Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_036
From Cath Lab to Surgery Room: A Multidisciplinary Triumph in Managing Total Occlusion Giant Right Coronary Artery Aneurysm With Fistulous Drainage and Pulmonary Thromboembolism
By Akbar Sinaga, Myeong Gon Kim
Presenter
Akbar Sinaga
Authors
Akbar Sinaga1, Myeong Gon Kim1
Affiliation
Catholic Kwandong University-International St Mary Hospital, Korea (Republic of)1
View Study Report
CASE20251106_036
Coronary - Surgical Therapy (Coronary)
From Cath Lab to Surgery Room: A Multidisciplinary Triumph in Managing Total Occlusion Giant Right Coronary Artery Aneurysm With Fistulous Drainage and Pulmonary Thromboembolism
Akbar Sinaga1, Myeong Gon Kim1
Catholic Kwandong University-International St Mary Hospital, Korea (Republic of)1
Clinical Information
Relevant Clinical History and Physical Exam
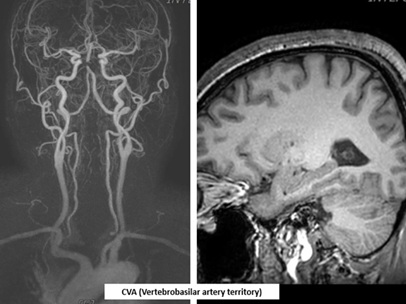
