Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_021
Unmasking the Invisible: Real-Time IVUS and Contralateral Injection for Precise PDA Recanalization
By Yi-Chun Huang, Chao-Yung Wang, Ming-Yun Ho, Yu-Ying Lu, Chun-Chi Chen
Presenter
Yi-Chun Huang
Authors
Yi-Chun Huang1, Chao-Yung Wang1, Ming-Yun Ho1, Yu-Ying Lu1, Chun-Chi Chen1
Affiliation
Chang Gung Memorial Hospital, Linkou, Taiwan1
View Study Report
CASE20251106_021
Coronary - Imaging & Physiology - Invasive Imaging (IVUS, OCT, NIRS, VH, etc)
Unmasking the Invisible: Real-Time IVUS and Contralateral Injection for Precise PDA Recanalization
Yi-Chun Huang1, Chao-Yung Wang1, Ming-Yun Ho1, Yu-Ying Lu1, Chun-Chi Chen1
Chang Gung Memorial Hospital, Linkou, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 62-year-old female with a historyof hypertension presented at 07:00 on November 1, 2025, with typical chest discomfort.She denied a history of diabetes mellitus, dyslipidemia, smoking,alcohol consumption, or any family history ofcardiovascular disease. Physical examination was unremarkable
Relevant Test Results Prior to Catheterization
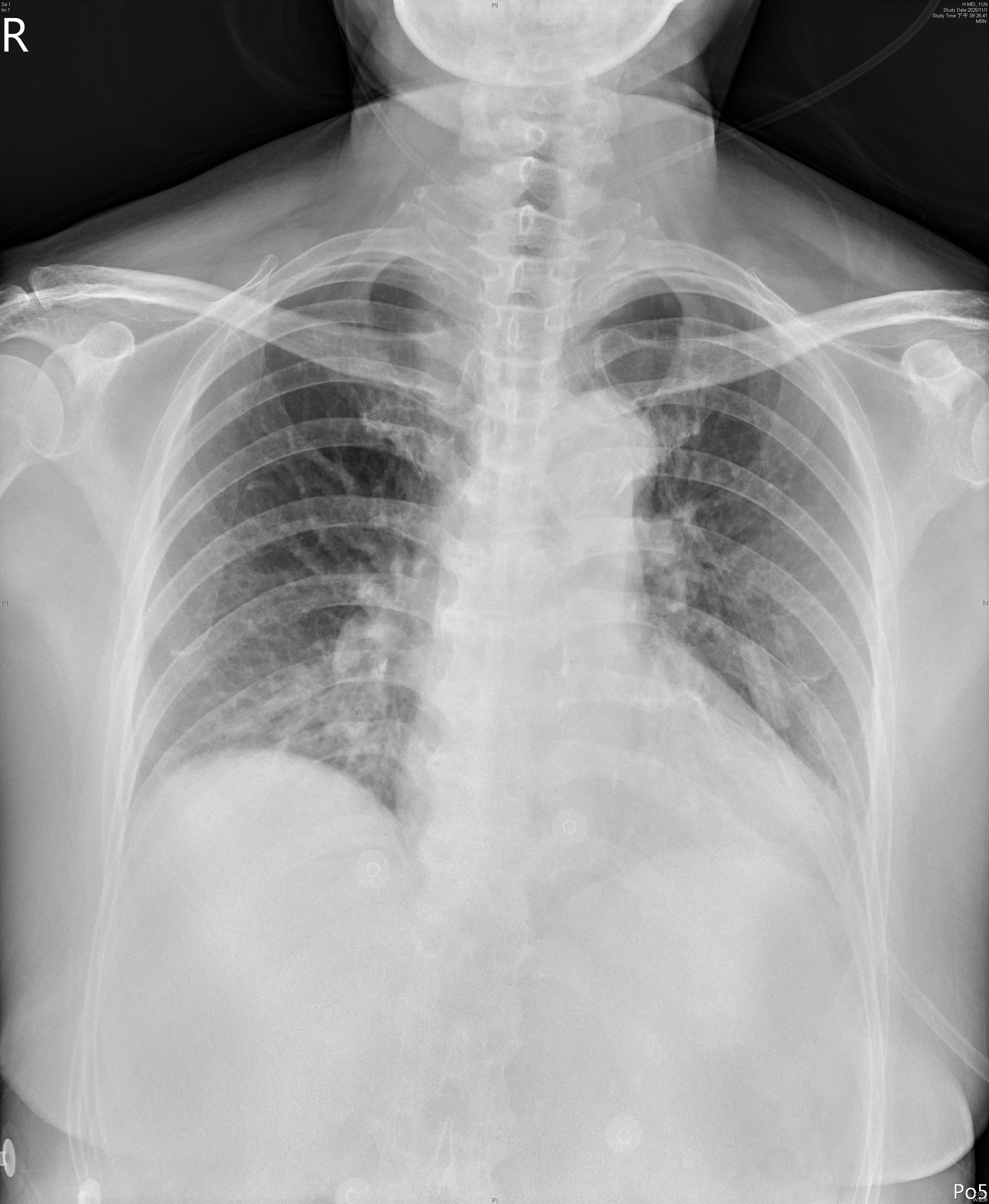
Electrocardiogramdemonstrated ST elevation in leads II, III, and aVF, with Q waves in lead III,indicating acute inferior myocardial infarction. Chestradiographshowed borderline cardiomegaly and mild pulmonary congestion
Relevant Catheterization Findings
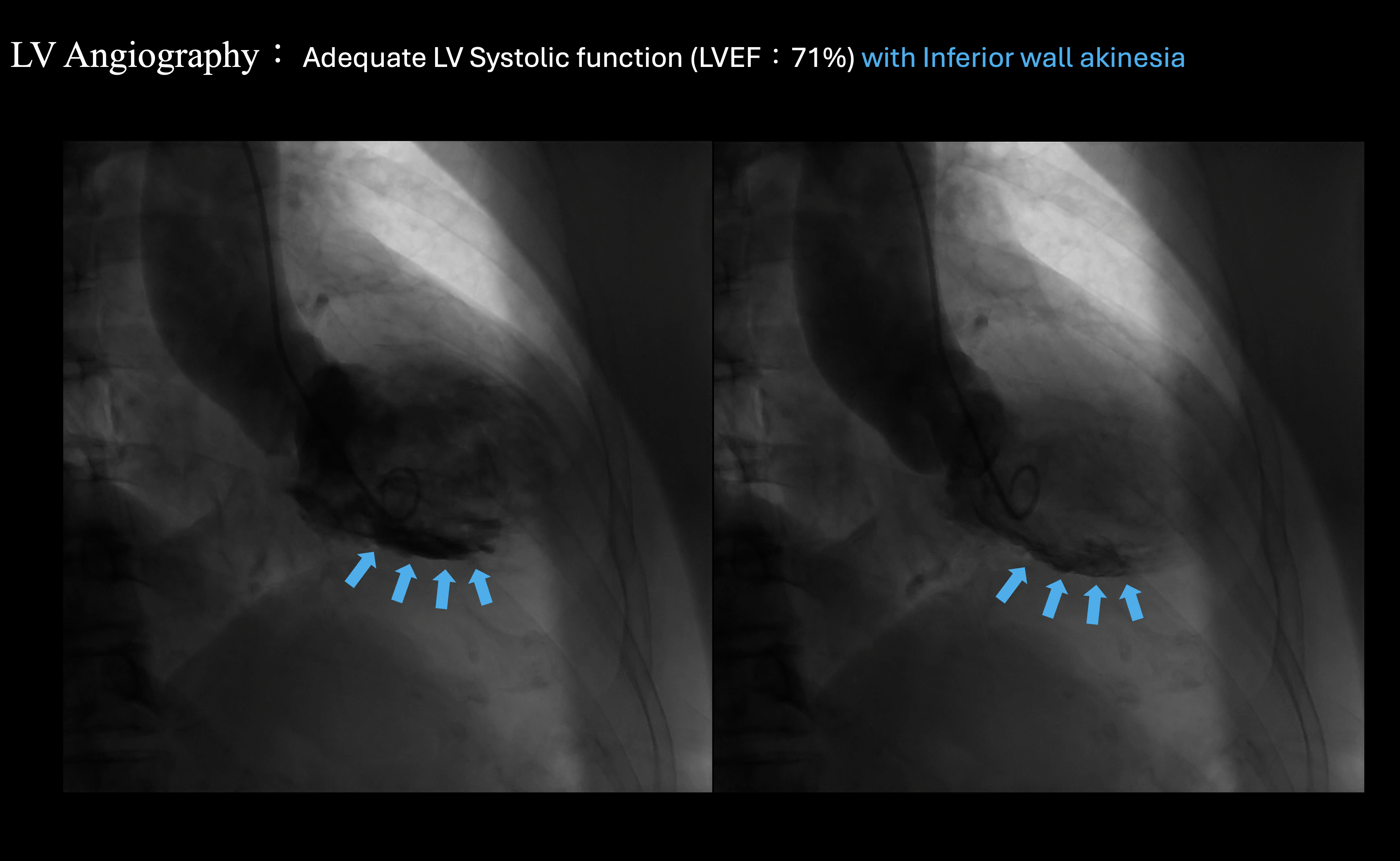
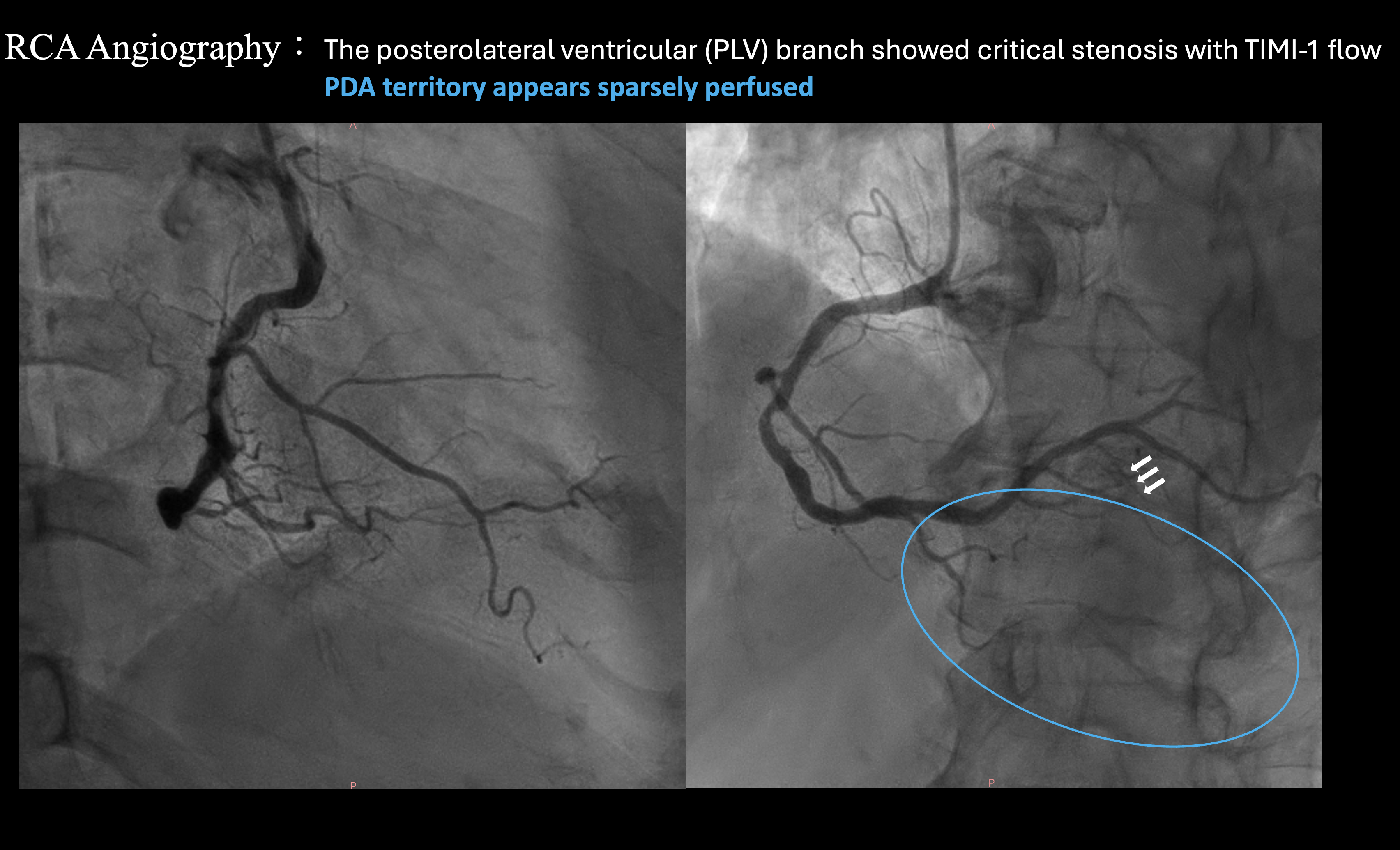
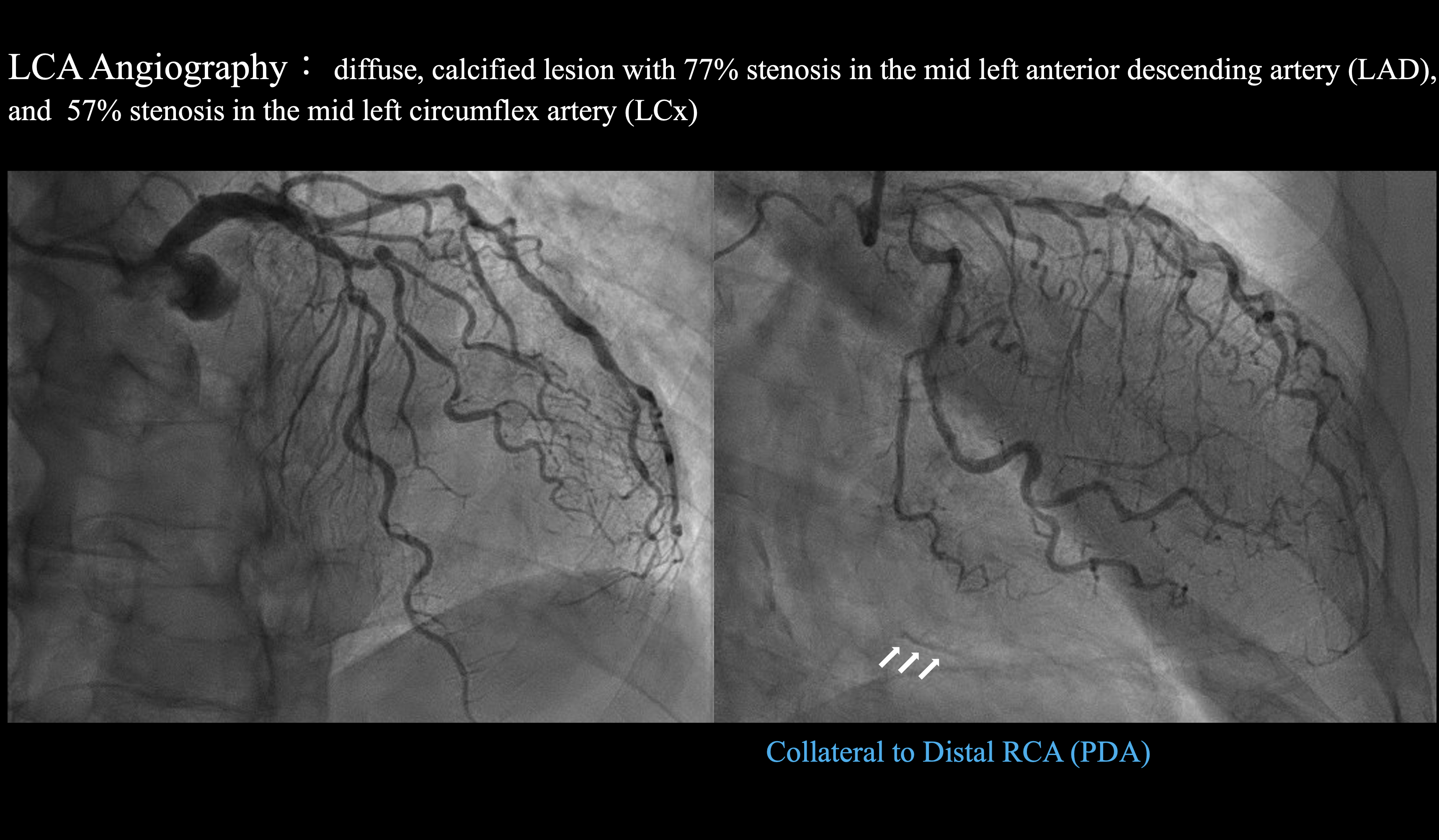
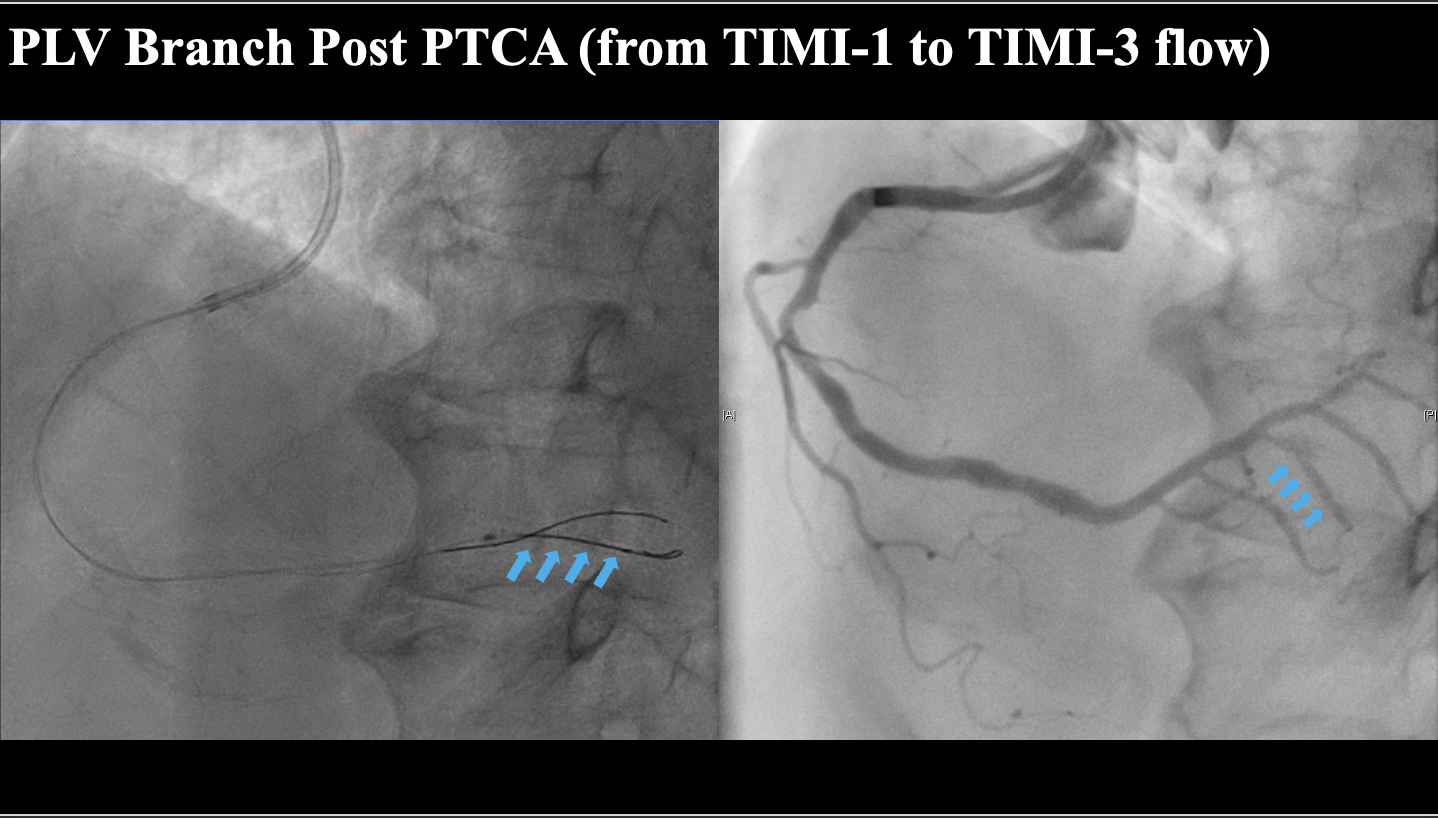
