Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_039
2 CTO, 1 Fistula: An Artery-to-Vein Twist In DVT Intervention
By Tsung-Ping Jeng, Jen-Kuang Lee
Presenter
Tsung-Ping Jeng
Authors
Tsung-Ping Jeng1, Jen-Kuang Lee2
Affiliation
National Taiwan University Hospital, Taiwan1, Division of Cardiology, Internal Medicine-National Taiwan University Hospital, Taiwan2
View Study Report
CASE20251106_039
Endovascular - Iliac / SFA Intervention
2 CTO, 1 Fistula: An Artery-to-Vein Twist In DVT Intervention
Tsung-Ping Jeng1, Jen-Kuang Lee2
National Taiwan University Hospital, Taiwan1, Division of Cardiology, Internal Medicine-National Taiwan University Hospital, Taiwan2
Clinical Information
Relevant Clinical History and Physical Exam
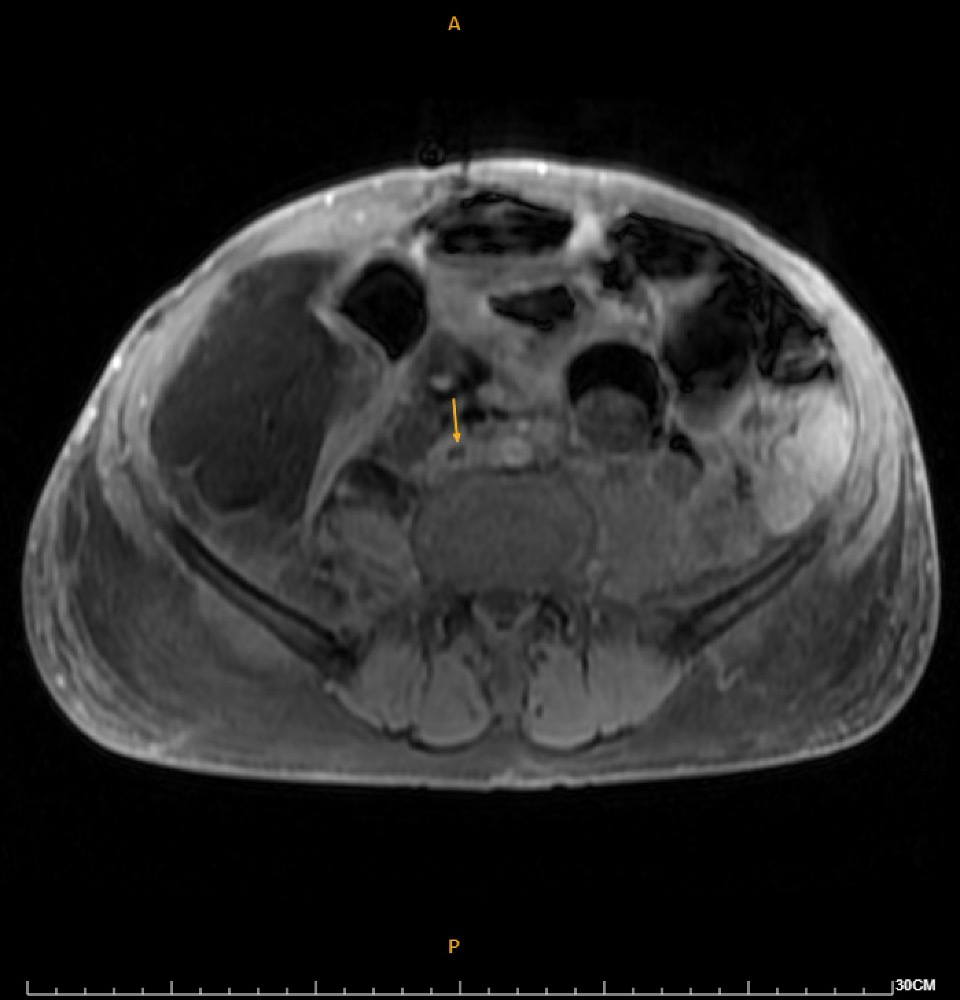
A 69-year-old man with recurrent retroperitoneal well-differentiated liposarcoma presented with fever, dysuria, and progressive right leg swelling and pain. Examination showed right leg warmth, grade II pitting edema, and tender telangiectasia over the right groin, suggesting DVT.

