Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_020
Not Every Medina 1.1.1 True Bifurcation Lesion Needs Two Stents: OCT-Optimized Provisional DES Stenting With RFR-Guided Side Branch DCB
By Liwei Su, Chon-Seng Hong
Presenter
Liwei Su
Authors
Liwei Su1, Chon-Seng Hong1
Affiliation
Chi Mei Medical Center, Taiwan1
View Study Report
CASE20251106_020
Coronary - Complex PCI - Bifurcation
Not Every Medina 1.1.1 True Bifurcation Lesion Needs Two Stents: OCT-Optimized Provisional DES Stenting With RFR-Guided Side Branch DCB
Liwei Su1, Chon-Seng Hong1
Chi Mei Medical Center, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
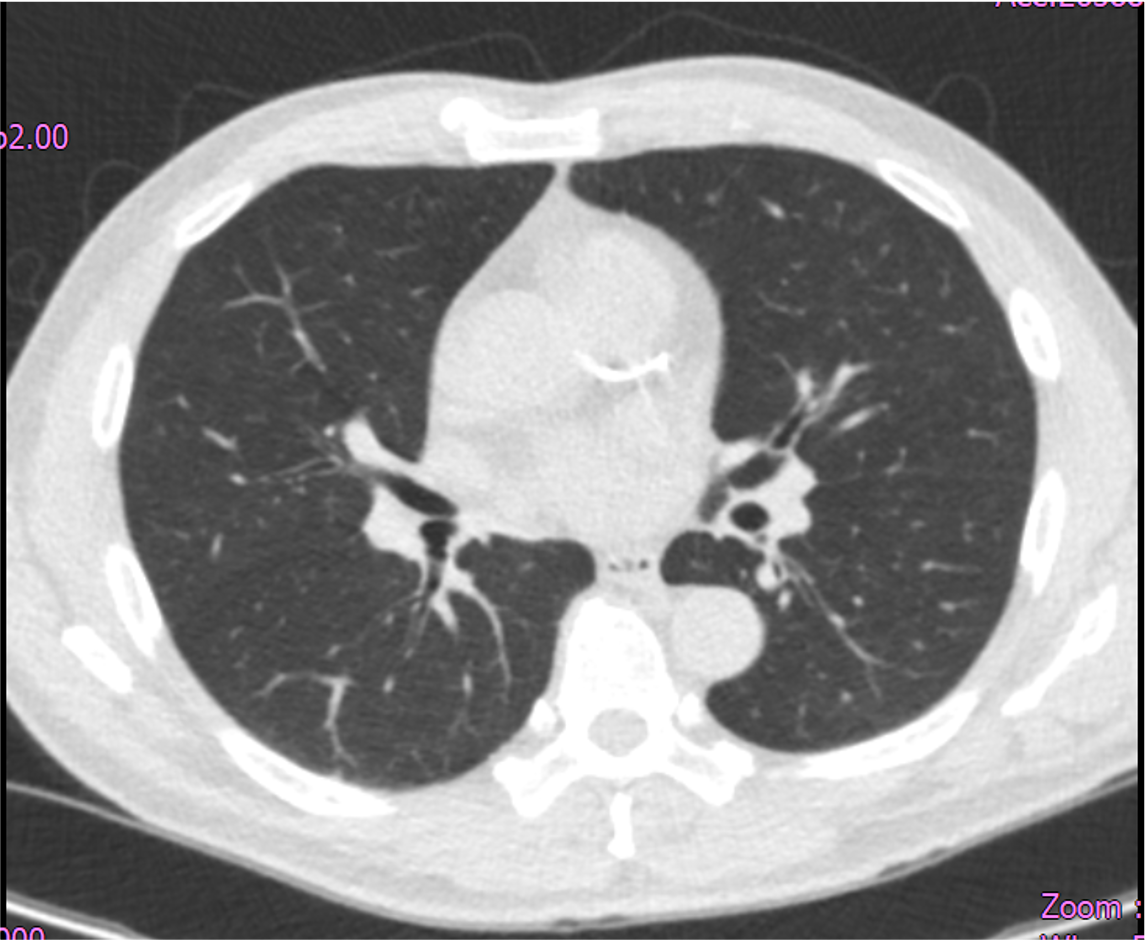
A 65-year-old man with hypertension, dyslipidemia, hyperuricemia, and CKD stage 3 presents with unstable angina. He had a positive treadmill test three years ago but deferred angiography. Recent LDCT for cough survey disclosed a coronary calcified lesion. He reports smoking 2 PPD, with no family history of cardiovascular disease. Physical examination shows normal heart sounds with no murmurs and no signs of heart failure.