Coronaryangiography revealed a diffuse, calcified lesion with 77% stenosis in the midleft anterior descending artery (LAD), and 57% stenosis in the mid leftcircumflex artery (LCx). Theposterolateral ventricular (PLV) branch showed critical stenosis with TIMI-1flow. Collateral circulation from the left coronary artery (LCA) to the distalright coronary artery (RCA) segment or posterior descending artery (PDA)was faintlyvisible
 LCA angiography with collateral.mp4
LCA angiography with collateral.mp4
RCA angiography.mp4
LV angiography.mp4
Interventional Management
Procedural Step
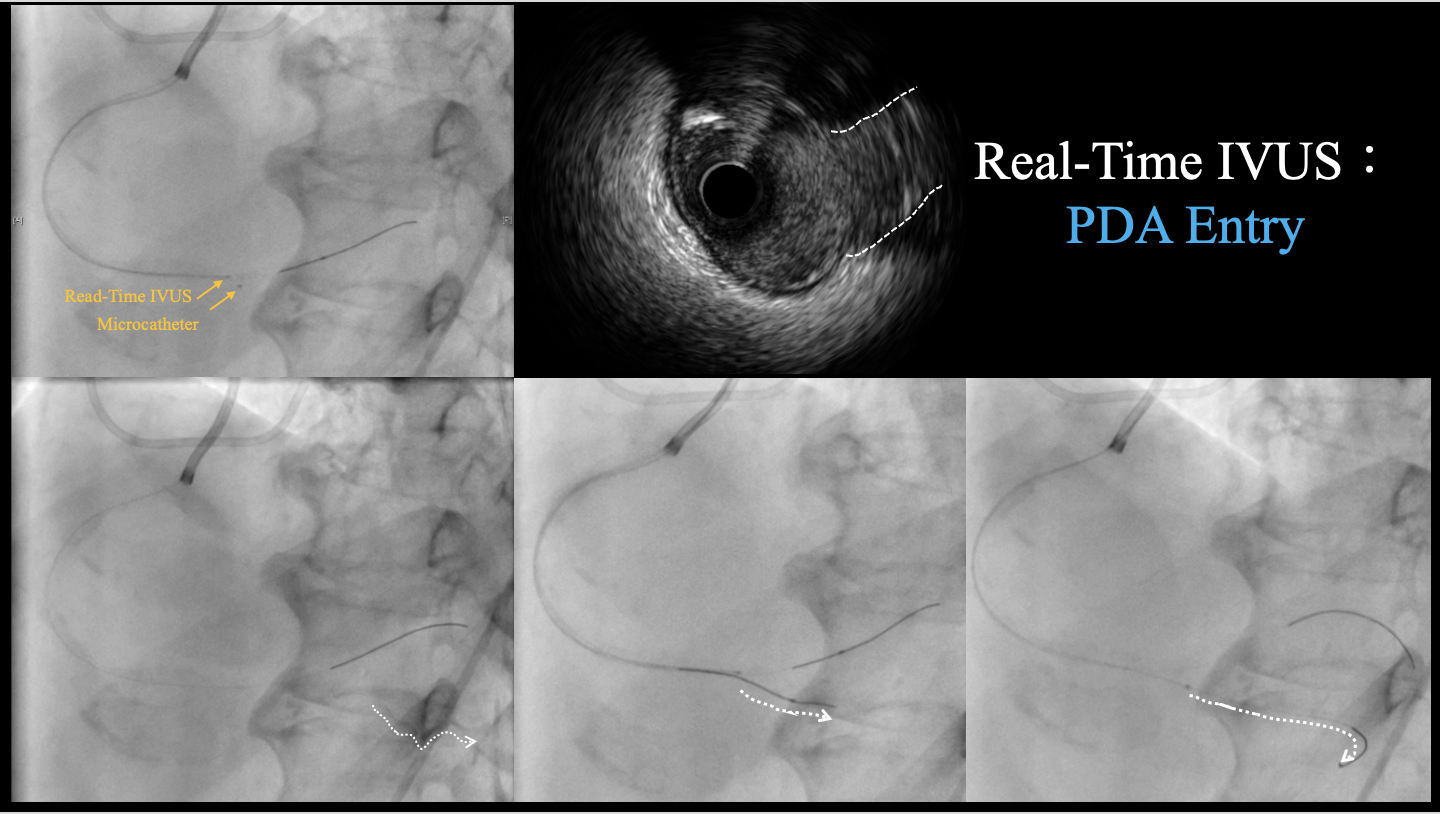
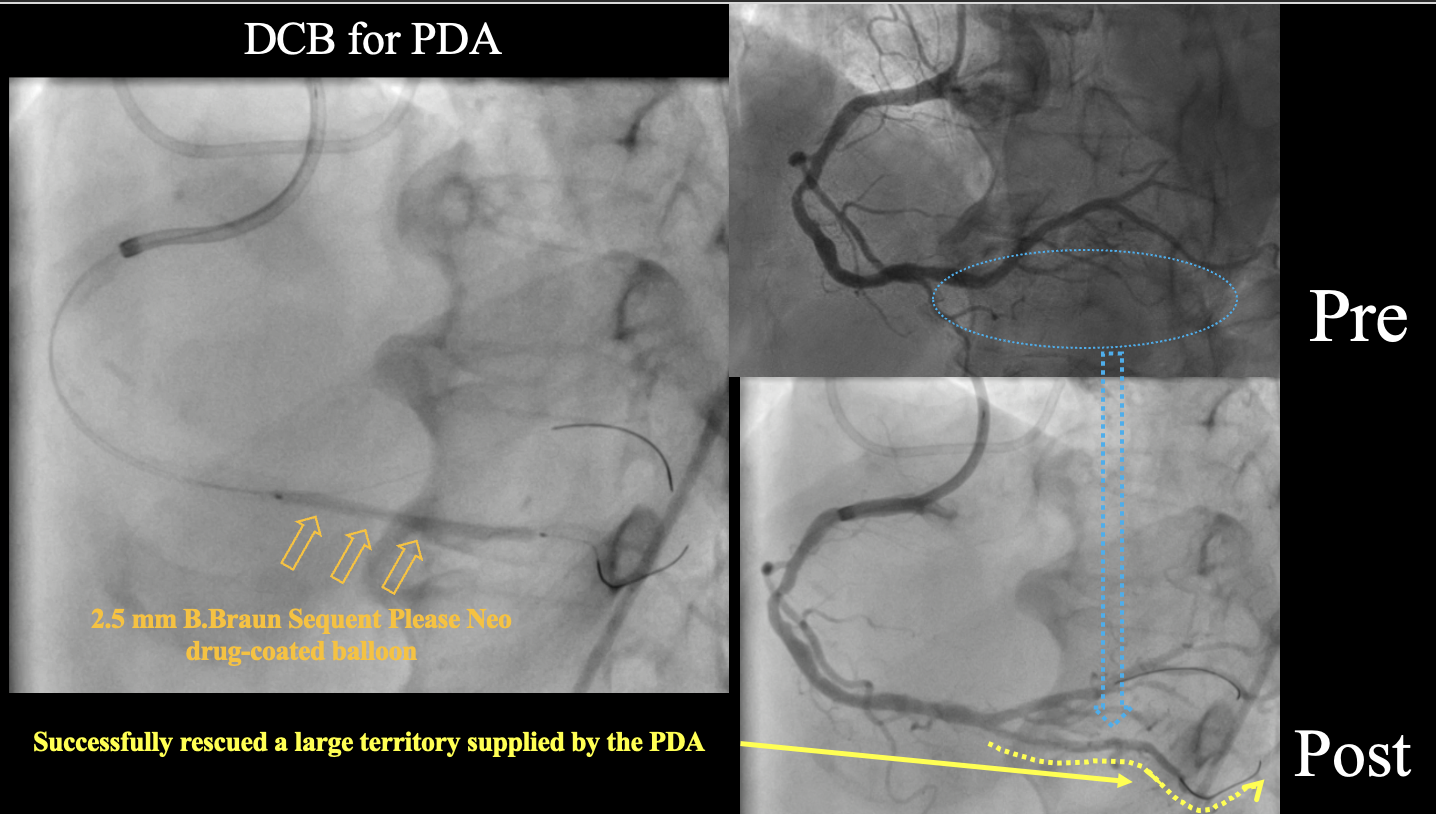
Dualaccess via right radial and right femoral arteries was established. A 7Fr SAL1.0 guiding catheter was used for the RCA, and a diagnostic catheter forcontralateral injection of the LCA. Based on ECG and clinical findings, initialpercutaneous transluminal coronary angioplasty (PTCA) was performed on the PLVbranch using a 2.0 mm semi-compliant