Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_030
Beyond the Angiogram: Delayed Cardiac Tamponade Caused by Suspected Distal Wire Micro-Perforation After Successful Percutaneous Coronary Intervention
By Kuan-Po Chiu, Zhen Cheng Hwang, Donna Shu-Han Lin, Su-Kiat Chua, Hao-Yun Lo, Yu-Jou Wu
Presenter
Yu-Jou Wu
Authors
Kuan-Po Chiu1, Zhen Cheng Hwang1, Donna Shu-Han Lin1, Su-Kiat Chua1, Hao-Yun Lo1, Yu-Jou Wu2
Affiliation
Division of Cardiology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan2
View Study Report
CASE20251106_030
Coronary - Complication Management
Beyond the Angiogram: Delayed Cardiac Tamponade Caused by Suspected Distal Wire Micro-Perforation After Successful Percutaneous Coronary Intervention
Kuan-Po Chiu1, Zhen Cheng Hwang1, Donna Shu-Han Lin1, Su-Kiat Chua1, Hao-Yun Lo1, Yu-Jou Wu2
Division of Cardiology, Department of Internal Medicine, Shin Kong Wu Ho-Su Memorial Hospital, Taiwan1, Shin Kong Wu Ho-Su Memorial Hospital, Taipei, Taiwan2
Clinical Information
Relevant Clinical History and Physical Exam
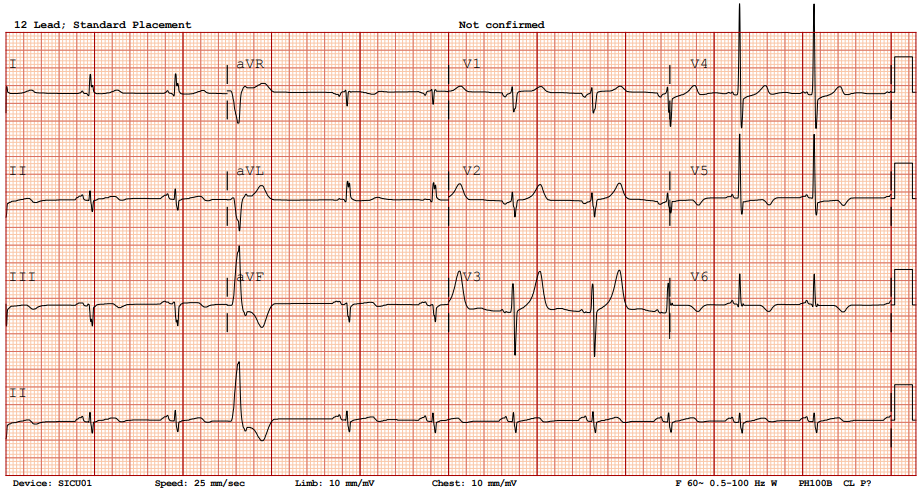
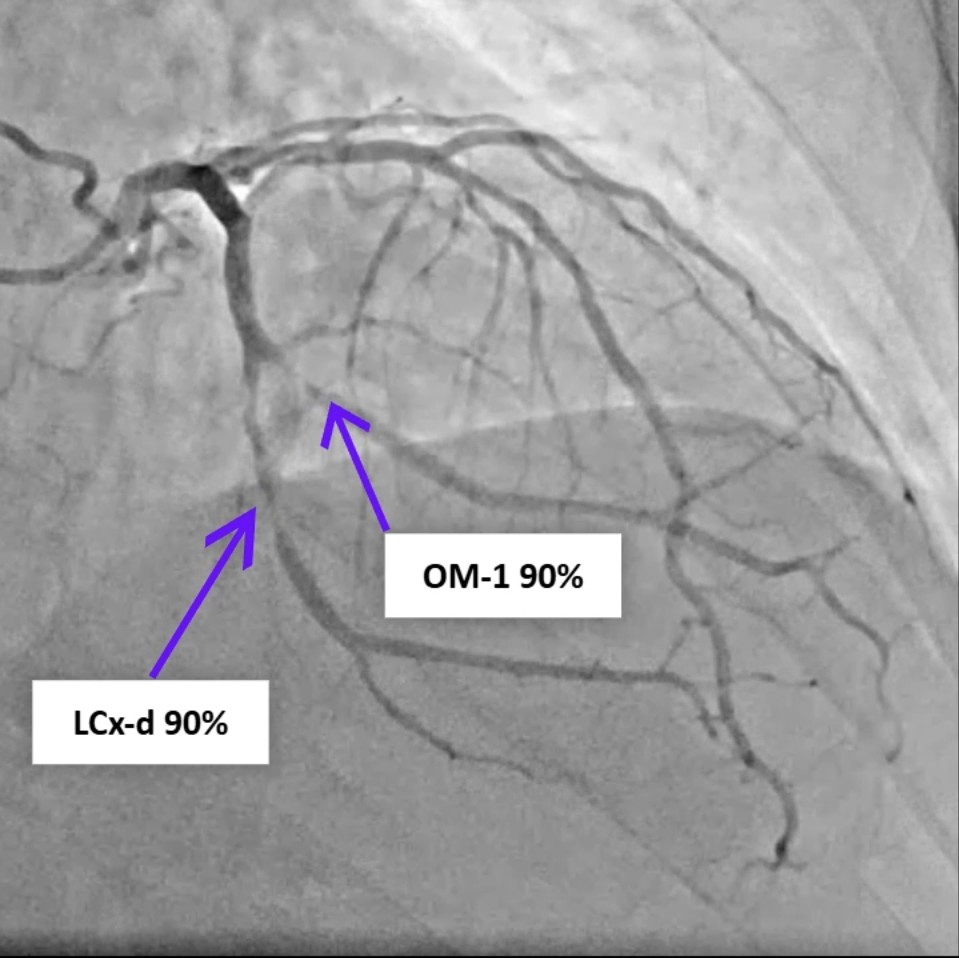
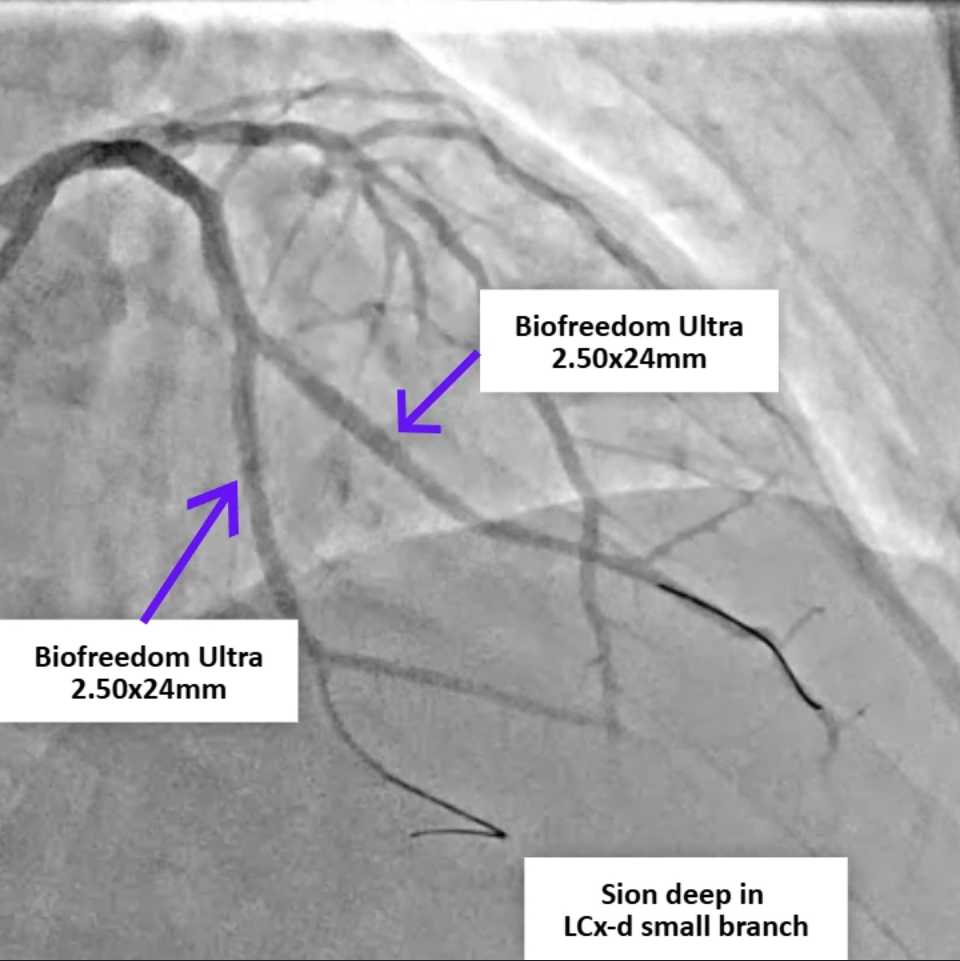
A 77-year-old man with hypertension, diabetes, and prior coronary artery disease presented with progressively typical angina for several days and was diagnosed with non-ST-elevation myocardial infarction. He underwent successful percutaneous coronary intervention with drug-eluting stents to the distal left circumflex and obtuse marginal (OM-1) branch, achieving TIMI-3 flow. Eight hours later, he developed sudden dizziness, diaphoresis, hypotension, and jugular venous distention.