Relevant Test Results Prior to Catheterization
Echocardiography showed adequate systolic and diastolic function, with no reginal wall motion abnormality detected. Thallium study showed moderate stress induced ischemia involving the inferior and basal inferoseptal segments, and mild ischemia involving the apex, mid anterior, and basal anteroseptal segments, indicating multi-territory inducible ischemia.
Relevant Catheterization Findings
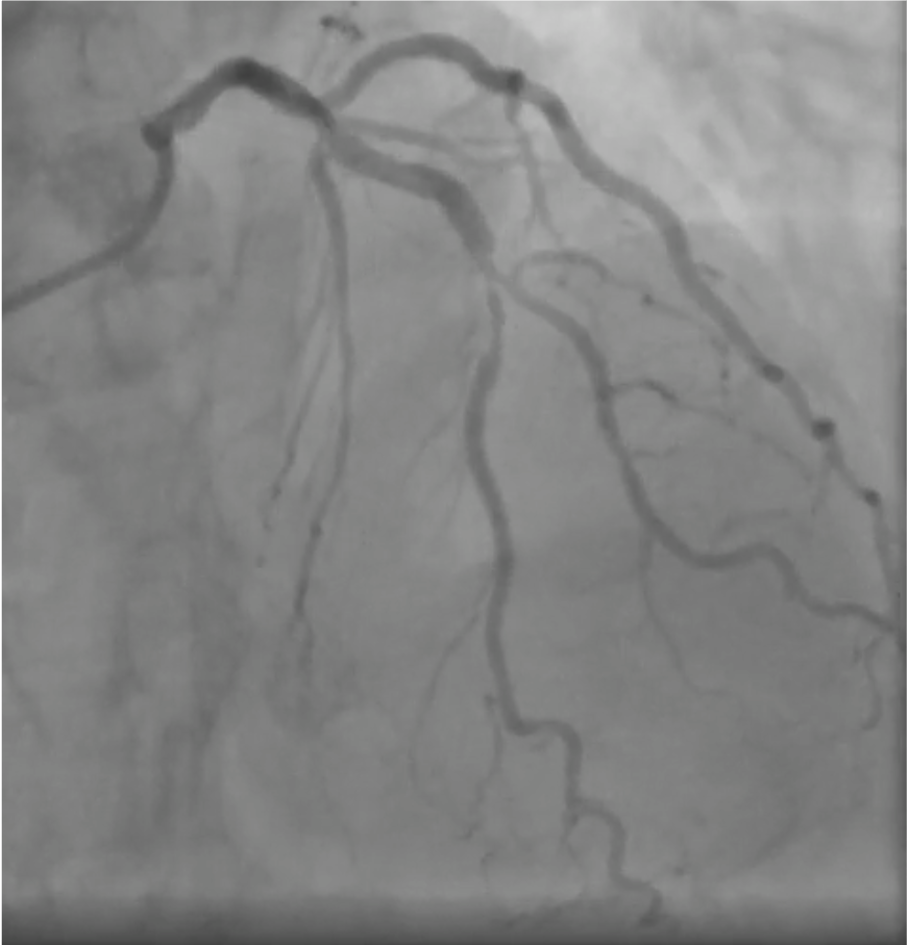
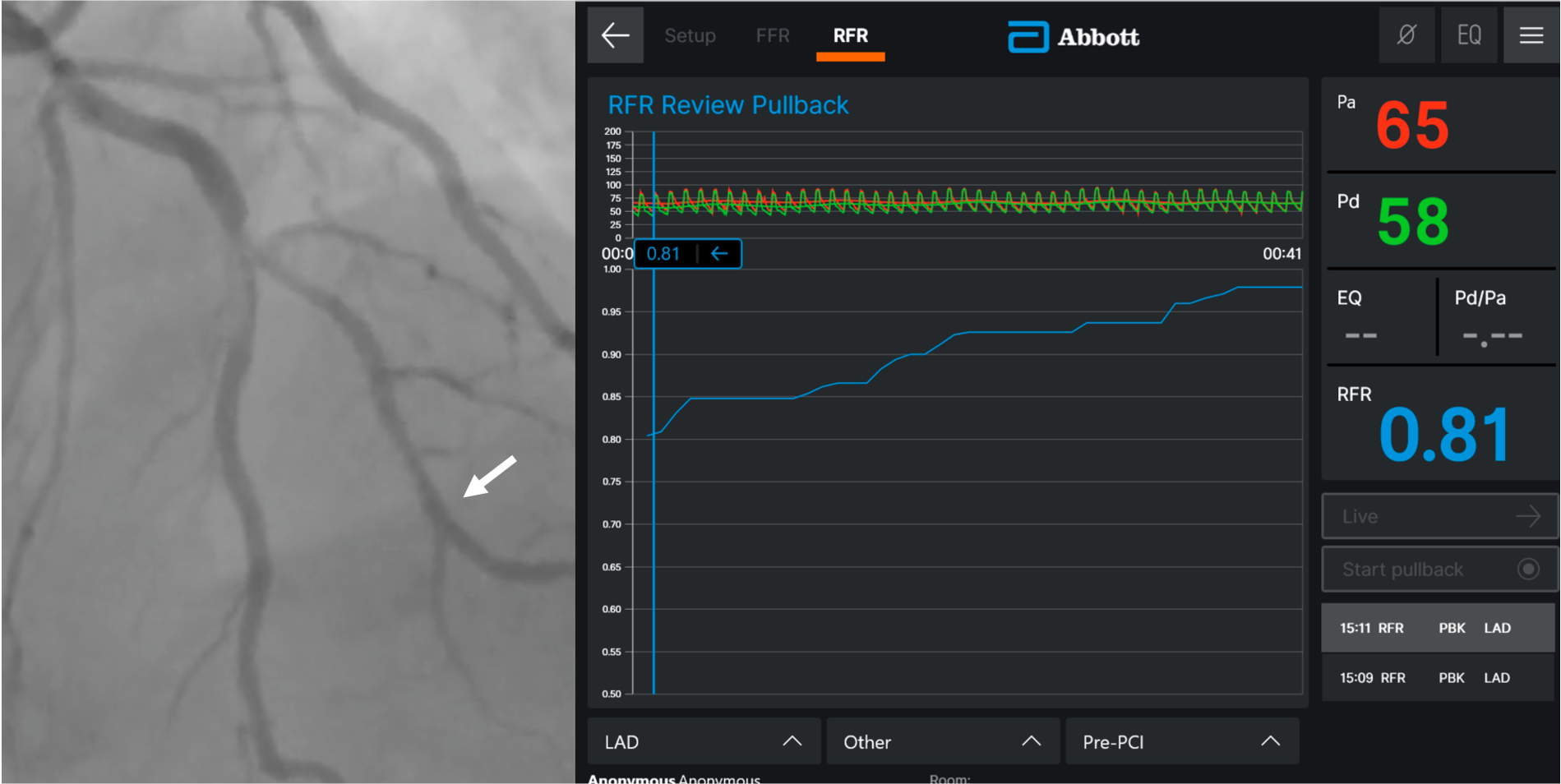
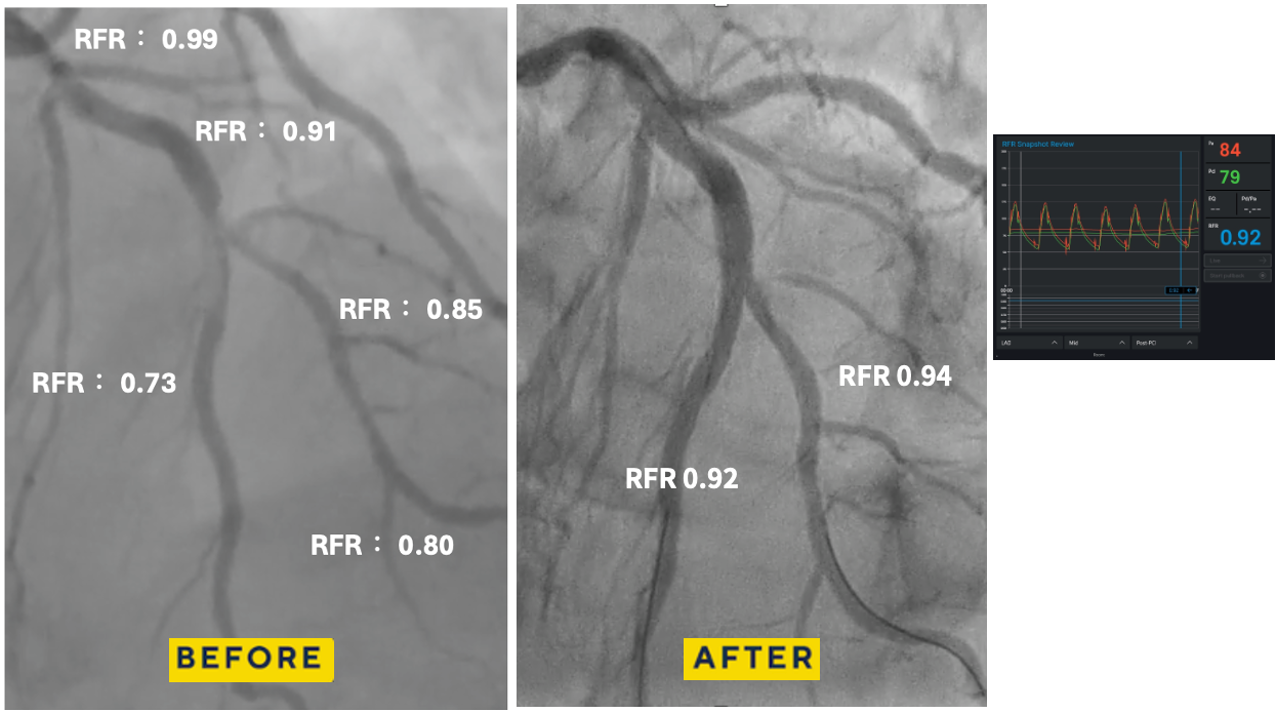