balloon, restoring TIMI-3 flow.Despiteexhaustive review of the RCA angiogram, the PDA ostium remained elusive. Toaddress this, a real-time intravascular ultrasound (IVUS)-guided technique wasemployed to systematically identify all side branches, ultimately pinpointingthe PDA ostium with precision. A Finecross microcatheter and UB3 guidewire wereused to create an entry into the PDA, overcoming mild resistance. The UB3guidewire successfully established the entry, and a runthrough guidewire wasadvanced through the chronic total occlusion (CTO) lesion.Serialballoon dilations were performed with 2.0 mm and 2.5 mm semi-compliantballoons. IVUS assessment indicated vessel diameter between 2.0–2.5 mm. A 2.5mm B.Braun Sequent Please Neo drug-coated balloon was used to treat the targetlesion, resulting in an excellent angiographic outcome.
Real-time IVUS.mp4
Real time IVUS.wiring.mp4
RCA-Final angiography.mp4
Case Summary
Thiscase highlights the importance of identifying and treating the often-overlookedPDA in inferior STEMI. Conventional angiography may miss subtle lesions, butcontralateral angiography for collateral from the LCA and real-time IVUSguidance provide crucial clues and definitive localization. Though technicallystraightforward, this case underscores the need for careful assessment ofcoronary anatomy and the wise use of available tools. Real-time IVUS improvessafety and efficacy, and helps clinicians address challenging lesions. Overall,this case is an instructive example with ongoing educational value forinterventional cardiologists.