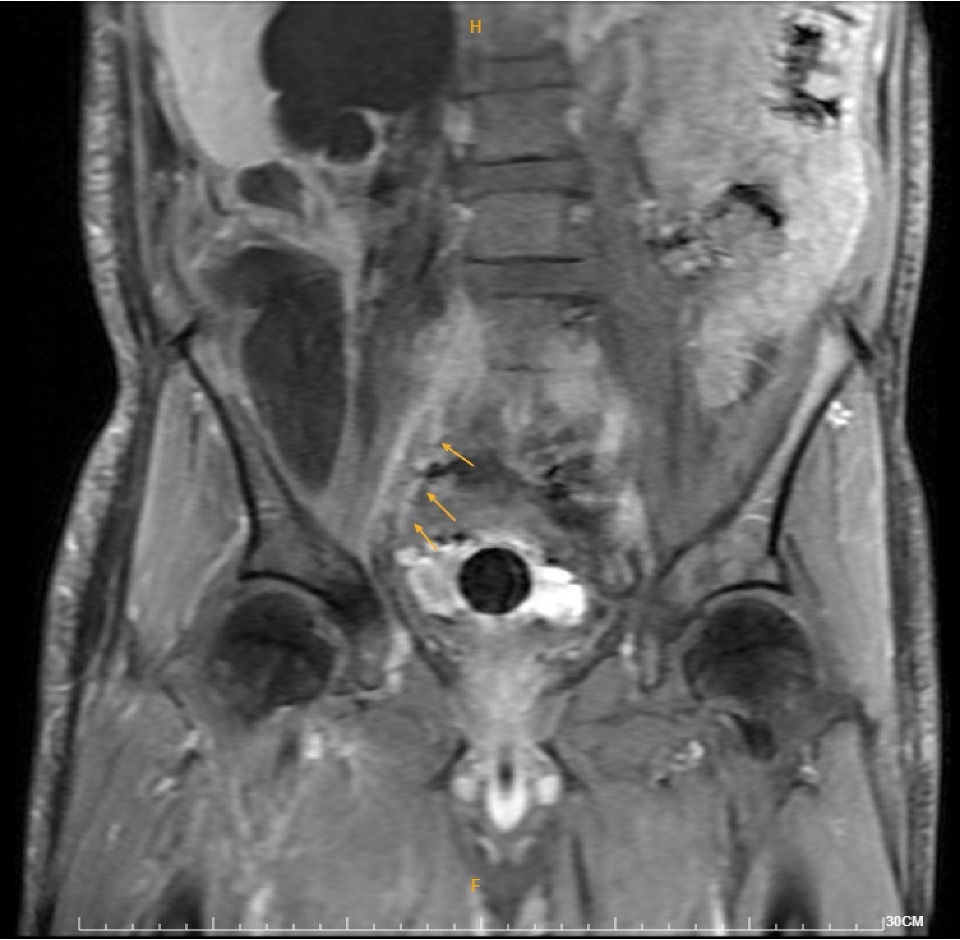
Relevant Test Results Prior to Catheterization
Duplex ultrasound demonstrated thrombosis from the right common femoral vein to the calf veins. MRI revealed a 16.8-cm retroperitoneal fat-containing tumor causing severe right hydronephrosis, and extensive thrombosis involving the right common, external, and internal iliac arteries, lower IVC, iliac, and femoral veins. DVT intervention was arranged.
Relevant Catheterization Findings
Catheterization revealed total occlusion of the right common iliac artery, likely due to tumor compression. Diffuse thrombosis was seen in the right common femoral vein, with total occlusion from the right common iliac vein to proximal RCFV. LCIV ostial stenosis (~80%) and IVC stenosis (~90%) were also present.