 LCx Pre-PCI.mp4
LCx Pre-PCI.mp4
LCx post.mp4
Relevant Test Results Prior to Catheterization
Arterial blood gas showed no CO₂ retention or hypoxemia, and hemogram revealed no anemia. Serial cardiac enzymes demonstrated a declining trend of Troponin I (12.5→7.9 ng/mL), suggesting no ongoing ischemic progression. Bedside echogram revealed a 1-cm circumferential pericardial effusion with right ventricular diastolic collapse, consistent with cardiac tamponade, but pericardiocentesis was not feasible due to the absence of a safe window. Computed tomography excluded aortic dissection.
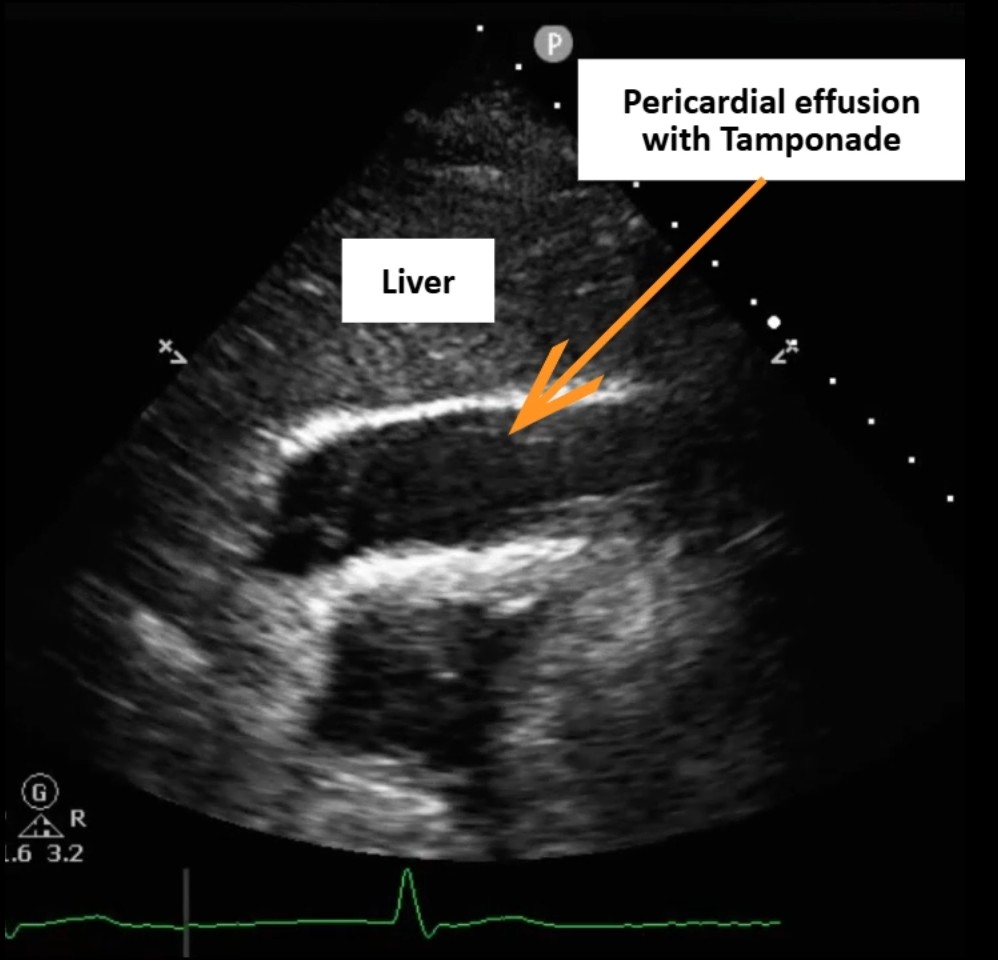
Tamponade PLAX.mp4
Tamponade Subcostal 標示.mp4
Aorta CT.mp4
Relevant Catheterization Findings
Review of the primary PCI angiography revealed no contrast extravasation; however, the Sion wire had advanced deeply into a small distal branch of the LCx artery, in hindsight possibly causing a distal micro-perforation. Repeat angiography demonstrated patent stents in both the left circumflex and obtuse marginal branches without in-stent thrombosis. No persistent or visible extravasation was noted, suggesting spontaneous hemostasis of the suspected micro-perforation.