Coronary angiography via left distal radial access revealed two-vessel coronary artery disease. A true LAD–Diagonal bifurcation lesion (Medina 1.1.1) was noted, with 80% stenosis in the LAD middle segment and 80% stenosis at the D2 ostium. The proximal RCA showed critical 99% stenosis. Resting coronary physiologic indices showed: LAD-O 0.99, LAD-M 0.73, LAD-D2 0.80

 RCA.mp4
RCA.mp4
LCA.mp4
Interventional Management
Procedural Step
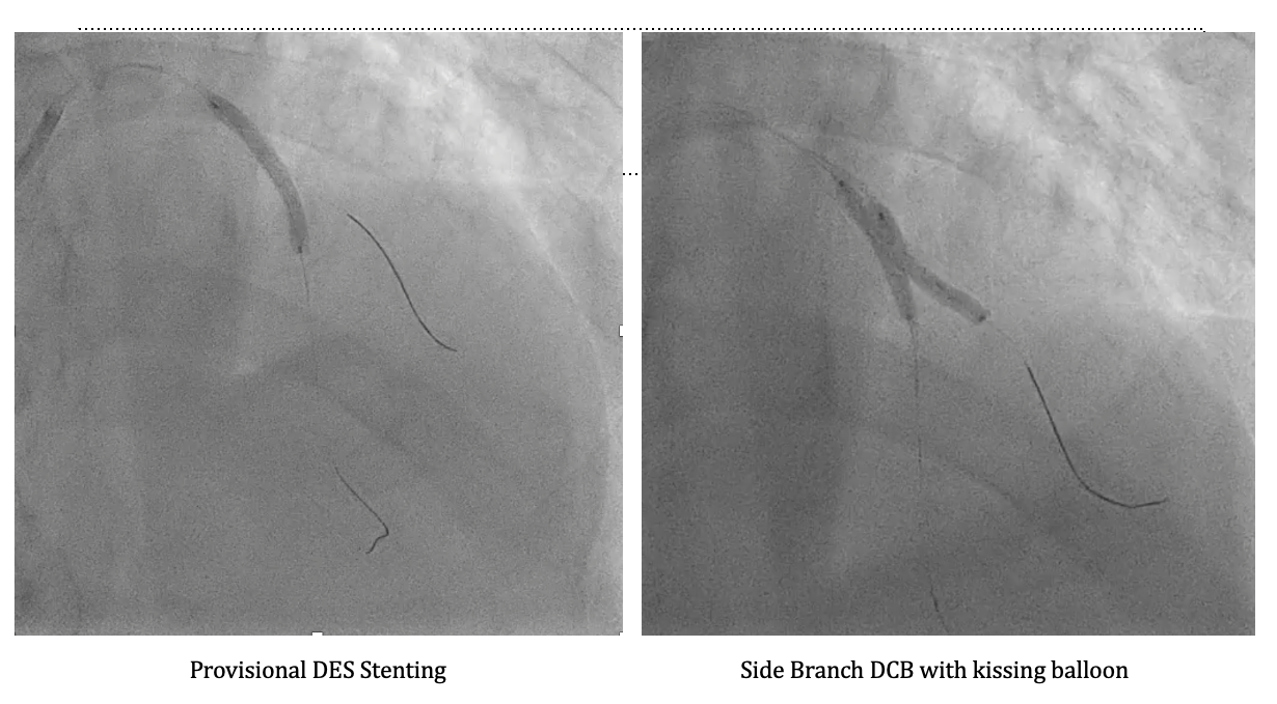
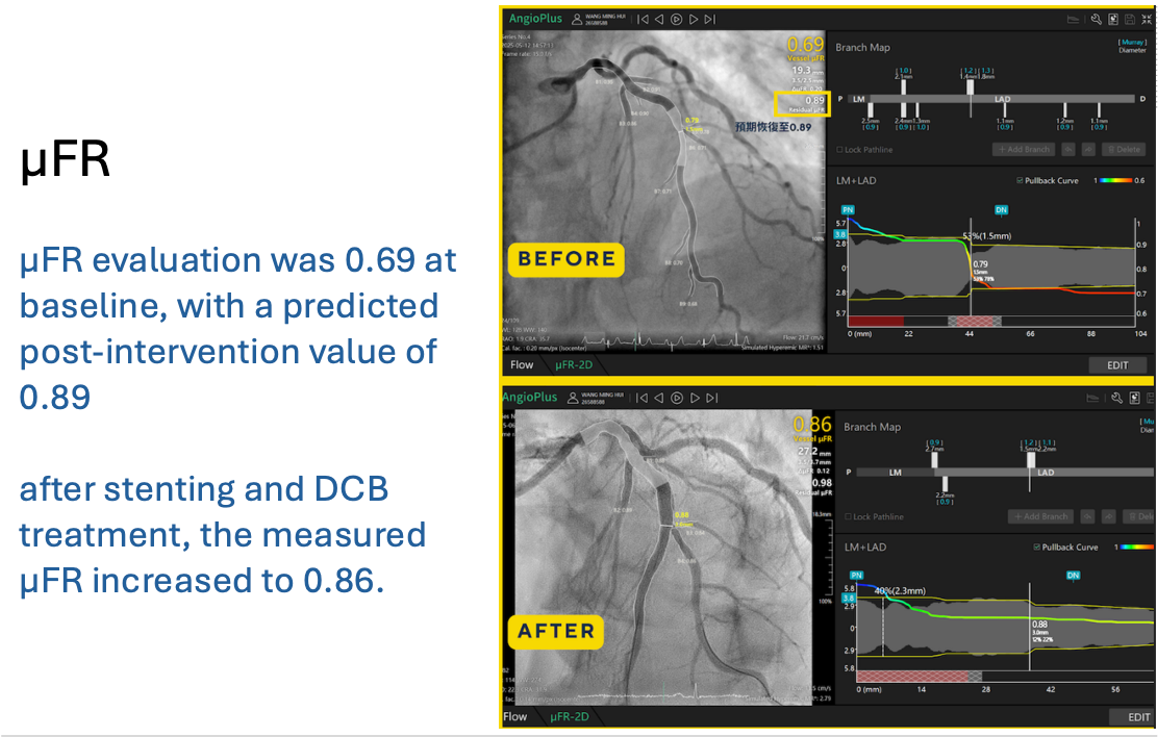
PCI was performed using a 6-in-7 Fr sheath through left radial access. Two wires were advanced (Pilot 50 to LAD-D and Terumo Floppy to LAD-D2), followed by predilatation of the LAD-M lesion with a 2.0×20 mm balloon. OCT