Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_024
Secundum ASD, Severe PAH and IVUS-Documented Dynamic LMCA Compression — When to Stent, When to Close?
By Steven Wong Poh Hock, Faten Aqilah Aris, Ning Ajleaa Ngah, Hafidz Abd Hadi, Geetha Kandavello, Afif Ashari
Presenter
Steven Wong Poh Hock
Authors
Steven Wong Poh Hock1, Faten Aqilah Aris1, Ning Ajleaa Ngah1, Hafidz Abd Hadi1, Geetha Kandavello1, Afif Ashari1
Affiliation
National Heart Institute, Malaysia1
View Study Report
CASE20251106_024
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Secundum ASD, Severe PAH and IVUS-Documented Dynamic LMCA Compression — When to Stent, When to Close?
Steven Wong Poh Hock1, Faten Aqilah Aris1, Ning Ajleaa Ngah1, Hafidz Abd Hadi1, Geetha Kandavello1, Afif Ashari1
National Heart Institute, Malaysia1
Clinical Information
Relevant Clinical History and Physical Exam
A 55-year-old female with a history of bronchial asthma, dyslipidemia, and an atrial septal defect (ASD) diagnosed in 2005, managed by the Adult Congenital Heart Disease team. She underwent right heart catheterization twice, with the latest Qp:Qs ratio of 0.98 (2015). She has a history of pulmonary artery