Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_035
Utilizing Near-Infrared Spectroscopy in Combination With Intravascular Ultrasound to Identify the Etiology of Cardiac Arrest
By Samarth Jani, Rohan Kaul, Rahul Kurup
Presenter
Samarth Jani
Authors
Samarth Jani1, Rohan Kaul1, Rahul Kurup1
Affiliation
Campbelltown Hospital, Australia1
View Study Report
CASE20251106_035
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Utilizing Near-Infrared Spectroscopy in Combination With Intravascular Ultrasound to Identify the Etiology of Cardiac Arrest
Samarth Jani1, Rohan Kaul1, Rahul Kurup1
Campbelltown Hospital, Australia1
Clinical Information
Relevant Clinical History and Physical Exam
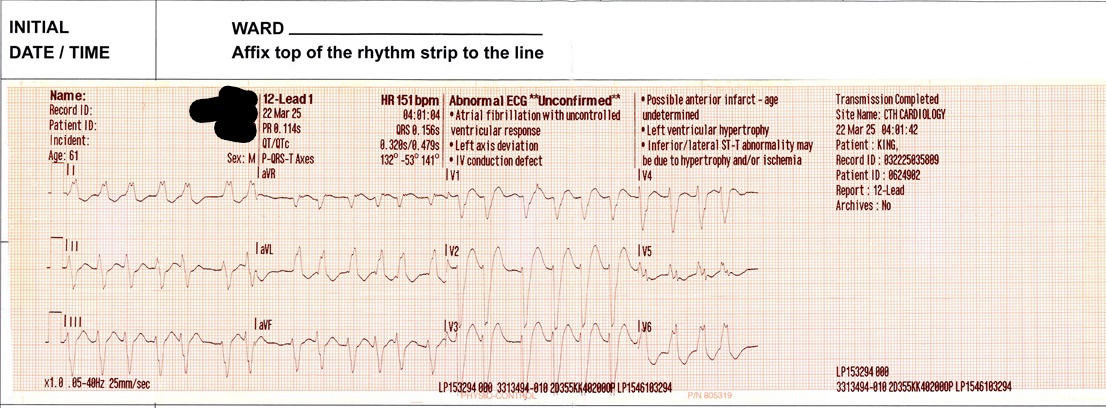
A 61 year old male presented to Campbelltown Hospital following an in hospital cardiac arrest at another centre. This was five days post left hip replacement. He had a known left bundle branch block but no coronary disease.
Return of spontaneous circulation was achieved after two cycles of CPR and one shock for ventricular tachycardia. Post arrest he had wide complex tachycardia, likely VT, and was treated with intravenous amiodarone. No ECG from arrest available.
Attached:
- Post ROSC ECG in ED
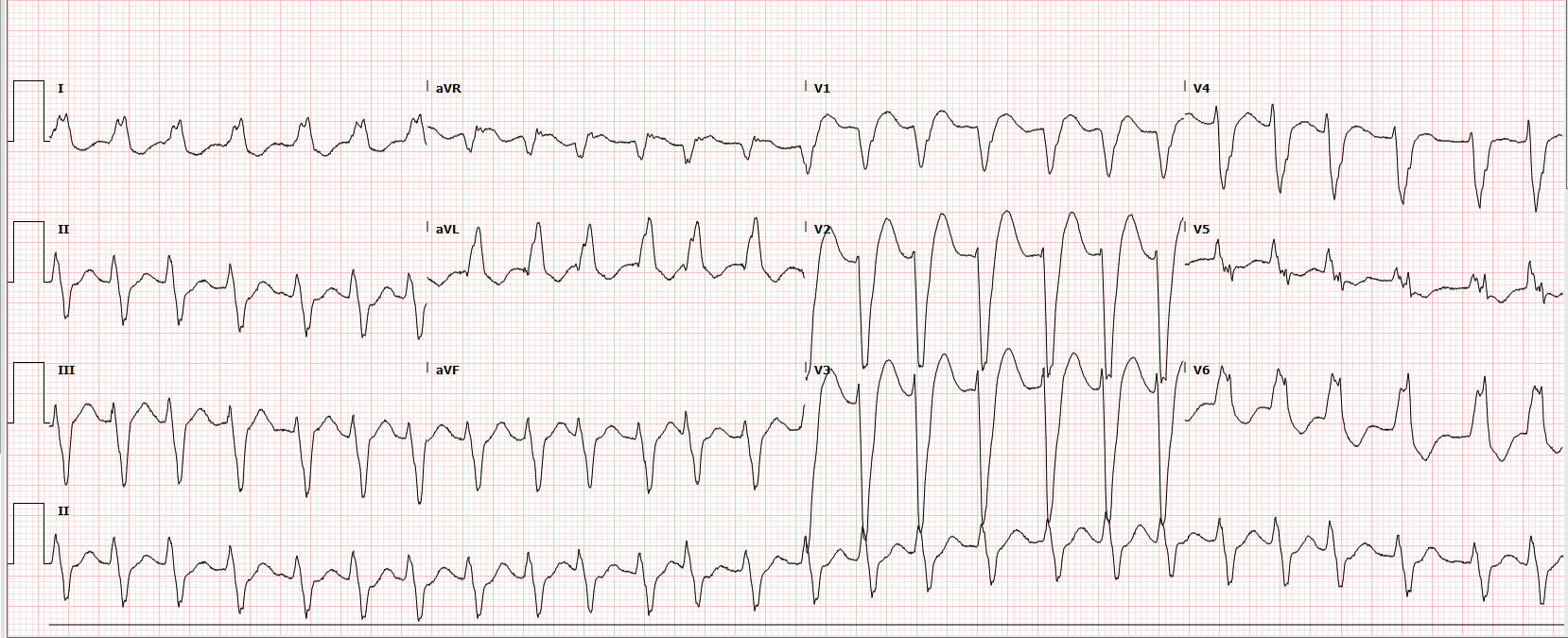
Return of spontaneous circulation was achieved after two cycles of CPR and one shock for ventricular tachycardia. Post arrest he had wide complex tachycardia, likely VT, and was treated with intravenous amiodarone. No ECG from arrest available.
