Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_032
Saving the Toes: Bidirectional Approach With Needle Cracking for Intrapopliteal CTO
By Chia-Chen Lee
Presenter
Chia-Chen Lee
Authors
Chia-Chen Lee1
Affiliation
Taichung Veterans General Hospital, Taiwan1
View Study Report
CASE20251106_032
Endovascular - Iliac / SFA Intervention
Saving the Toes: Bidirectional Approach With Needle Cracking for Intrapopliteal CTO
Chia-Chen Lee1
Taichung Veterans General Hospital, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
An 75-year-old male has past medical history of CAD, TVD, statuspost CABG in 2021, followed by multiple PCI, CHF,HFmrEF (LVEF: 41%), NYHA Functional Class II, Stage C, ESRD on regularhemodialysis since November 2024 and type 2 Diabetes Mellitus, controlled withoral antidiabetic drugs. He suffered from poor wound healing of the right 2ndto 4th toes for over one month.

Relevant Test Results Prior to Catheterization
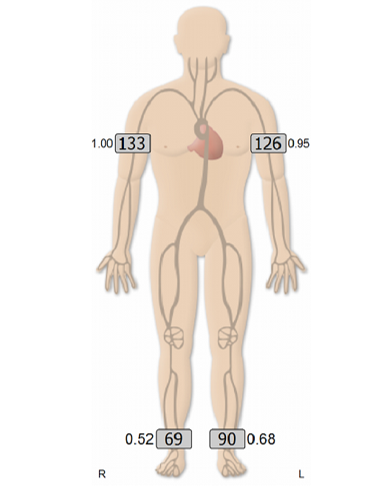