of LAD-M demonstrated a mixed fibroatheroma with superficial calcification <90°, some 90–180° beyond the LAD-D2 bifurcation, and a lipid pool proximal to the bifurcation, with calcification on the same side of the D2 ostium, guiding reference sizing to 3.0 mm distally and 4.25 mm proximally. OCT of LAD-D2 showed mixed fibroatheroma with ~90° superficial calcium and distal reference ~3.0 mm. Kissing balloon predilatation was performed, followed by Onyx Frontier 3.0×26 mm DES deployment in LAD-M and POT with a 4.0×12 mm NC balloon. Distal rewiring was performed, and incomplete distal stent expansion was corrected with a 3.0×20 mm NC balloon. The side branch cell was opened using kissing balloon inflation. Post-stent RFR improved (LAD-D2: 0.73→0.94; LAD-M: 0.80→0.92), supporting DCB treatment for LAD-D2 with PREVAIL 3.0×20 mm/10 ATM, followed by kissing balloon. OCT confirmed good apposition but underexpansion at LAD-M, which improved after further post-dilatation (MSA 3.53→3.79 mm; expansion 65→82%). Final POT was performed with a 4.0×12 mm NC balloon. OCT of LAD-D2 showed a dissection to the media without flow limitation. The patient remained comfortable, and final physiology was good. The intended hybrid DCB side-branch treatment strategy was achieved.
DCB kissing.mp4
stenting.mp4
FINAL.mp4
Case Summary
This case illustrates that not every Medina 1.1.1 bifurcation lesion requires a two-stent strategy. OCT guided accurate lesion characterization and sizing for optimized main branch DES implantation, while RFR confirmed physiologic improvement and supported selective DCB treatment for the side branch. This hybrid approach preserved bifurcation geometry and avoided unnecessary metal. Moreover, this strategy aligns with the recent DCB Academic Research Consortium Position Statement, which endorses DCB use in appropriately selected bifurcation lesions following adequate lesion preparation and imaging guidance.