Interventional Management
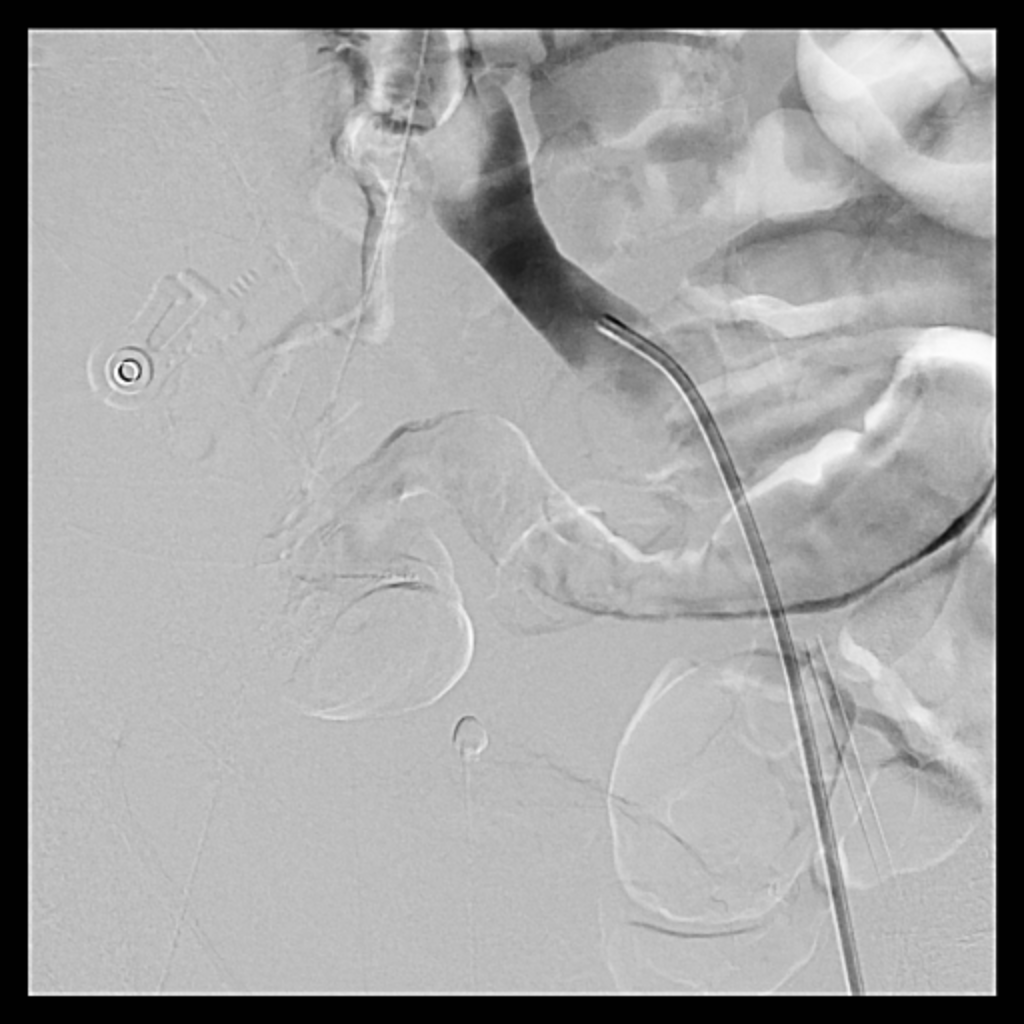
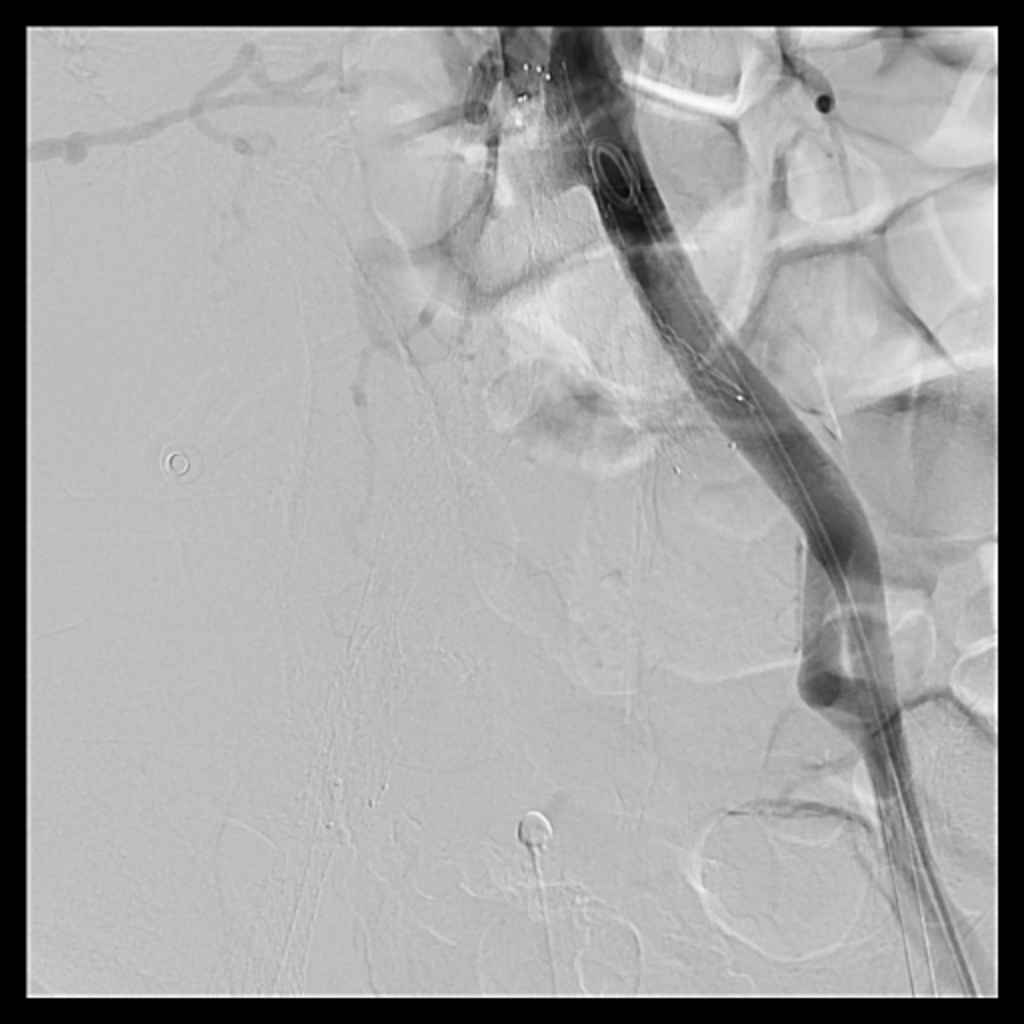
Procedural Step
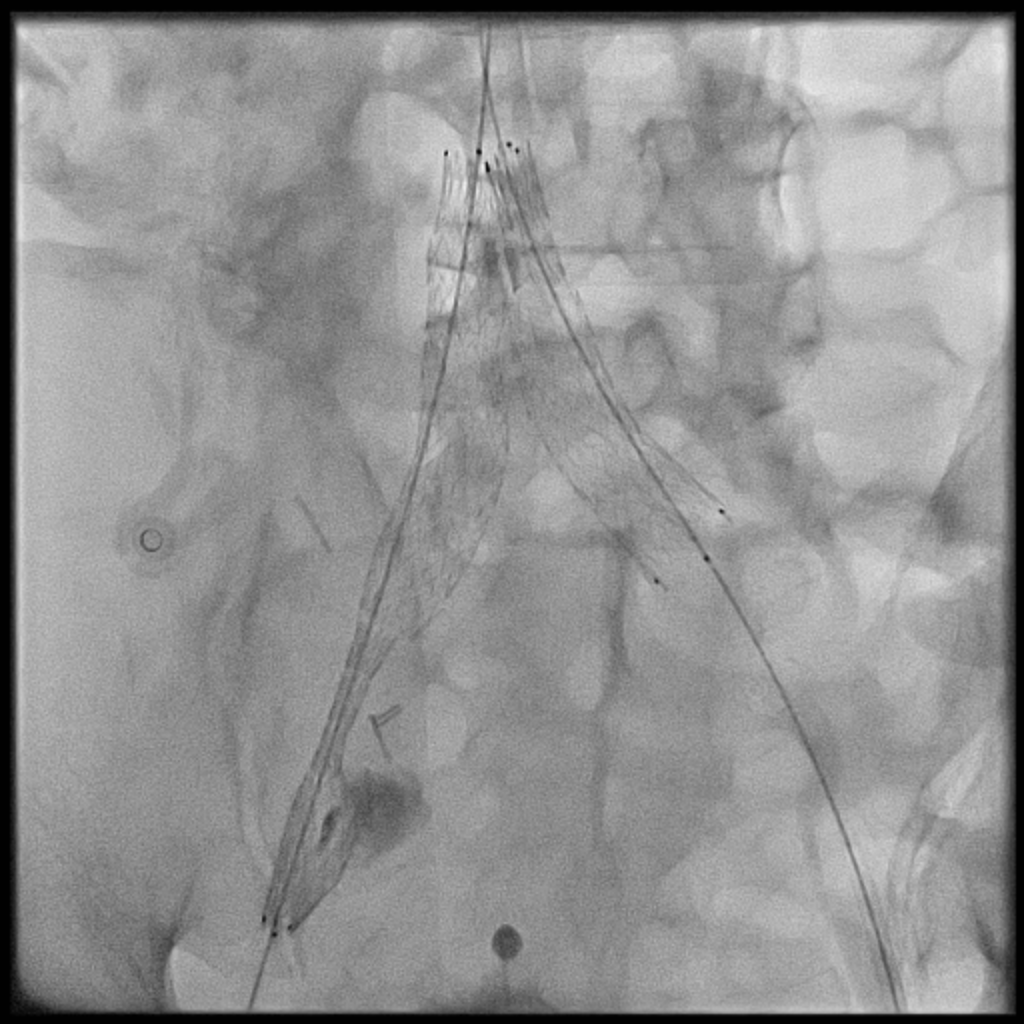
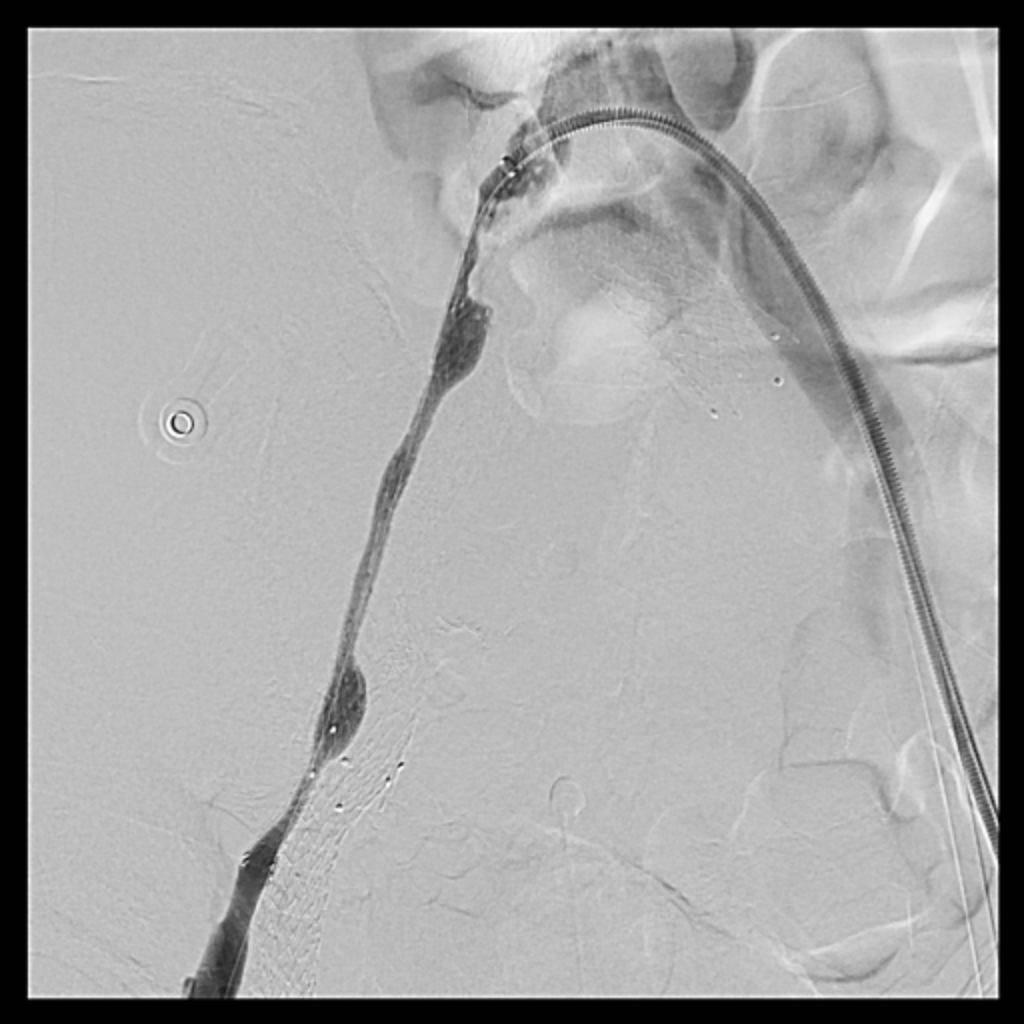
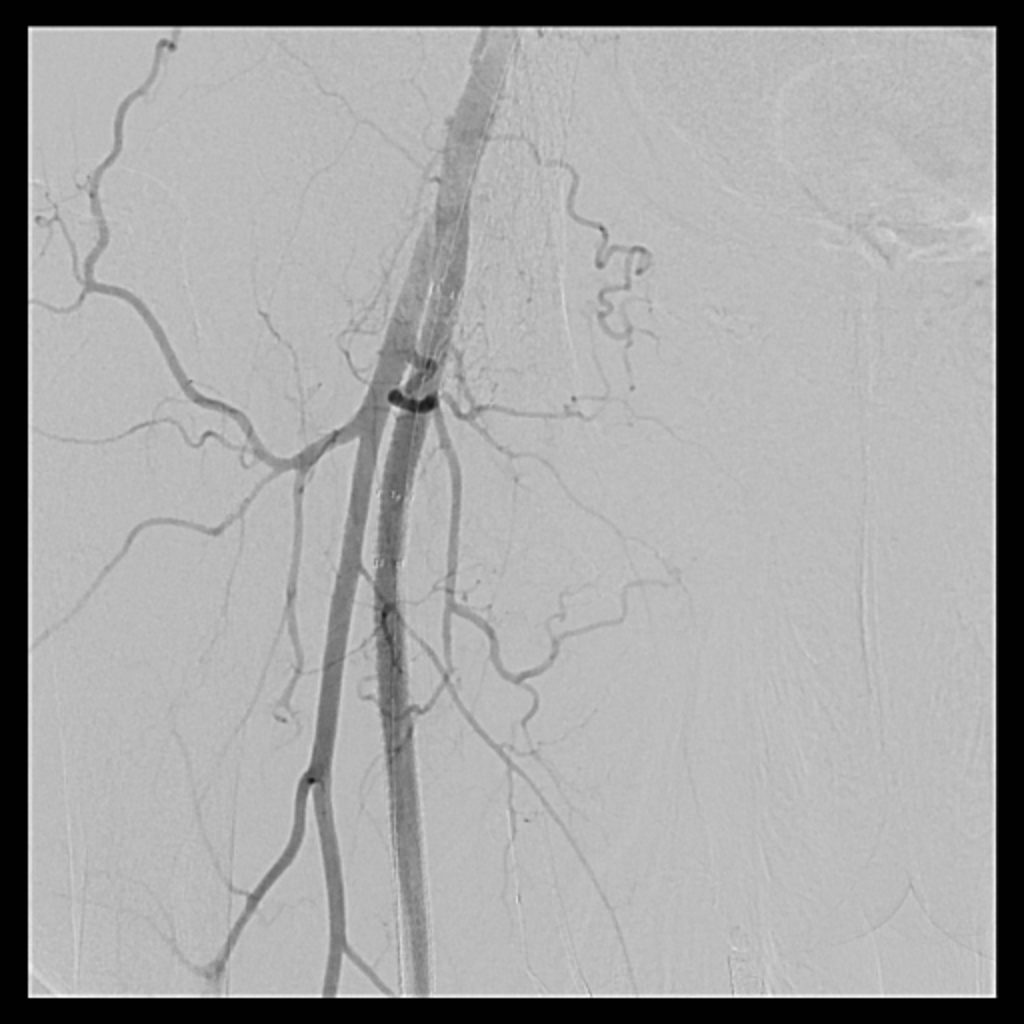
Venous access was obtained and venography confirmed heavy thrombus burden; therefore, the initial 6 Fr sheath was upsized to a 9 Fr sheath. Two Terumo stiff wires were advanced into the IVC to secure stable access. Mechanical thrombectomy using the Boston Scientific AngioJet system was performed from the right iliac vein to the right common femoral vein. During venography, unexpected early arterial opacification suggested an iatrogenic artery-to-vein fistula. Iliac angiography was then performed, revealing a total occlusion of the right common iliac artery with collateral reconstitution. To restore arterial flow and seal the fistula, a contralateral approach was used. A wire successfully crossed the occluded segment into the true lumen, followed by deployment of a covered stent. Final angiography showed complete closure of the fistula and restored antegrade arterial flow without distal embolization. The patient remained hemodynamically stable.
 RCIA CTO pass.mp4
RCIA CTO pass.mp4
RSFA cover stent with AV sheath removal.mp4
RDFA antegrade wiring into tumor feeding aretery.mp4
Case Summary
This case demonstrates that venous interventions may unexpectedly expose silent arterial disease. Rapid recognition of arterial opacification led to timely management of an iatrogenic artery-to-vein fistula and unrecognized arterial occlusion. Endovascular therapy enabled simultaneous rescue and reconstruction with excellent immediate outcomes.