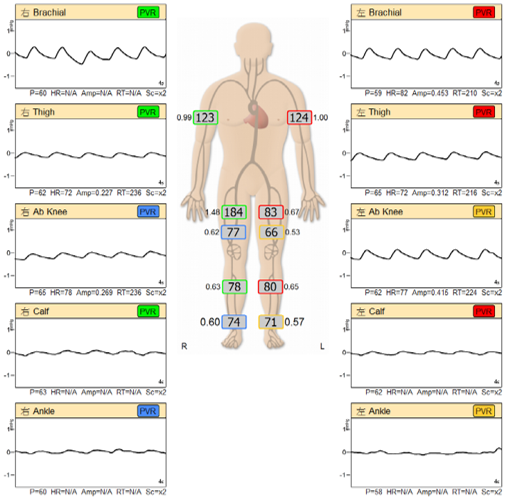
The ABI of right side was 0.52, while the left one was0.68. The PVR showed dampened waveform, absent dicrotic notch, and reducedamplitude especially over bilateral lower limbs, which indicate reduced bloodflow that can be a sign of peripheral artery disease.
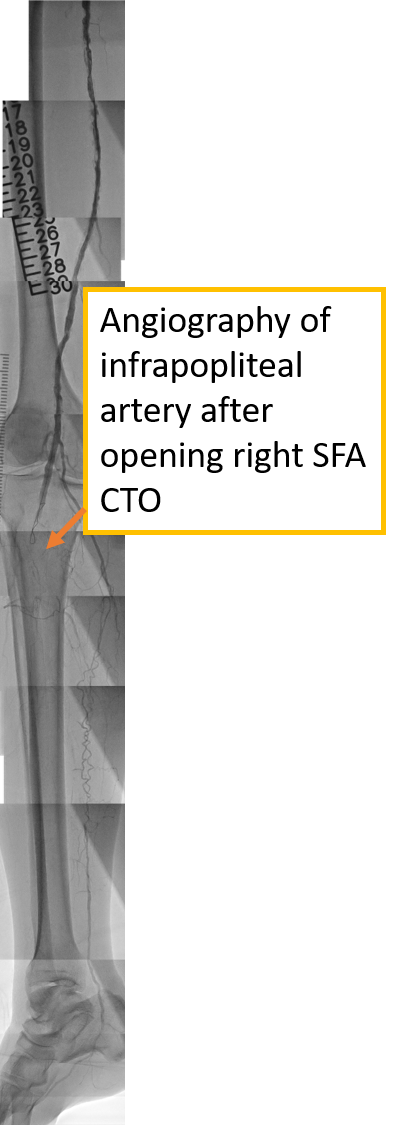
Relevant Catheterization Findings
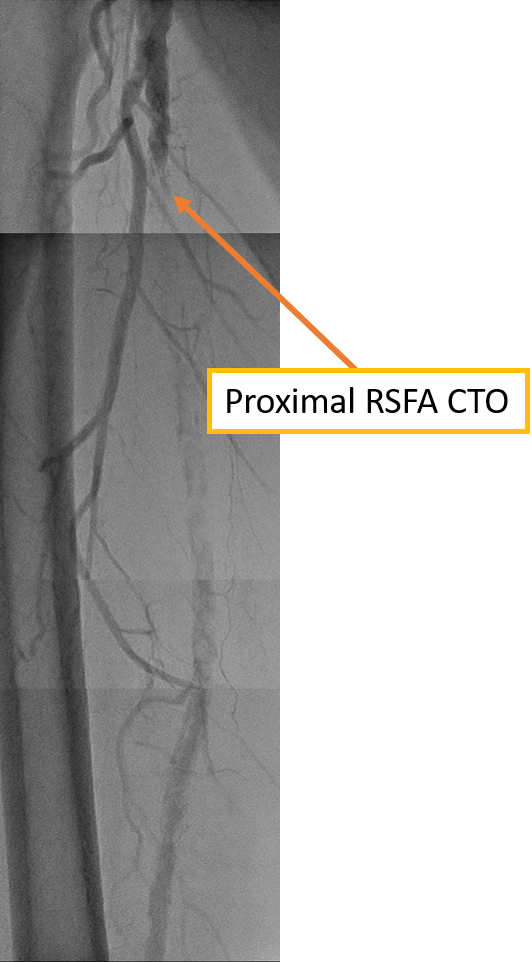
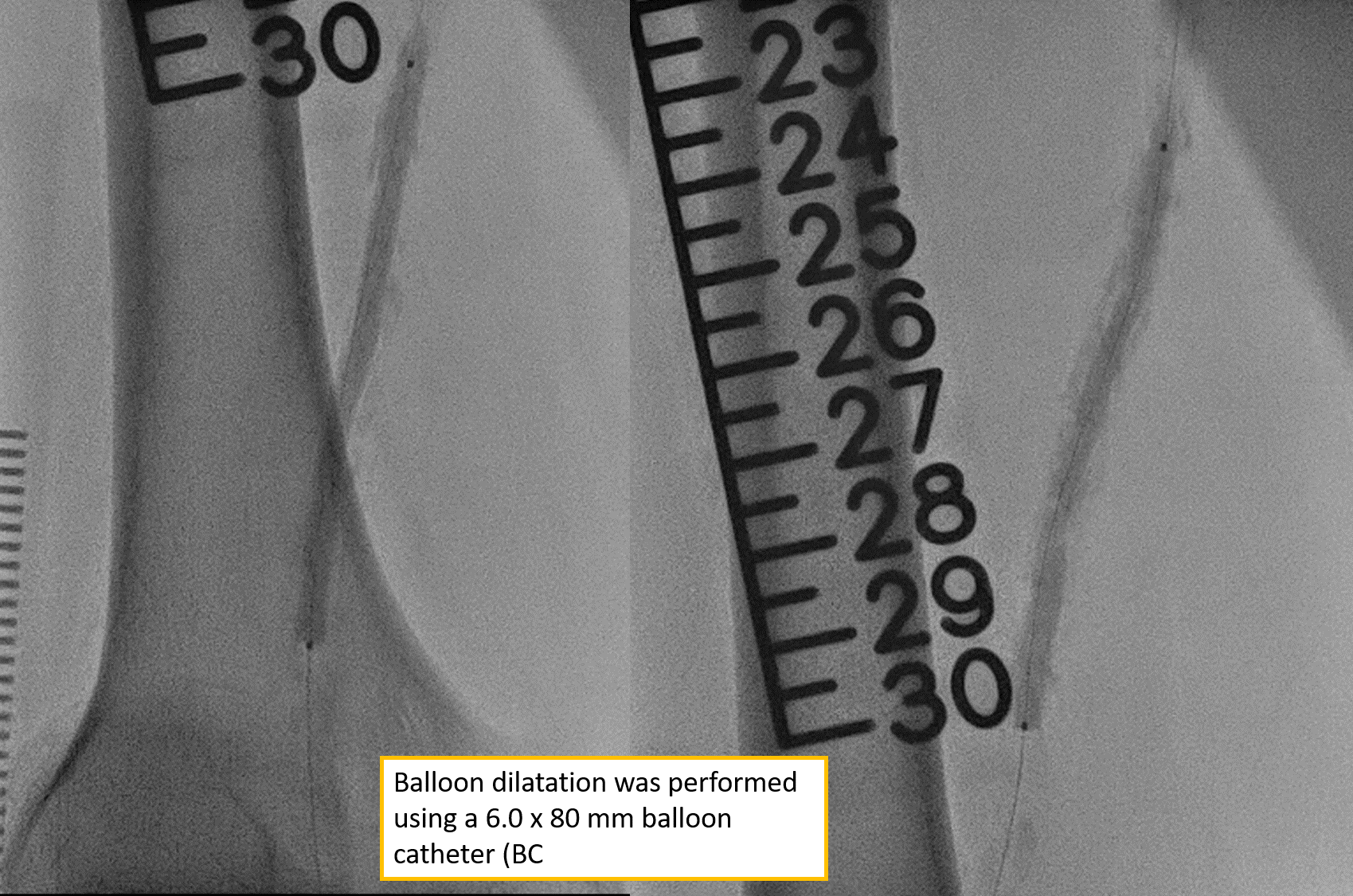
Right common femoralartery: Patent with atherosclerotic changeRSFA: CTO with heavy calcificationBalloondilatation was performed using a 6.0 x 80 mm balloon catheter (BC). However,the post dilatation angiography showed infrapopliteal artery critical totalocclusion. Attempted wiring of the infrapopliteal CTO was unsuccessful due totechnical difficulty. Given the complexity of the lesion, a decision was madeto defer further intervention, and a repeat attempt is scheduled in two weeks.