Attached:
- Post ROSC ECG in ED
Relevant Test Results Prior to Catheterization
CT pulmonary angiography undertaken post cardiac arrest showed no pulmonary embolism, aortic, or mediastinal pathology. Transthoracic echocardiogram revealed moderate left ventricular
systolic dysfunction with regional wall motion abnormalities affecting mid to distal anteroseptal, inferoseptal, anterior, and anterolateral segments. Troponin peaked at 1800 ng/L.
systolic dysfunction with regional wall motion abnormalities affecting mid to distal anteroseptal, inferoseptal, anterior, and anterolateral segments. Troponin peaked at 1800 ng/L.
Relevant Catheterization Findings
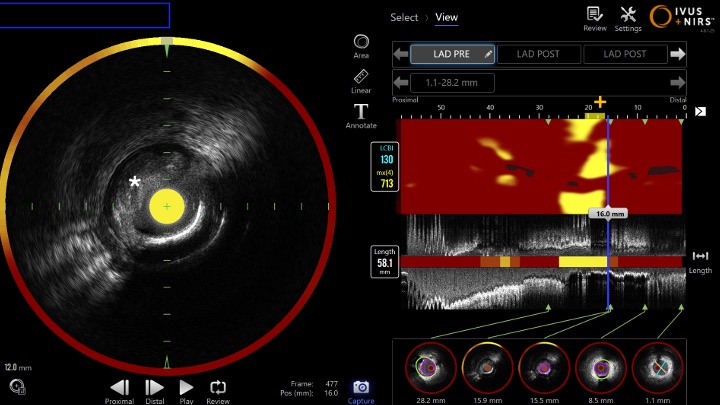
Invasive coronary angiography demonstrated a 95% stenosis in the proximal left anterior descending artery. Combined Near Infrared Spectroscopy (NIRS) and Intravascular Ultrasound (IVUS) imaging identified minimal calcification with features consistent with plaque rupture, therefore identifying the culprit lesion as the cause of the cardiac arrest.
Interventional Management
Procedural Step
Coronary angiography was performed via right radial access. Angiography demonstrated a right dominant system with severe (95%) proximal LAD stenosis - 30 mm long Type C lesion.
After administration of 180 mg ticagrelor and 8000 IU heparin, the lesion was crossed. Pre dilatation was performed using a 3.5 mm non compliant Trek (Abbott, California, USA) balloon. Makoto NIRS-IVUS DualPro (InfraredX - Nipro Corp, Massachusetts, USA) imaging revealed minimal calcification and clear evidence of plaque rupture with a large lipid core burden index (LCBI = 700). An Onyx Frontier drug eluting stent (Medtronic, Ireland) was deployed near to the ostium. Post dilatation was performed with a 3.5 mm and 4.0 mm noncompliant balloon.
Repeat IVUS assessment showed stent under expansion proximally, therefore was post dilated again with 4.0 mm noncompliant and 4.5 mm semi compliant balloon proximally.
There was excellent angiographic and IVUS result with a distal minimal stent area of (MSA) 9.1 mm2 and stent expansion (SE) of greater than 90%.
The patient was discharged two days post angiogram on dual anti platelets for twelve months.
Images attached:
- Baseline LAD Angiogram
- Post PCI LAD Angiogram
- Near Infrared Spectroscopy (NIRS) and IVUS image showing lipidic plaque and rupture
* = site of plaque rupture
+ = site of maximum lipid arc (yellow) --> measured as LCBI (Lipid Core Burden Index)


After administration of 180 mg ticagrelor and 8000 IU heparin, the lesion was crossed. Pre dilatation was performed using a 3.5 mm non compliant Trek (Abbott, California, USA) balloon. Makoto NIRS-IVUS DualPro (InfraredX - Nipro Corp, Massachusetts, USA) imaging revealed minimal calcification and clear evidence of plaque rupture with a large lipid core burden index (LCBI = 700). An Onyx Frontier drug eluting stent (Medtronic, Ireland) was deployed near to the ostium. Post dilatation was performed with a 3.5 mm and 4.0 mm noncompliant balloon.
Repeat IVUS assessment showed stent under expansion proximally, therefore was post dilated again with 4.0 mm noncompliant and 4.5 mm semi compliant balloon proximally.
There was excellent angiographic and IVUS result with a distal minimal stent area of (MSA) 9.1 mm2 and stent expansion (SE) of greater than 90%.
The patient was discharged two days post angiogram on dual anti platelets for twelve months.
Images attached:
- Baseline LAD Angiogram
- Post PCI LAD Angiogram
- Near Infrared Spectroscopy (NIRS) and IVUS image showing lipidic plaque and rupture
* = site of plaque rupture
+ = site of maximum lipid arc (yellow) --> measured as LCBI (Lipid Core Burden Index)
Case Summary
This case highlights the diagnostic and procedural value of integrating NIRS and IVUS imaging to identify the culprit plaque and optimize stent deployment. The combined use of these modalities can allow greater understanding of the cause of myocardial infarction, improving stent optimisation and procedural outcomes.