular systolic function with an ejection fraction of 60% and no regional wall motion abnormalities.
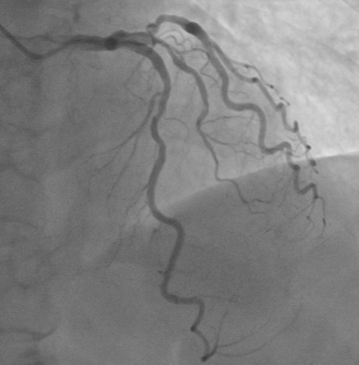
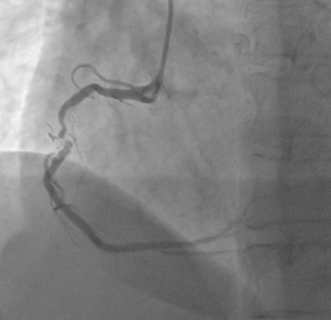
Relevant Catheterization Findings
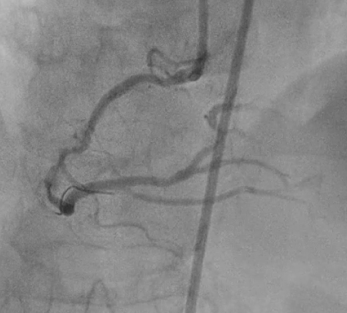
Right Coronary Angiography via right radial artery using 5 Fr TIG Optitorque demonstrated a tight lesion at mid part of Right Coronary Angiography (RCA) with heavy calcification. Left coronary angiography demonstrated non-significant stenosis at Left Anterior Descendent (LAD) and Left Circumflex (LCx) arteries. Therefore, the patient was planned to undergo PCI procedure via femoral access with IVUS guidance and preparation for rotablation.

 Diagnostic LAD.avi
Diagnostic LAD.avi
Diagnostic RCA-1.avi
Diagnostic RCA-2.avi
Interventional Management
Procedural Step
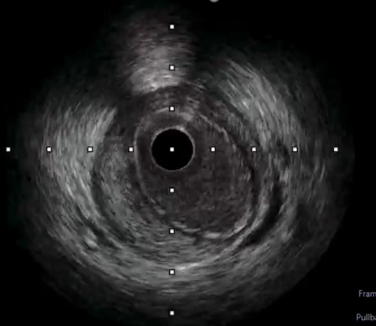
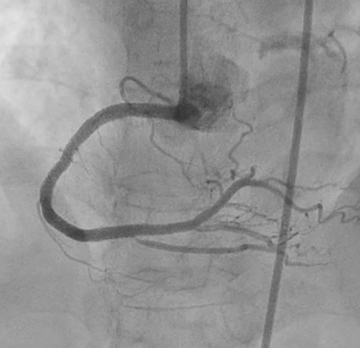
PCI began by engaging a 7Fr JR 4.0 to the RCA ostium via right femoral artery. Wiring initially performed with Runthrough NS through Fine Cross microcatheter, but wire entered subintimal space. Several manipulations to reposition the wire were unsuccessful. Immediate contrast injection showed no flow to the distal part due to abrupt closure of the RCA Patient became angina with marked ST-segment elevation. Rewiring was immediately attempted using Fielder XT-A through Fine Cross microcatheter and the wire successfully entered true lumen A 1.5 x 1.5 mm NC balloon was placed at the lesion but balloon ruptured.A 2.0 x 15 mm NC balloon with extension catheter as support but balloon ruptured.Finally A 2.0 x 20 mm NC scoring balloon successfully inflated then flow was restored with TIMI III flow.Angina relieved, ST-segment lower and hemodynamic improvedIVUS showed massive-compressive intra mural hematoma along distal to proximal RCA with intimal tear of dissection, and the wire within false lumen at mid part RCA.Coronary fenestration attempted using 3.0 x 15 mm NC scoring balloon inflation with dual guidewire inside the lumen.Hematoma surprisingly propagated marked by contrast trapping and no flow to PLBFenestration performed again using 2.5 x 15 mm NC scoring balloon and flow successfully restored.Four DES finally decided to be deployed at distal to ostial RCAFinal angiogram showed excellent result with TIMI III flow, hematoma was disappeared with good stent apposition on IVUS examination
Abrupt closure movie.mp4
IVUS movie.mp4
Final angio movie.mp4
Case Summary
This case demonstrates that calcification in atherosclerotic plaques can contribute to complications during PCI. Intimal tears resulting from dissection leading to iatrogenic compressive intramural hematoma is life-threatening complication, and the challenge of managing this complication is crucial due to its serious consequence if not addressed promptly. Coronary fenestration and stenting strategies should be considered as rescue options to address these complications.