thrombosis, treated with oral anticoagulants. A recent CTPA showed resolved thrombus and left mainstem stenosis, leading to a planned coronary angiogram.
Relevant Test Results Prior to Catheterization
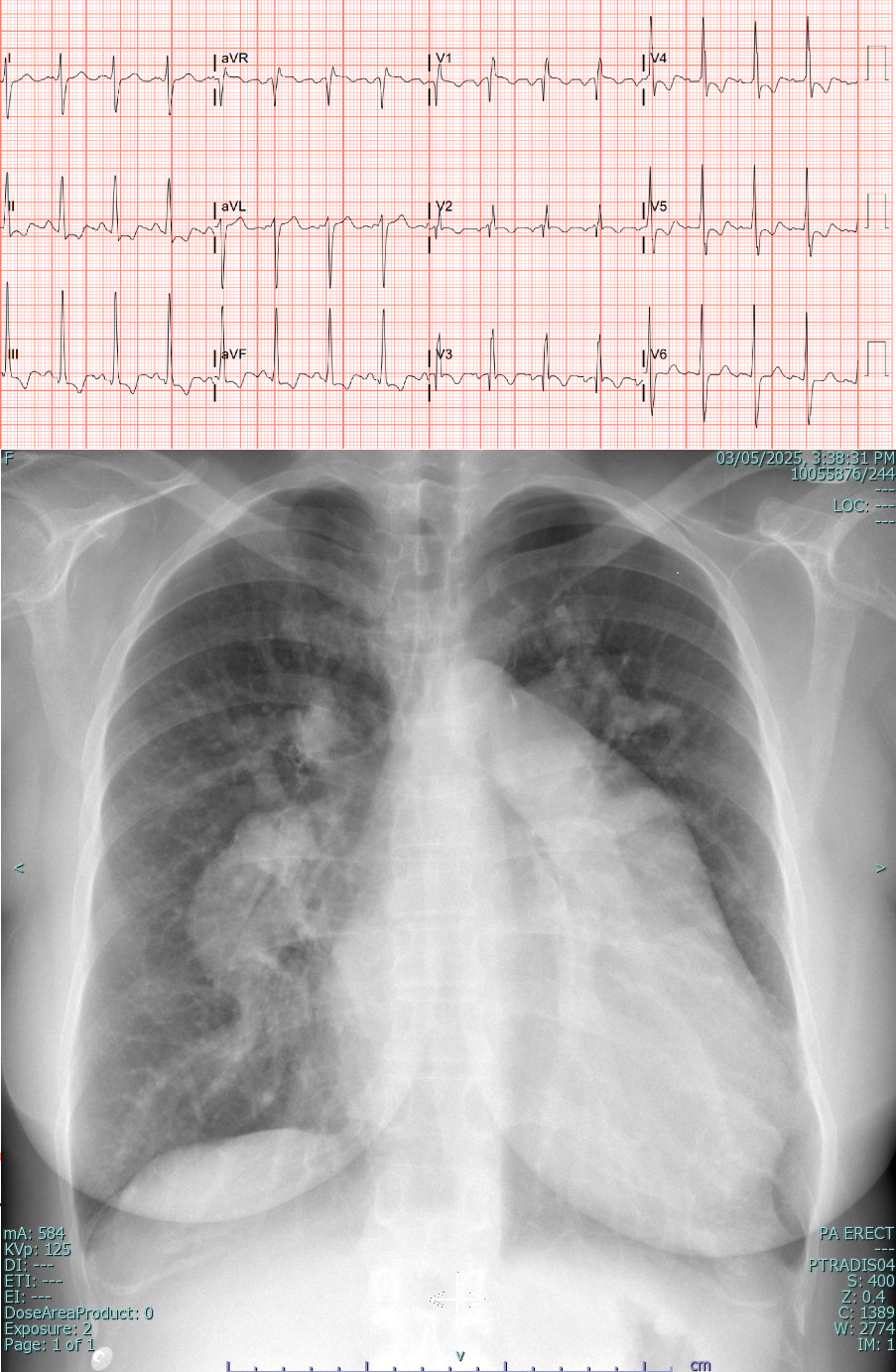
EF 56% (Simpsons),
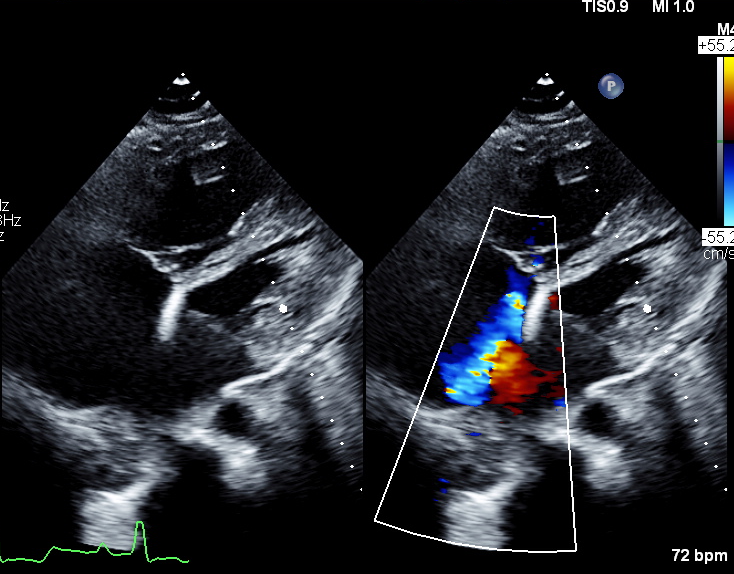
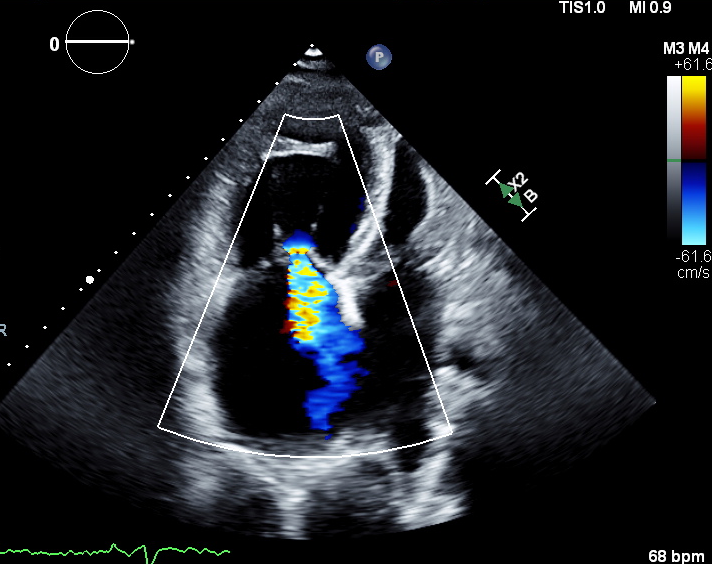
Secundum ASD with bidirectional shunt
Dilated RA and RV
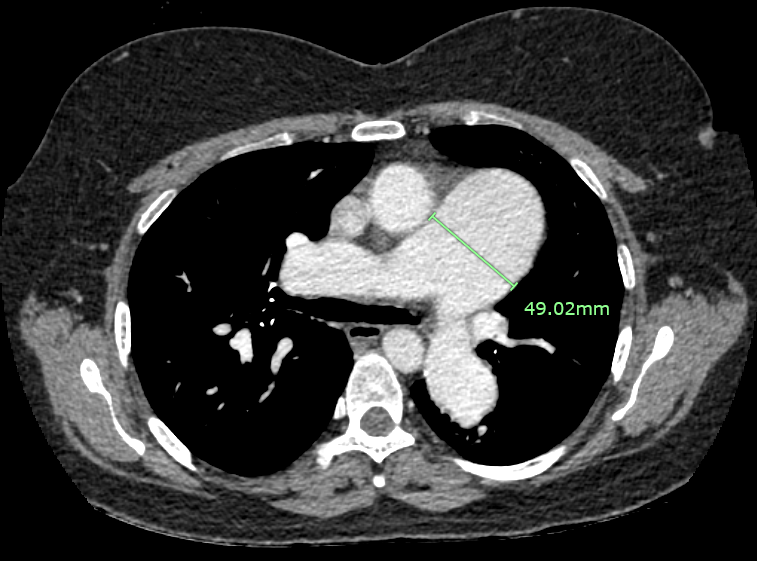
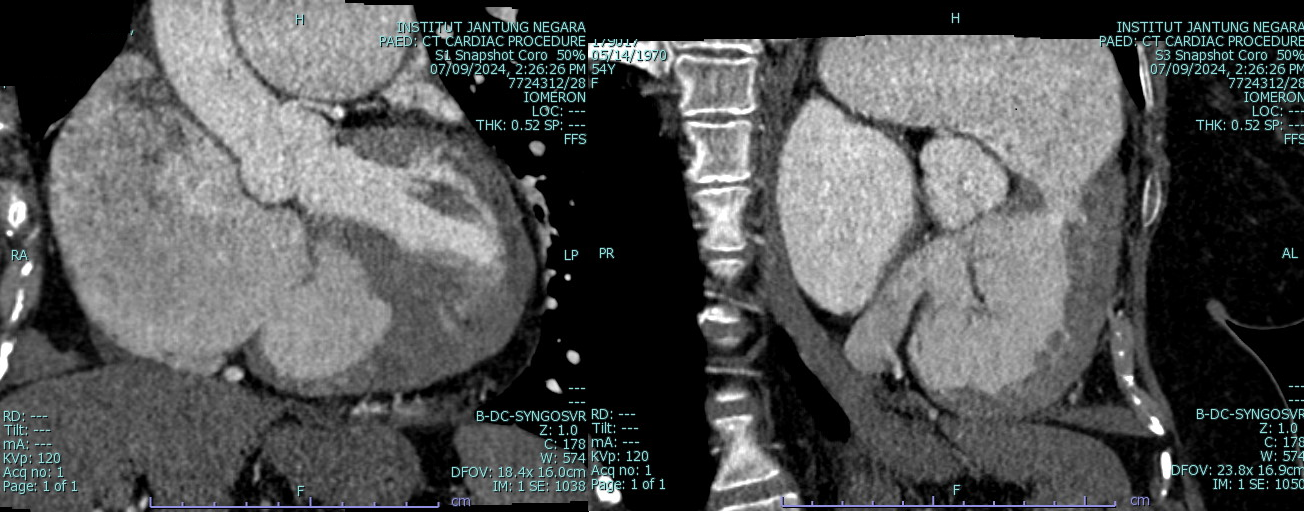
CT scan (CTPA and CT coronary) : Resolved pulmonary artery thrombosis, Normal epicardial coronary arteries.