A55-year-old man with previous percutaneous coronary intervention for STEMI, vertebrobasilar infarction, and recent thoracic endovascular aortic repair (TEVAR) for a descending thoracic aortic aneurysm presented to the emergency department with acute chest and back pain without any trauma. He also had hypertension, diabetes, hyperlipidemia, and routinely take the medication. On arrival, his vital signs showed a markedly elevated blood pressure of 178/120 mmHg, while the others within normal limit.

Relevant Test Results Prior to Catheterization
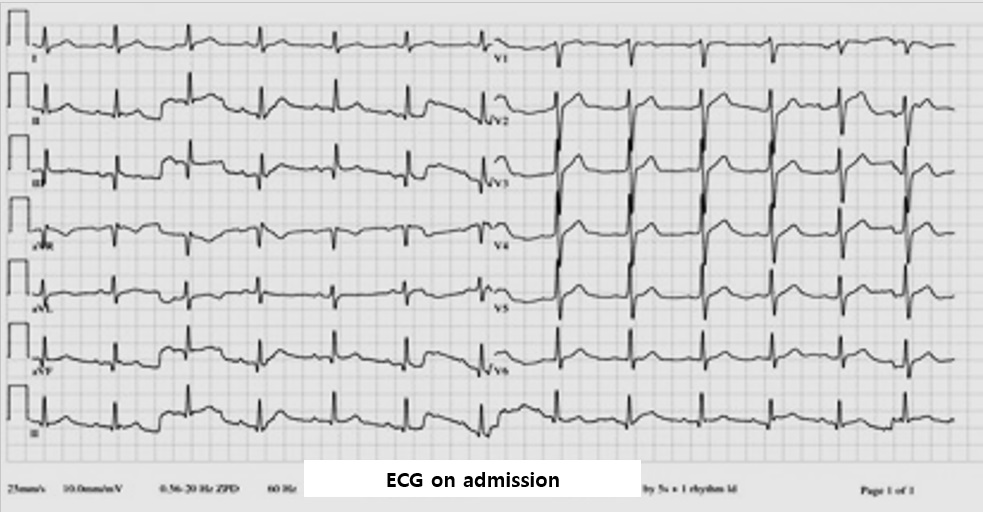
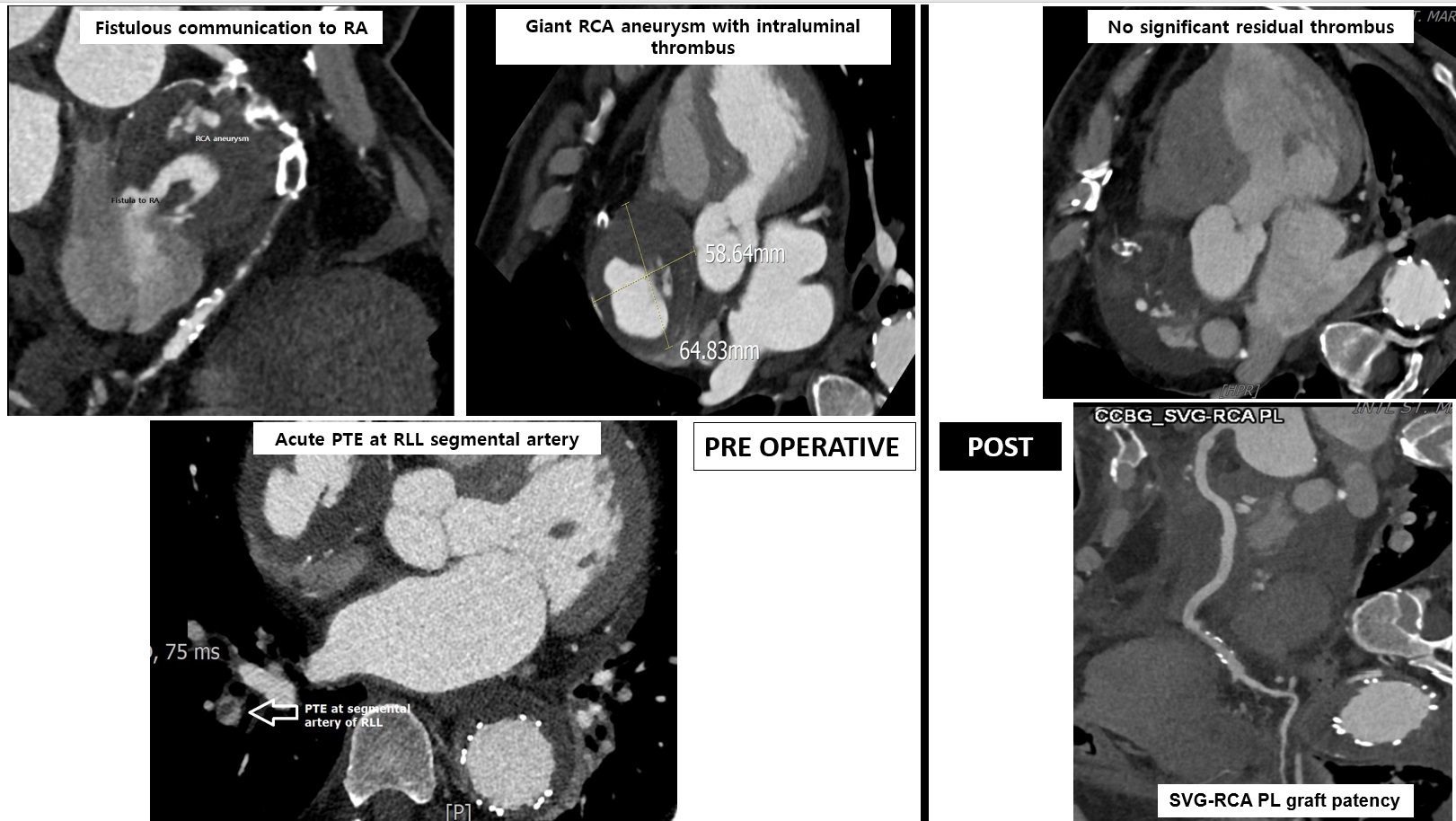
EKG showed no new ischemic changes. Laboratory result revealed mildly elevated inflammatory markers and NT-proBNP, with normal troponin. CT angiography identified a 5.9×6.5 cm giant RCA aneurysm with thrombus, total mid-distal RCA occlusion, a fistula to the right atrium, and also probable acute pulmonary embolism involving the segmental branch of the right lower lobe.