 01.avi
01.avi
01final.avi
Interventional Management
Procedural Step
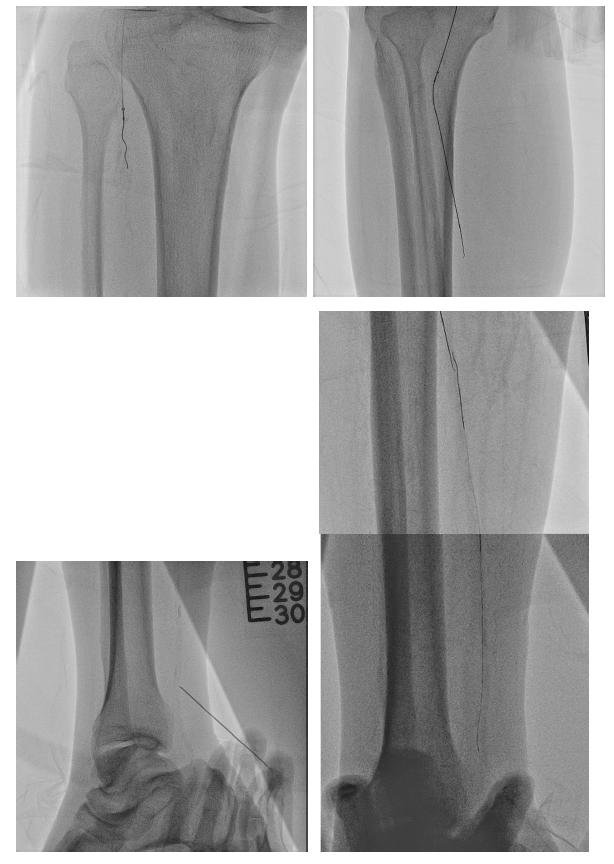
From a right femoral approach to RCFA, we used 0.014" GLADIUS GW with Oscar® multifunctional peripheral catheter initially and changed wire to ASTATO XS40 GW to wiring the infrapopliteal CTO targeting the posterior tibial artery. However, even under strong support of Oscar® multifunctional peripheral catheter, we still could not antegrade wiring through. Therefore, we performed a retrograde puncture to distal posterior tibial artery. We used 0.014" GLADIUS GW with CXI microcatheter and Knuckle technique to retrograde approach proximal posterior tibial artery. Successful rendezvous was achieved, confirming passage through the CTO segment. Balloon passage through the distal PTA lesion was difficult due to tight stenosis. So, several attempts with needle cracking technique on the distal PTA lesion was done, following serial balloon dilatation to PTA. Distal PTA perforation occurred secondary to excessive needle cracking. Several attempted hemostasis were performed following distal PTA perforation but in vain. A covered stent was deployed to seal the distal PTA perforation. Final angiography showed successful revascularization to PTA CTO.


03.avi
04 perforation.avi
05 final.avi
Case Summary
This 75-year-old male patient suffered from chronic limb-threatening ischemia, resulting from proximal RSFA CTO. Successful recanalization of SFA and infrapopliteal CTOs often requires combined antegrade and retrograde wiring techniques. Wire rendezvous and retrograde tip-in are keys to crossing complex occlusions. Balloon passage in distal arteries can be challenging; small coronary balloons and needle cracking may help. Revascularization improves his wound healing and aids limb salvage. Nevertheless, prompt management of complications like arterial perforation with balloon tamponade, heparin reversal, and covered stents is vital