 RZ echo modified 4c.avi
RZ echo modified 4c.avi
RZ echo a4c.avi
Secundum ASD with bidirectional shunt
Dilated RA and RV
CT scan (CTPA and CT coronary) : Resolved pulmonary artery thrombosis, Normal epicardial coronary arteries.
Relevant Catheterization Findings
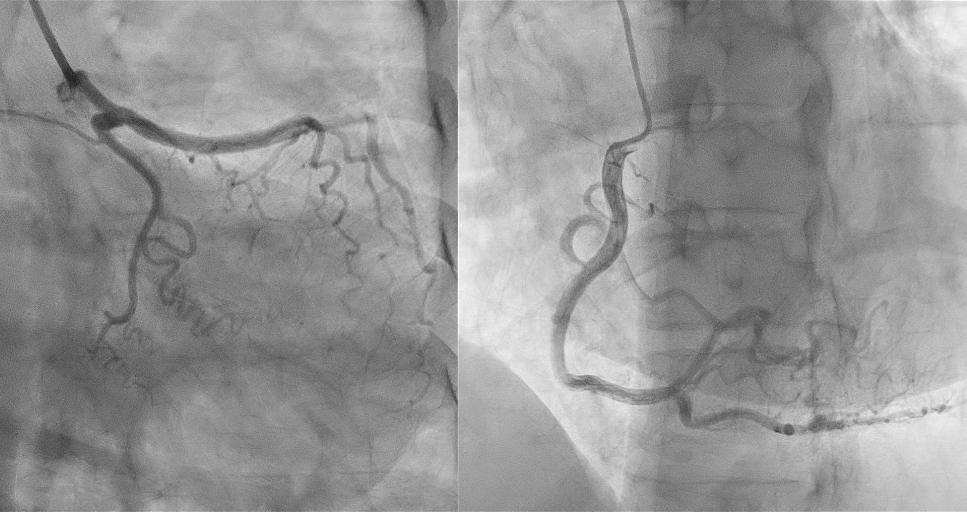
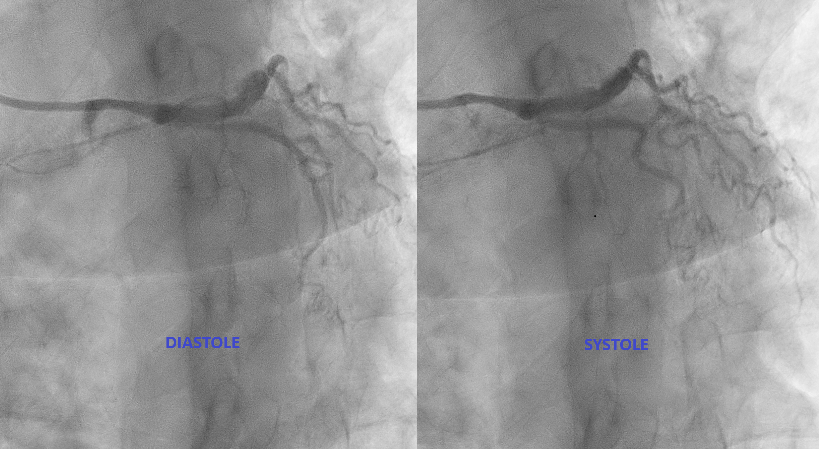
Coronary angiogram via Right radial accessLeft mainstem coronary artery (LMCA) : Moderate Disease 60% TIMI 3
