Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_027
RVOT Stenting in Adult With Late-Presenter Tetralogy of Fallot and Severe Scoliosis
By Emil Prabowo, Alisia Yuana Putri, Radityo Prakoso
Presenter
Emil Prabowo
Authors
Emil Prabowo1, Alisia Yuana Putri2, Radityo Prakoso2
Affiliation
Department of Cardiology and Vascular Medicine, Faculty of Medicine, Universitas Airlangga, Indonesia1, Division of Pediatric Cardiology and Congenital Heart Disease, Department of Cardiology and Vascular, Indonesia2
View Study Report
CASE20251106_027
Structural - Other Structural Interventions
RVOT Stenting in Adult With Late-Presenter Tetralogy of Fallot and Severe Scoliosis
Emil Prabowo1, Alisia Yuana Putri2, Radityo Prakoso2
Department of Cardiology and Vascular Medicine, Faculty of Medicine, Universitas Airlangga, Indonesia1, Division of Pediatric Cardiology and Congenital Heart Disease, Department of Cardiology and Vascular, Indonesia2
Clinical Information
Relevant Clinical History and Physical Exam
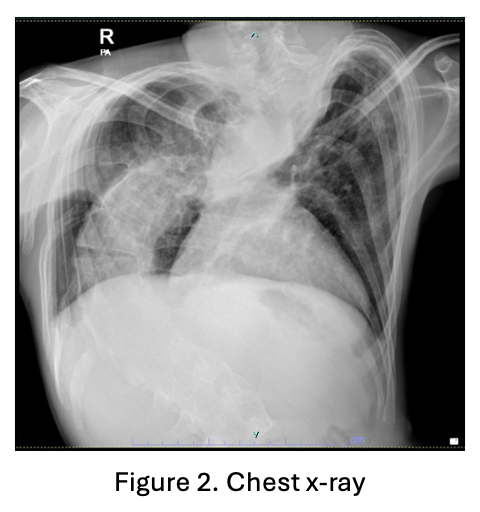
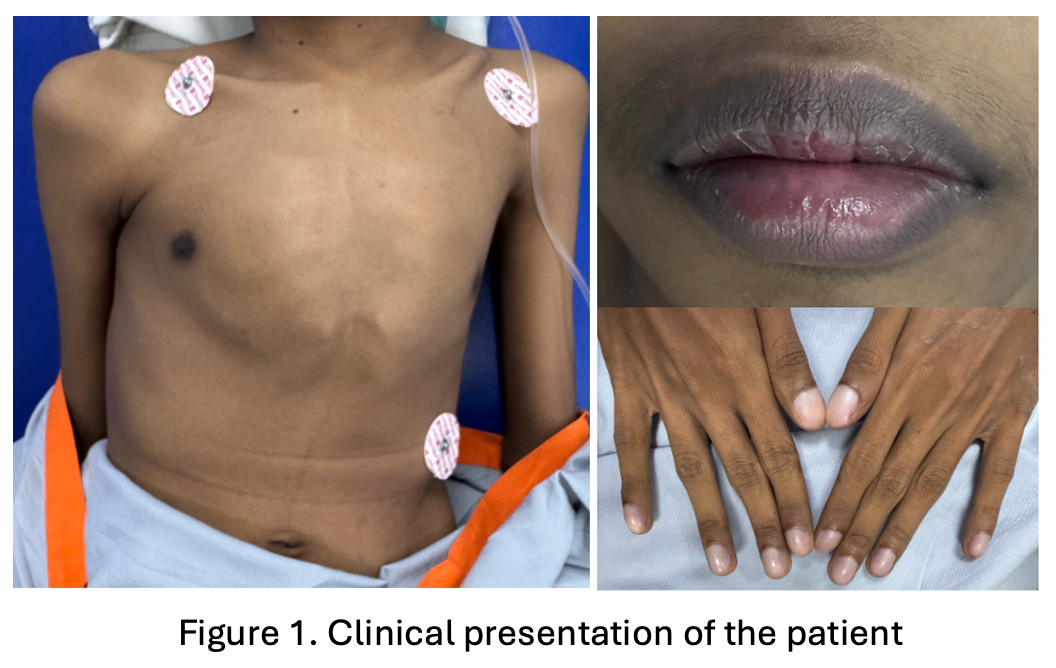
We report a 23-year-old male with pectus carinatum, severe scoliosis, and underweight status (BMI 17.9 kg/m²), referred for recurrent pre-hypoxic spells despite optimal medical management of Tetralogy of Fallot (ToF).