Relevant Catheterization Findings
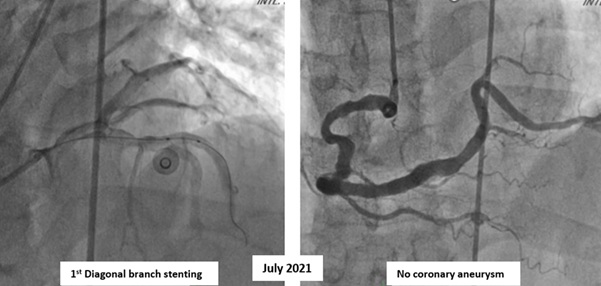
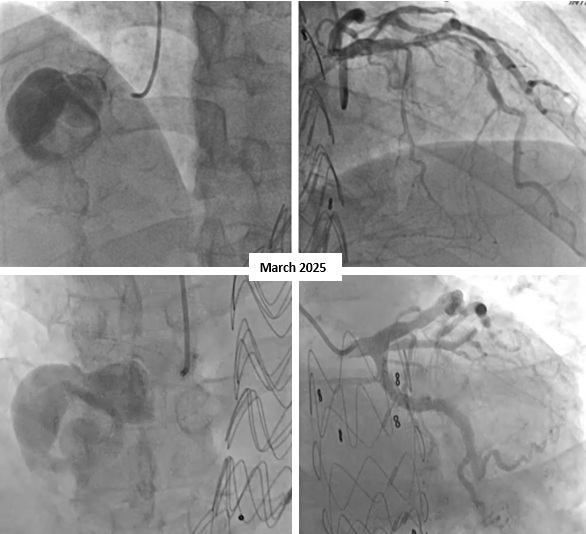
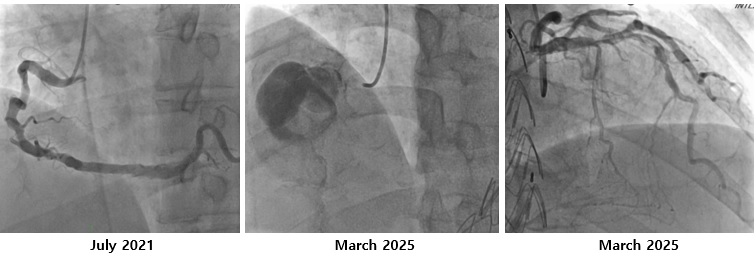
The coronary angiography showed a giant right coronary artery (RCA) aneurysm with total occlusion at mid-RCA and collateral flow from the left circumflex artery. It is different with right coronary angiography at 4 years ago that showed no coronary aneurysm. The left coronary artery has a good flow to the distal without any significant stenosis and patent stent on 1st diagonal artery branch.