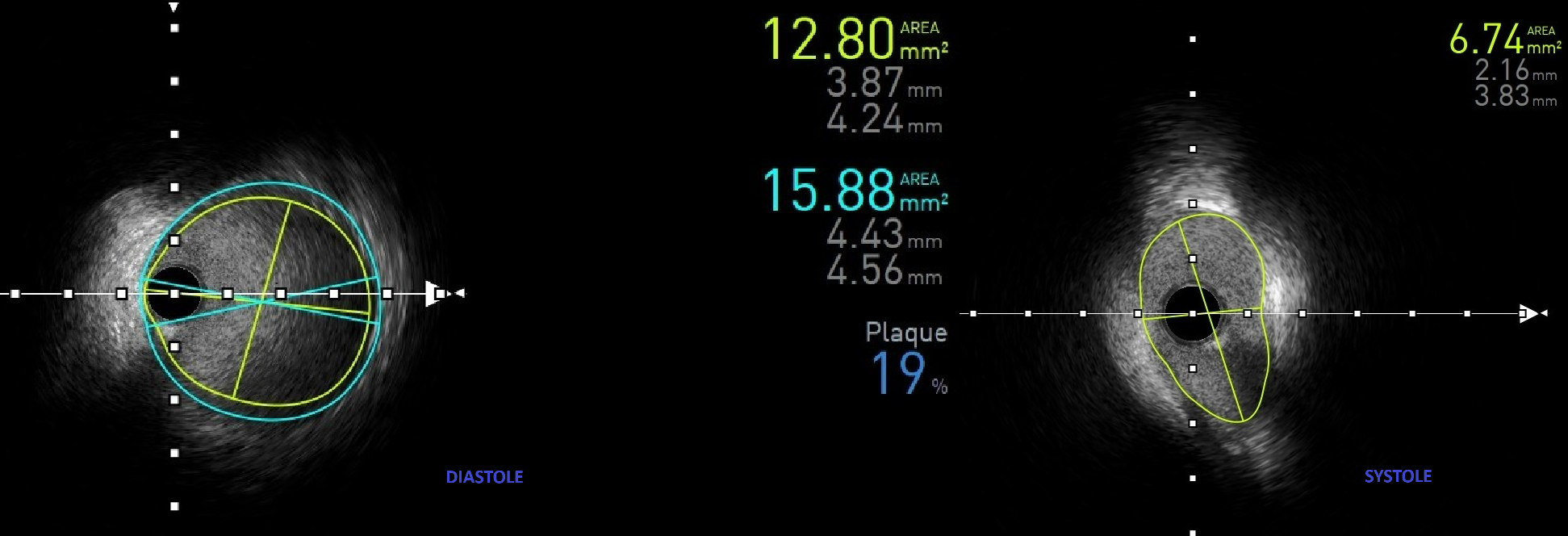
IVUS pullback performed:
Dynamic compression of LMCA externally (MLA reduction by 47.3%, from 12.8 to 6.74 mm2)Minimal intimal plaqueLAD, LCX, RCA was normal.
RZ caudal angio.avi
RZ LMS stenosis spider.avi
RCA normal.avi
IVUS pullback performed:
Dynamic compression of LMCA externally (MLA reduction by 47.3%, from 12.8 to 6.74 mm2)Minimal intimal plaqueLAD, LCX, RCA was normal.