Relevant Test Results Prior to Catheterization
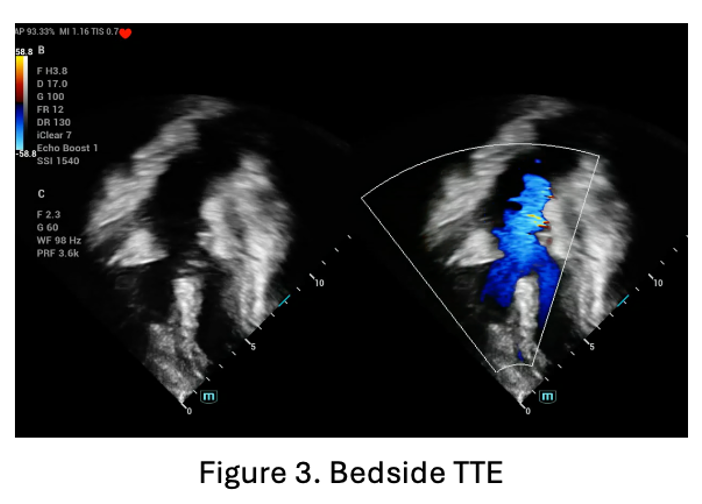
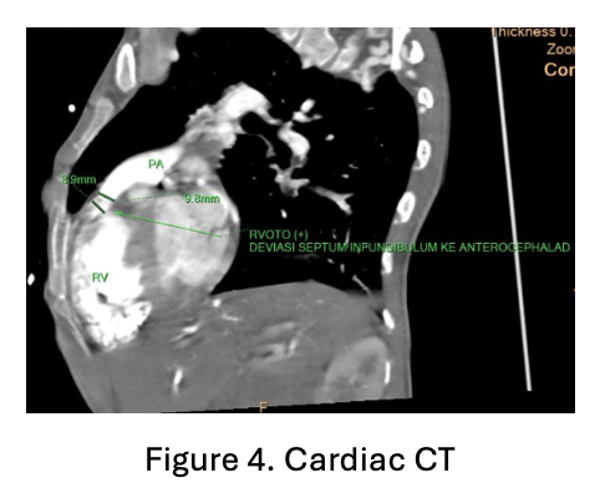
The patient came with lethargic, normal blood pressure and heart rate, increased work of breathing and decreased oxygen saturation into 62% on room air. Laboratory test showed increased hemoglobin and hematocrit into 21.7 mg/dL and 71.3% respectively. Bedside transthoracic echocardiography showed subaortic ventricular septal defect diameter 15-16 mm, right to left shunt, severe narrowing infundibulum, right ventricular outflow tract obstruction, with critical pulmonary stenosis.
Relevant Catheterization Findings
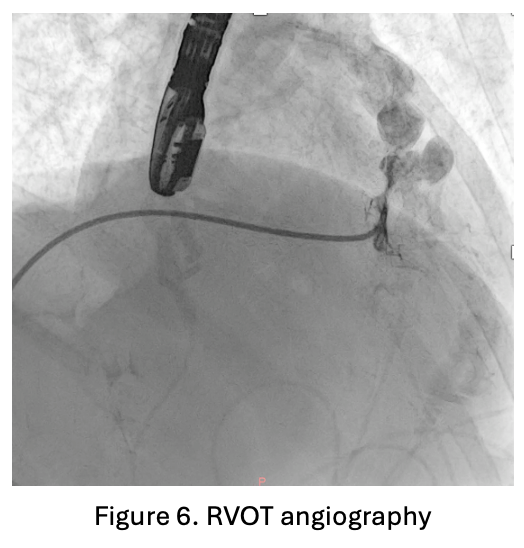
An 8F sheath was inserted into the femoral vein and an arterial line was placed in the femoral artery. Intraoperative transesophageal echocardiography (TOE) showed a very tight right ventricular outflow tract (RVOT) measuring 23.7 mm in length, with a left ventricular ejection fraction (LVEF) of 51.7% by Simpson’s method. RVOT angiography performed using a 3.5/5F Guiding JR catheter confirmed narrowing at the RVOT segment.
