Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_031
Unusual Complication in a TAVR With a Bicuspid Valve, Small Annulus and Heavy Calcium With Baseline LBBB
By Mahesh Shivaji Ahire
Presenter
Mahesh Shivaji Ahire
Authors
Mahesh Shivaji Ahire1
Affiliation
SMBT Heart Institue, India1
View Study Report
CASE20251106_031
Structural - Aortic Valve Intervention - Bicuspid AV
Unusual Complication in a TAVR With a Bicuspid Valve, Small Annulus and Heavy Calcium With Baseline LBBB
Mahesh Shivaji Ahire1
SMBT Heart Institue, India1
Clinical Information
Relevant Clinical History and Physical Exam
Patient History: DM-II, HTN since 5 yrs.Medical complaints: exertional Dyspnea for 1 monthK/C/O CRF- S. Creatinine-2.5mg%, ECG- LBBBDiagnosis: Bicuspid Aortic Valve, small annulus, calcified severe aortic stenosis
Relevant Test Results Prior to Catheterization
CAG S/O MILD PLAQUE IN LM
Relevant Catheterization Findings
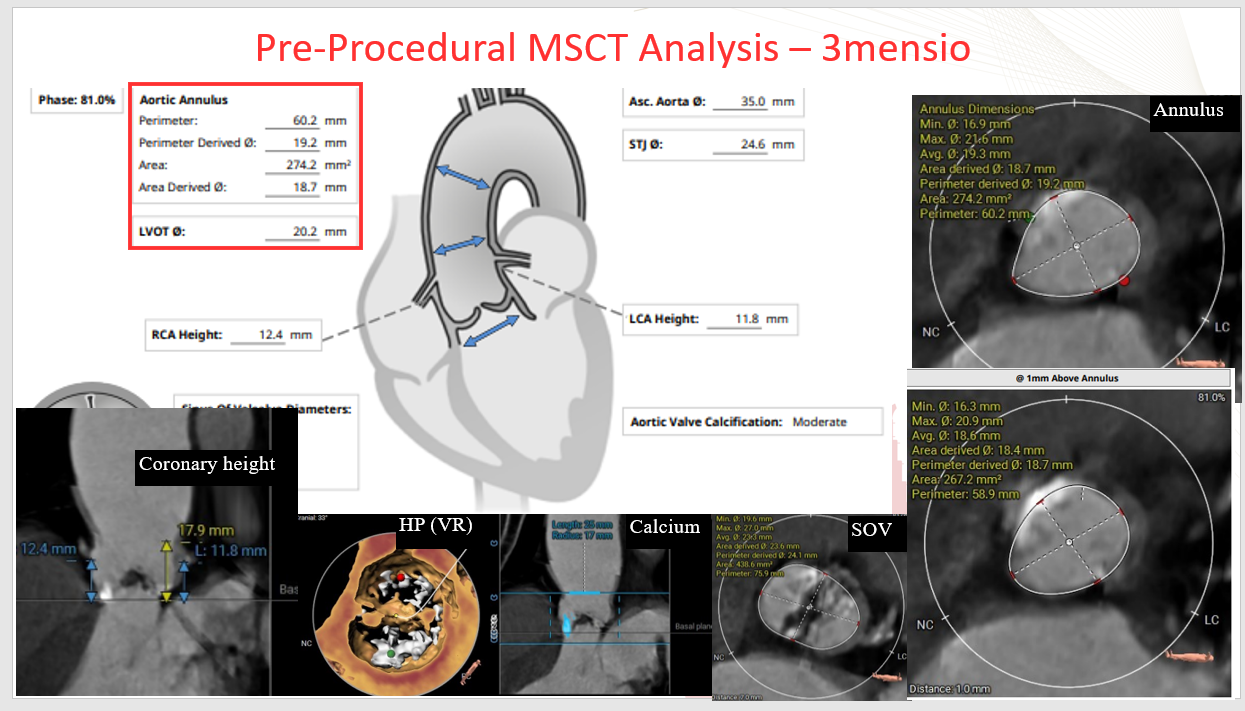
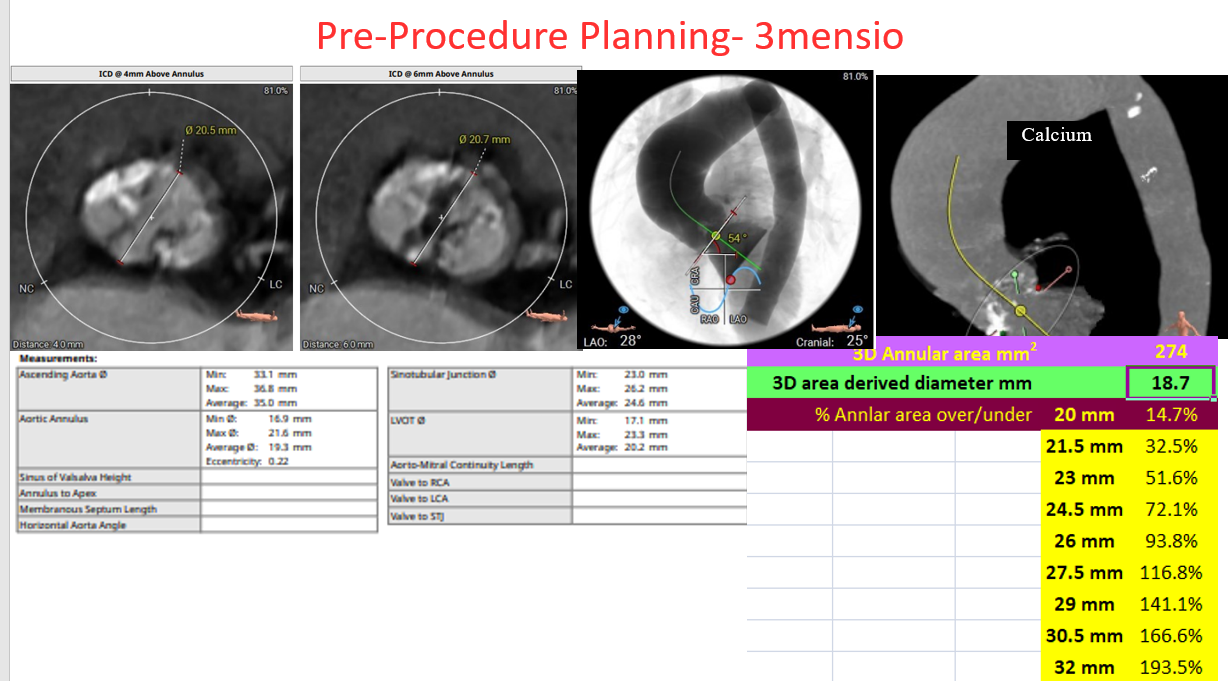
CT S/O RISK FACTORS TO CONSIDER—
OVERALL-
ELDERLY WITH CKD
BASELINE LBBB- NEED FOR PERMANENT PACEMAKER
2. HIGH RISK FOR TAVR-(CHALLENGING FOR THE PROCEDURE)