Recheck LCA.mp4
Recheck LCA cranial view.mp4
Recheck LVG.mp4
Interventional Management
Procedural Step
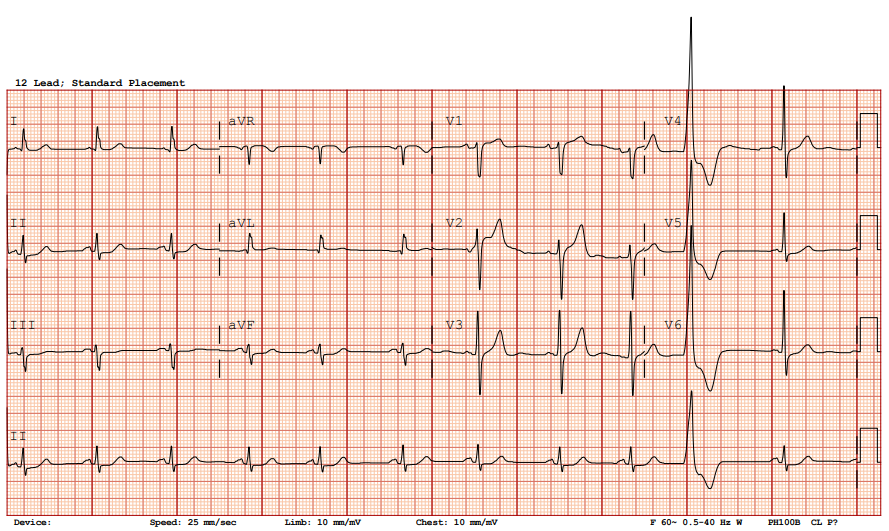
Due to cardiac tamponade with progressing shock, the patient was immediately evaluated for emergency intervention. A cardiovascular surgeon performed an emergent subxiphoid pericardiotomy under local anesthesia. After sterile preparation, a linear incision was made over the xiphoid region and deepened to the pericardium, which was opened bluntly. Approximately 450 mL of fresh blood was evacuated, and a 28 Fr chest tube was inserted for continuous drainage. The patient’s blood pressure rose dramatically from 70 mmHg systolic to over 200 mmHg after decompression, indicating effective relief of tamponade. Once hemodynamic stability was achieved, the interventional cardiology team performed repeat coronary angiography to identify the potential source of bleeding, as detailed in the previous section. The patient was then transferred to the intensive care unit for close monitoring. Chest tube drainage was minimal (0 mL) on postoperative day 2, and follow-up bedside echocardiography revealed no residual pericardial effusion or right ventricular diastolic collapse. The chest tube was subsequently removed, and the patient was transferred back to the general ward for discharge preparation.


Post OP day 2 ECHO.mp4
Post OP day 2 ECHO_2.mp4
Case Summary
We present a case of delayed cardiac tamponade occurring hours after an otherwise successful percutaneous coronary intervention. This case underscores that even in the absence of angiographic contrast extravasation, distal wire micro-perforation may still occur and result in life-threatening pericardial effusion. Clinicians should remain alert to delayed hemodynamic deterioration following PCI, particularly when guidewires are advanced deeply into small distal branches. Although uncommon, coronary perforation during PCI has been reported in approximately 0.2% to 0.6% of cases, including those performed with workhorse guidewires.