Interventional Management
Procedural Step
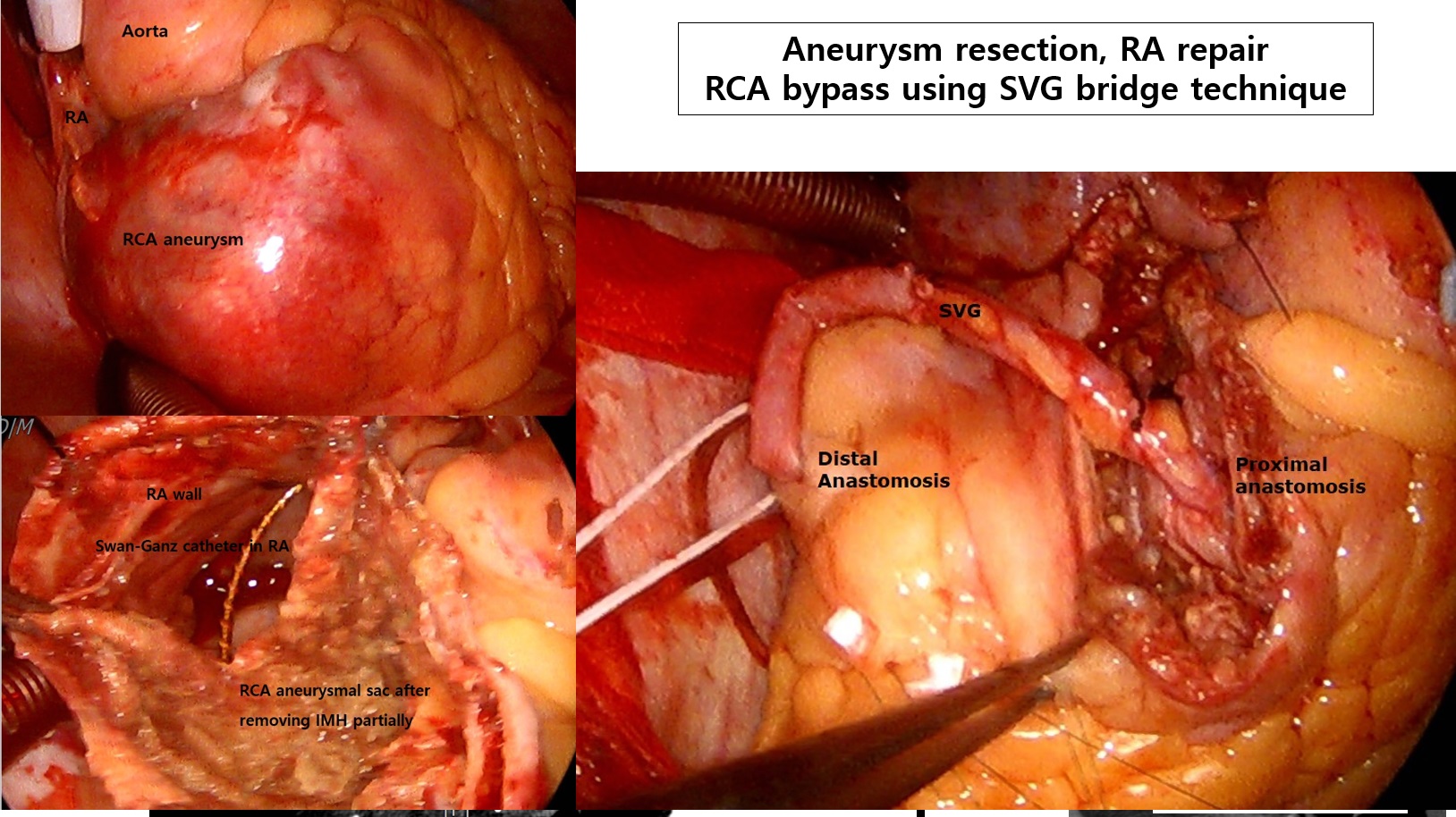
After discussing with the heart team, the surgery was planned. After several days of patient's condition improvement, the surgical was performed. Surgical exploration was undertaken via median sternotomy. Intraoperative findings included a giant RCA aneurysm measuring approximately 6 cm with massive intramural haematoma, a fistulous connection to the RA, and a proximally visible RCA orifice with distal total occlusion. The aneurysmal sac was resected, the RA wall was repaired, and a coronary artery bypass graft (CABG) was performed using a reversed saphenous vein graft from the proximal RCA to the distal RCA segment. Echocardiography on 4th day postoperative day (POD 4) showed preserved biventricular function without residual mass. Coronary CT angiography on POD 7 confirmed patent RCA graft and resolution of the aneurysmal mass.
Case Summary
This case exemplifies the importance of early surgical referral in patients with symptomatic giant coronary aneurysms, especially when complicated by fistulous drainage or thromboembolic phenomena. Furthermore, it underscores the value of a multidisciplinary approach in the diagnosis and perioperative management of such complex cardiovascular cases.