SMALL ANNULUS
BICUSPID AORTIC VSLVE
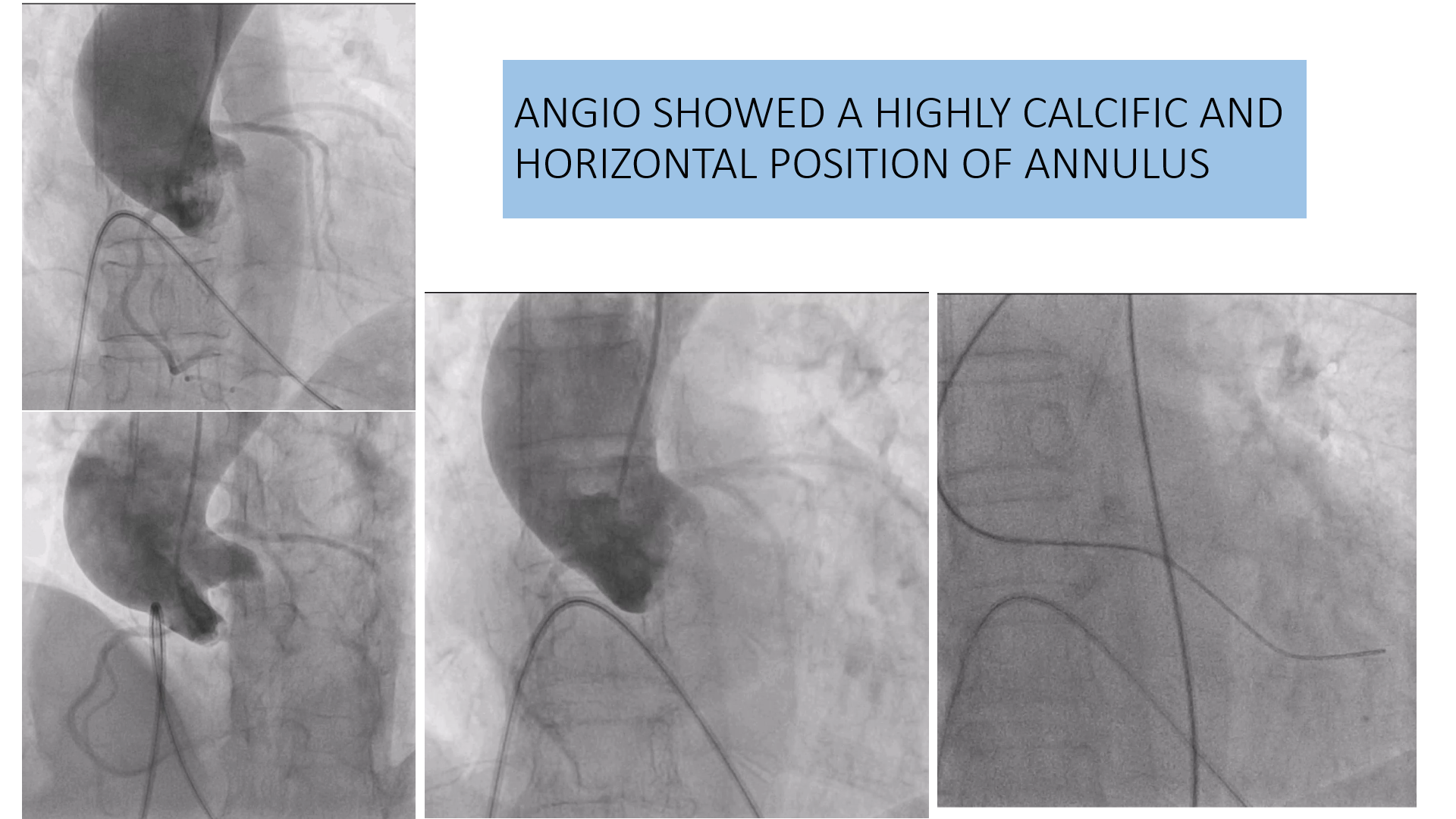
HORIZONTAL AORTA
HEAVY CALCIUM
Interventional Management
Procedural Step
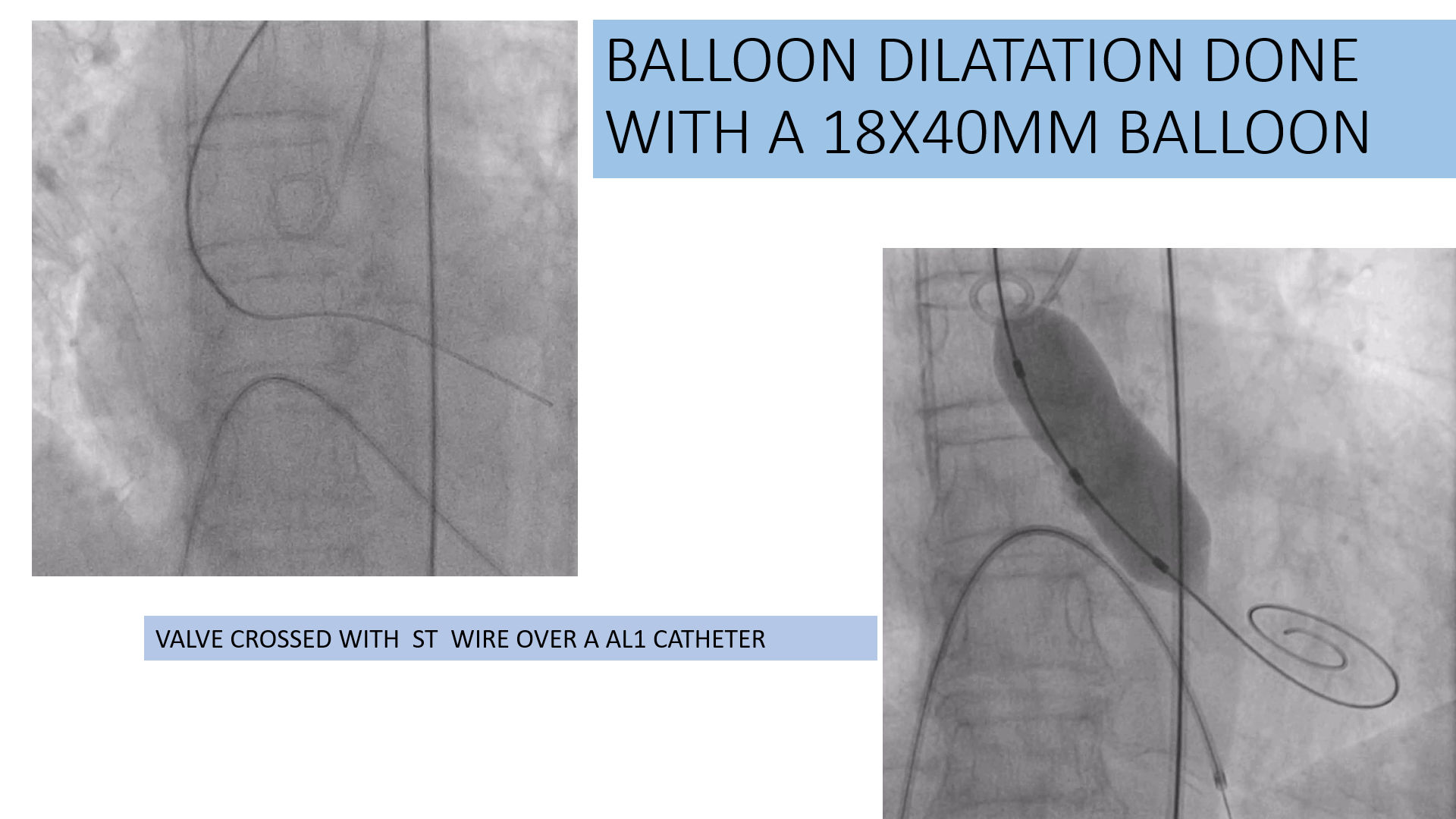
ValveCrossing and Pre-Dilatation: The native valve was crossed using an ST wire overan AL1 support catheter. Prediction: Balloon Dilatation was performed using an18x40 mm balloon.