Interventional Management
Procedural Step
Right Heart Catheterization:
Hemodynamic findings:
Pre iNO
- Aorta : 136/70/95
- Right atrium : 12/2/8
- Left atrium : 16/3/8
- Aorta // right ventricle : 129/63/89 // 86 end diastolic pressure 12
- Aorta // pulmonary artery : 127/58/85 // 86/18/48
- Aorta // right pulmonary artery : 123/58/82 // 85/15/45
Post iNO (40ppm, 15min, O2 1L/min)
- Aorta // pulmonary artery: 125/64/86 // 78/10/44
- Aorta // right ventricle: 131/71/92 // 80 EDP 7
- Right atrium: 16/8/12
- Left atrium : 21/6/13
- Left ventricle 140 end diastolic pressure 15
- Pullback left ventricle – aorta : 132 end diastolic pressure 14 – 130/79/91
- Last aorta : 134/72/95
Pre - Post iNO
- Qp QS : 1.66 – 1.29
- Pulmonary vascular resistance : 4.9 – 3.78
- Pulmonary vascular resistance index : 8.55 - 6.59
- SVT : 16.20 – 11.64
- Systemic vascular resistance index : 28.37 – 20.30
- Pulmonary vascular resistance / systemic vascular resistance : 0.30 – 0.32
- Fick cardiac output : 4.55 – 6.36
- Fick cardiac index : 2.61 – 3.65
- SV : 48.92 – 68.4
- SVi : 28.06 – 39.2
Oxygen saturation
- Pre - Post iNO
- Superior vena cava : 67 – 80
- Inferior vena cava : 79 -88
- Right atrium : 81 – 88
- Right ventricle : 83 -90
- MPA : 82 – 89
- Aorta : 95 – 99
- Left atrium : 95 – 98
Conclusion:
- Atrial septal defect secundum with pulmonary hypertension
-Vasoreactivity results may be skewed with O2-Severe tricuspid regurgitation due to prolapsed anterior leaflet and retracted septal leaflet

Hemodynamic findings:
Pre iNO
- Aorta : 136/70/95
- Right atrium : 12/2/8
- Left atrium : 16/3/8
- Aorta // right ventricle : 129/63/89 // 86 end diastolic pressure 12
- Aorta // pulmonary artery : 127/58/85 // 86/18/48
- Aorta // right pulmonary artery : 123/58/82 // 85/15/45
Post iNO (40ppm, 15min, O2 1L/min)
- Aorta // pulmonary artery: 125/64/86 // 78/10/44
- Aorta // right ventricle: 131/71/92 // 80 EDP 7
- Right atrium: 16/8/12
- Left atrium : 21/6/13
- Left ventricle 140 end diastolic pressure 15
- Pullback left ventricle – aorta : 132 end diastolic pressure 14 – 130/79/91
- Last aorta : 134/72/95
Pre - Post iNO
- Qp QS : 1.66 – 1.29
- Pulmonary vascular resistance : 4.9 – 3.78
- Pulmonary vascular resistance index : 8.55 - 6.59
- SVT : 16.20 – 11.64
- Systemic vascular resistance index : 28.37 – 20.30
- Pulmonary vascular resistance / systemic vascular resistance : 0.30 – 0.32
- Fick cardiac output : 4.55 – 6.36
- Fick cardiac index : 2.61 – 3.65
- SV : 48.92 – 68.4
- SVi : 28.06 – 39.2
Oxygen saturation
- Pre - Post iNO
- Superior vena cava : 67 – 80
- Inferior vena cava : 79 -88
- Right atrium : 81 – 88
- Right ventricle : 83 -90
- MPA : 82 – 89
- Aorta : 95 – 99
- Left atrium : 95 – 98
Conclusion:
- Atrial septal defect secundum with pulmonary hypertension
-Vasoreactivity results may be skewed with O2-Severe tricuspid regurgitation due to prolapsed anterior leaflet and retracted septal leaflet
Case Summary
This case highlights our patient with longstanding secundum ASD and pulmonary arterial hypertension who developed dynamic left main coronary compression by a dilated pulmonary artery, confirmed on IVUS (MLA 12.8→6.7 mm², minimal plaque). Cardiac MRI showed Qp:Qs 1.86 and right-sided dilatation; right-heart catheterization revealed elevated but partially reversible PVR (4.9→3.8 WU with iNO). A multidisciplinary, safety-first “treat-and-reassess” strategy (targeted PAH therapy with planned fenestrated ASD closure if PVR improves) avoided premature high-risk interventions and provides a practical framework for similar complex ACHD patients.