Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_034
Anterior STEMI Presenting With Cardiogenic Shock With Apical VSD – Management With ASD Device
By Rohit Mody
Presenter
Rohit Mody
Authors
Rohit Mody1
Affiliation
Mody Harvard Cardiac Institute & Research Centre , India1
View Study Report
CASE20251106_034
Coronary - High-Risk Intervention (Diabetes, Heart Failure, Renal Failure, Shock, etc)
Anterior STEMI Presenting With Cardiogenic Shock With Apical VSD – Management With ASD Device
Rohit Mody1
Mody Harvard Cardiac Institute & Research Centre , India1
Clinical Information
Relevant Clinical History and Physical Exam
65 years old male presented with Acute Anterior wall MIwindow period- 72hrs NIDDM Hypertensive Presented with Cardiogenic shock ECHOshows apical VSD EF 35% There was sever TR and PAHVSD was showing left to rightshunt with PAH RWMA in Anterior territory.

Relevant Test Results Prior to Catheterization
65 years old male presented with Acute Anterior wall MIwindow period- 72hrs NIDDM Hypertensive Presented with Cardiogenic shock ECHOshows apical VSD EF 35% There was sever TR and PAHVSD was showing left to rightshunt with PAH RWMA in Anterior territory.
Relevant Catheterization Findings
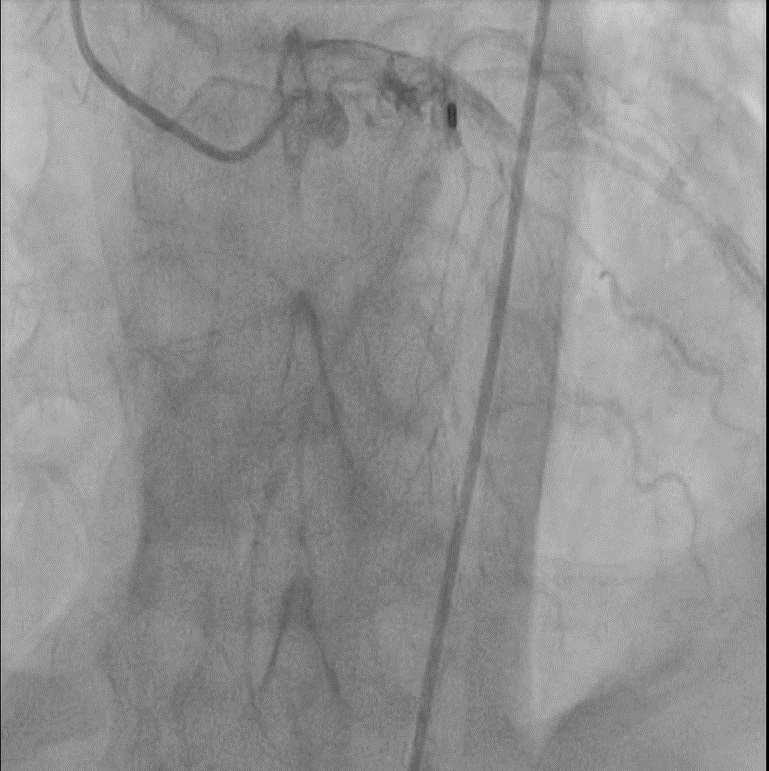
Angiogram reveals mid LAD100%, out of window period
Interventional Management
Procedural Step
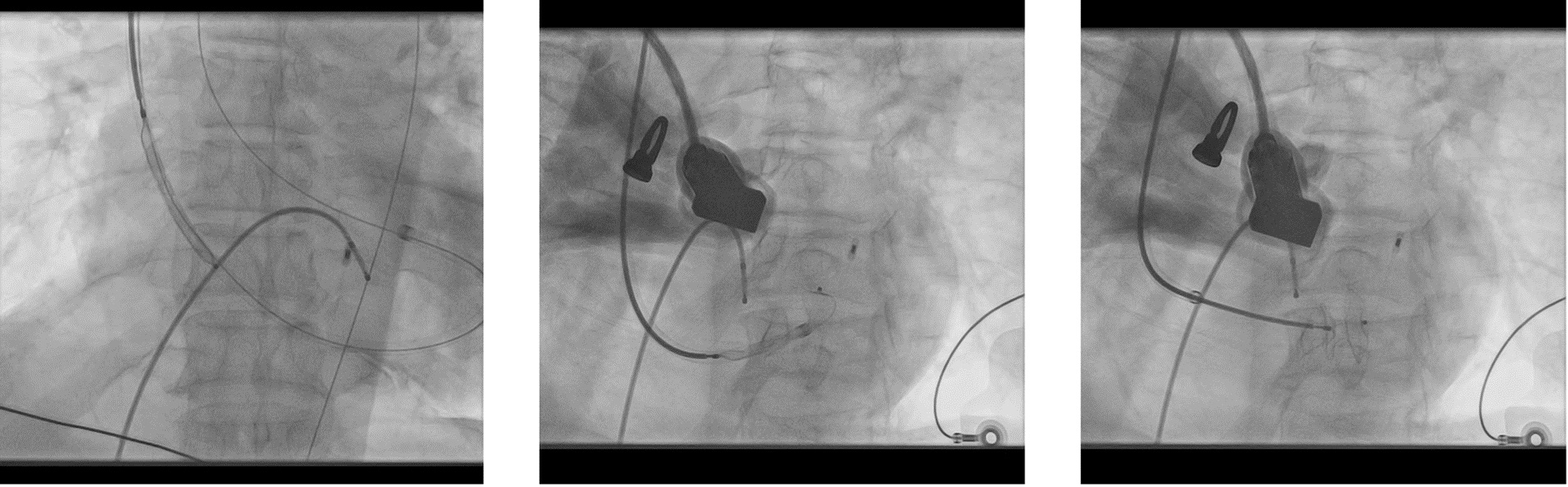
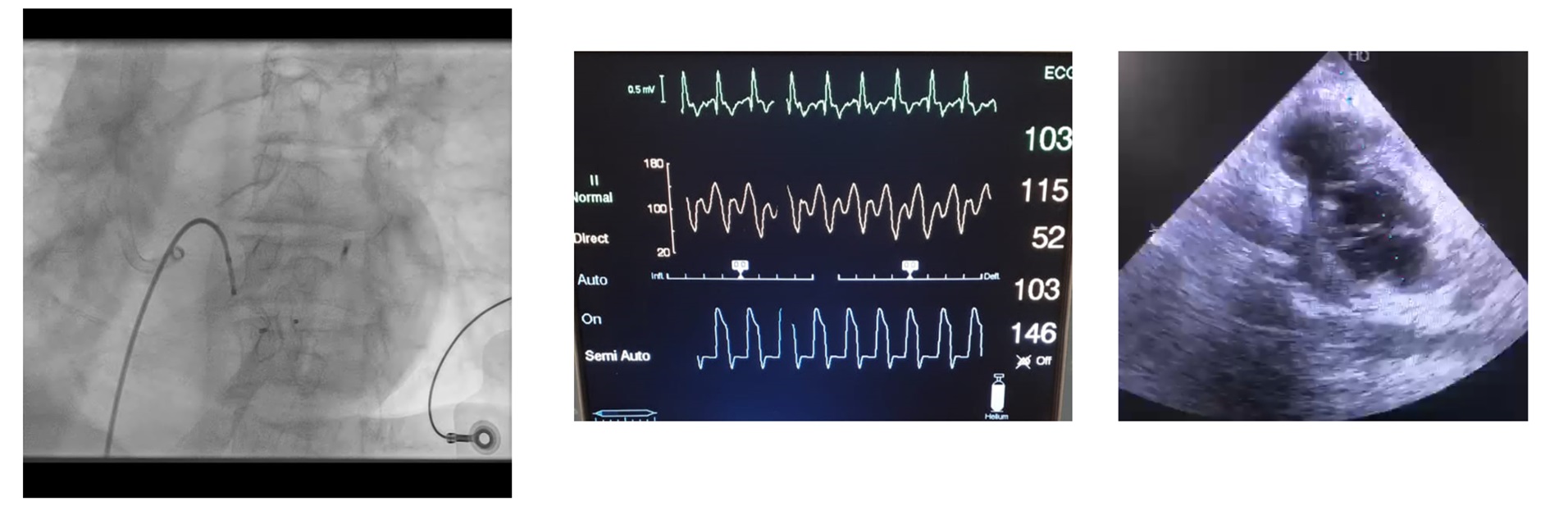