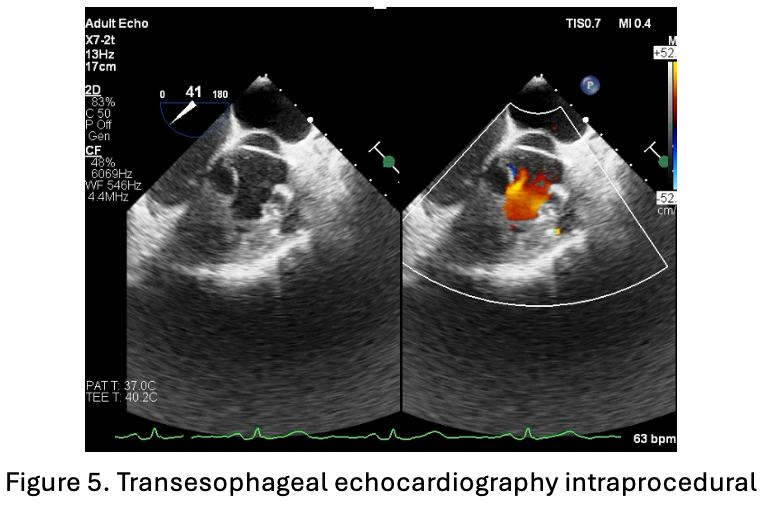
 TOE TOFF.mp4
TOE TOFF.mp4
Graphy RVOT.mp4
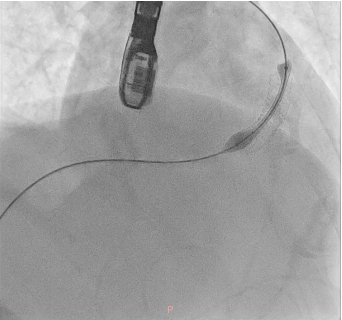
Interventional Management
Procedural Step
A soft hydrophilic 0.035-inch wire was directed into the RVOT, advanced distally to the right pulmonary artery, then exchanged for a super stiff 0.035-inch wire. An Armada vascular balloon 7.0x60 mm was positioned in the RVOT and inflated to 12 atm for ten cycles. An Omnilink vascular stent was deployed in the RVOT and inflated to 12 atm. Due to the patient’s late presentation, a second identical stent was placed at the same location. Following the procedure, LVEF improved to 64.7%, and aortic oxygen saturation increased from 86% to 94%.
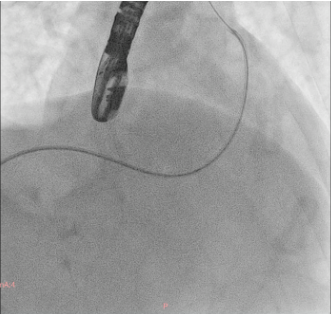
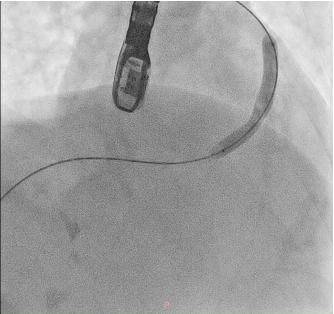
Proced 1.mp4
Proced2.mp4
Case Summary
Patient discharge four days later, increased peripheral oxygen saturation from 84% to 92% room air. Follow up at three months shown significant improvement of the symptom. Transthoracic echocardiography evaluation pre-discharge shown patent flow of the stent, and three month CT follow up shown patent flow of the stent and increased of pulmonary artery size. In conclusion, late-presenting ToF patients face complex risks; RVOT stenting provides effective palliation, improves oxygenation, and bridges to surgery or definitive management.