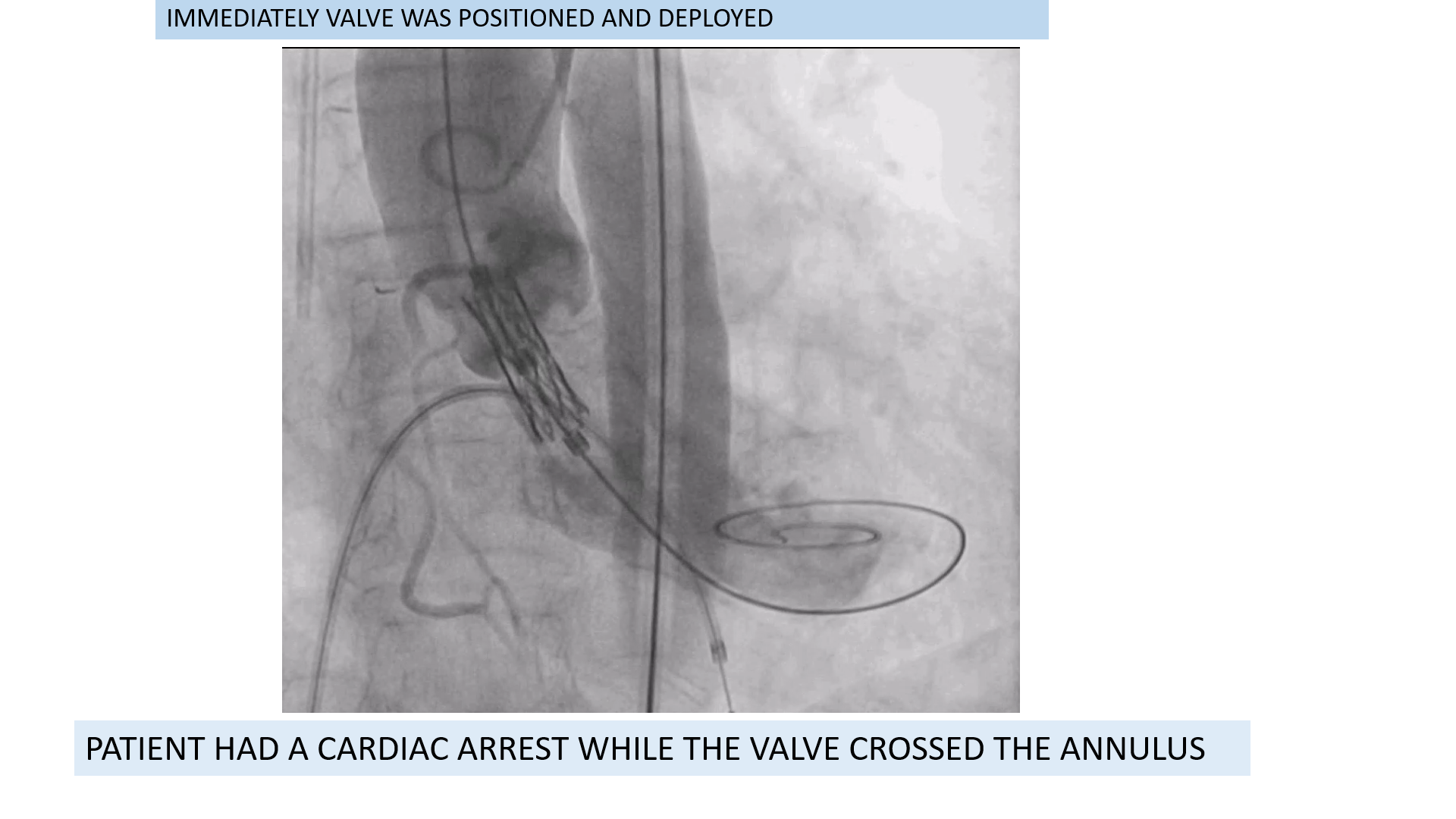
Case Summary
Focus on Technique: Emphasises the need for Gentle Handling of wires and catheters within the delicate cardiac structures, especially the Right Atrium (RA) and Right Ventricle (RV).Risk Acknowledgement: Highlights that Rashness/Overconfidence can lead to potentially Lethal Perforations.Team Readiness: This case demonstrates CPR, cardioversion and immediate availability of Cardiothoracic Surgery for emergency bailout (Heart Team concept).