A 65-year-old hypertensive, diabetic male presented with acute anterior wall MI (window 72 hrs) complicated by cardiogenic shock and apical ventricular septal defect (VSD) on echocardiography, showing a significant left-to-right shunt with severe PAH and EF 35%. An intra-aortic balloon pump (IABP) was inserted for hemodynamic stabilization. The procedure was performed via dual access — 6F femoral arterial sheath and 8F internal jugular venous sheath. The left ventricle was cannulated, and the VSD was carefully crossed using a catheter and guidewire, which was advanced into the pulmonary artery. The wire was then snared through the VSD defect to establish an arteriovenous loop, providing stability for device delivery. Over this loop, an Amplatzer 14 mm ASD device was advanced through the 8F sheath and positioned across the apical VSD under echocardiographic and fluoroscopic guidance. After confirming proper alignment and stability, the device was successfully released, achieving complete closure of the shunt. Immediate echocardiography confirmed no residual flow across the septum. The patient was transferred to the CCU for monitoring, with gradual IABP weaning over 4–5 days. Follow-up echocardiography before discharge showed no residual shunt, improved hemodynamics, and stable LV function.

Case Summary
We conclude from this study that VSD device closureinsetting of Post MI is feasible and can be successful las an alternative tosurgery. In Extreme cases of hemodynamic instability and shock patient can betaken on MCS like ECMO. In our case we stabilized the patient with IABP supportand an NIV support. Although the most important risk factor for mortality ispresence of cardiogenic shock and closure in acute phase. We did our case at 72hrs. and patient was in cardiogenic shock. We used ASD device in this case asthere was adequate