Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_019
Nightmare at Midnight: Troubleshooting in Left Main Stenting
By Hsuan-Ling Tseng
Presenter
Hsuan-Ling Tseng
Authors
Hsuan-Ling Tseng1
Affiliation
Chi-Mei Medical Center, Taiwan1
View Study Report
CASE20251106_019
Coronary - Complex PCI - Left Main
Nightmare at Midnight: Troubleshooting in Left Main Stenting
Hsuan-Ling Tseng1
Chi-Mei Medical Center, Taiwan1
Clinical Information
Relevant Clinical History and Physical Exam
A 60-year-old woman with CAD (2-V-D), s/p PCI with DES to mLAD and pLCX on 11/13/2024 (LM 40% stenosis), T2DM, hypertension, and dyslipidemia, presented with sudden chest tightness and dyspnea at midnight on 05/29/2025. Vital signs: T 37.4 °C, P 91/min, R 18/min, BP 162/84 mmHg. Appeared anxious but alert; lungs with bilateral basal rales; heart sounds regular, no murmur.
Relevant Test Results Prior to Catheterization
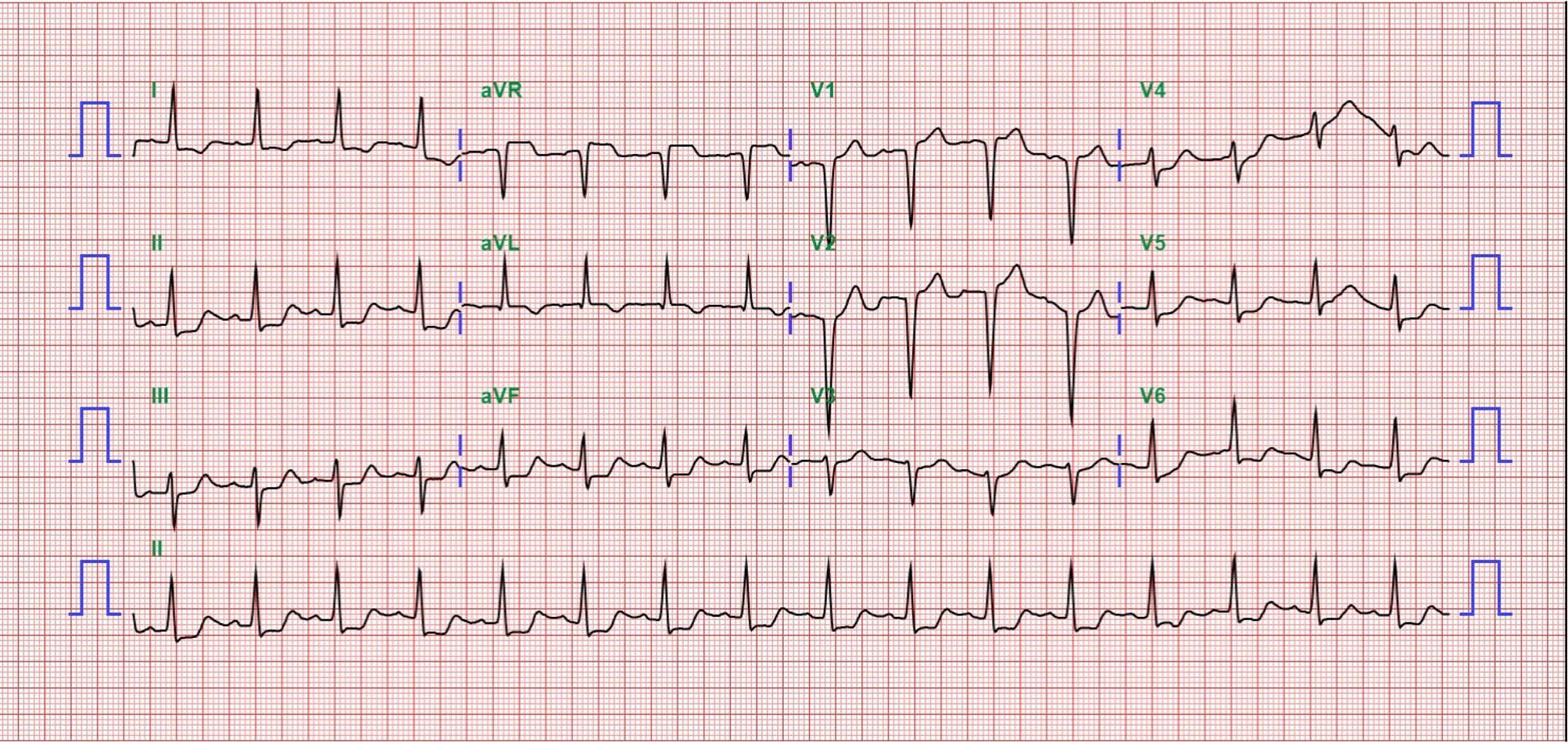
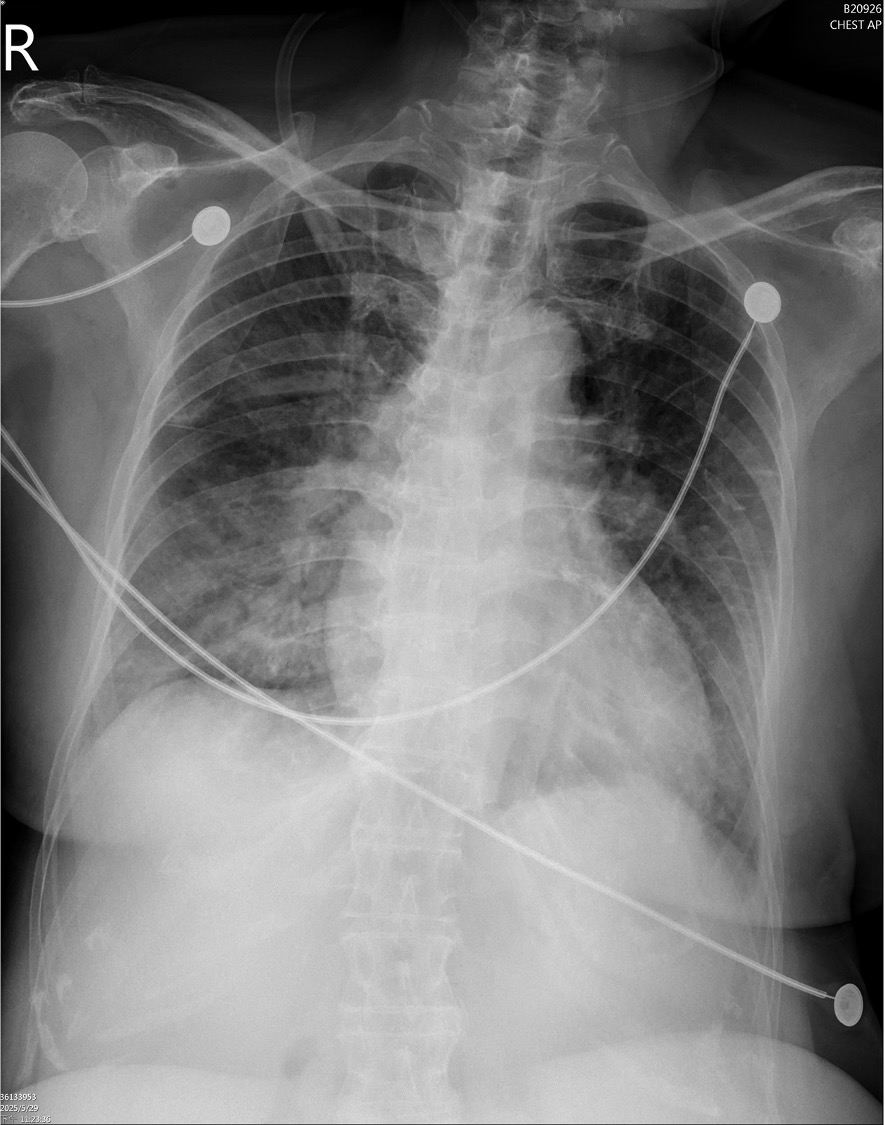
ECG showed ST elevation in aVR with diffuse ST depression. Chest X-ray revealed bilateral pulmonary edema. Laboratory data demonstrated elevated hs-troponin I (1012 pg/mL). Bedside TTE revealed global hypokinesis with an estimated LVEF of 40%.
 A4C.mp4
A4C.mp4
LAX.mp4
Relevant Catheterization Findings
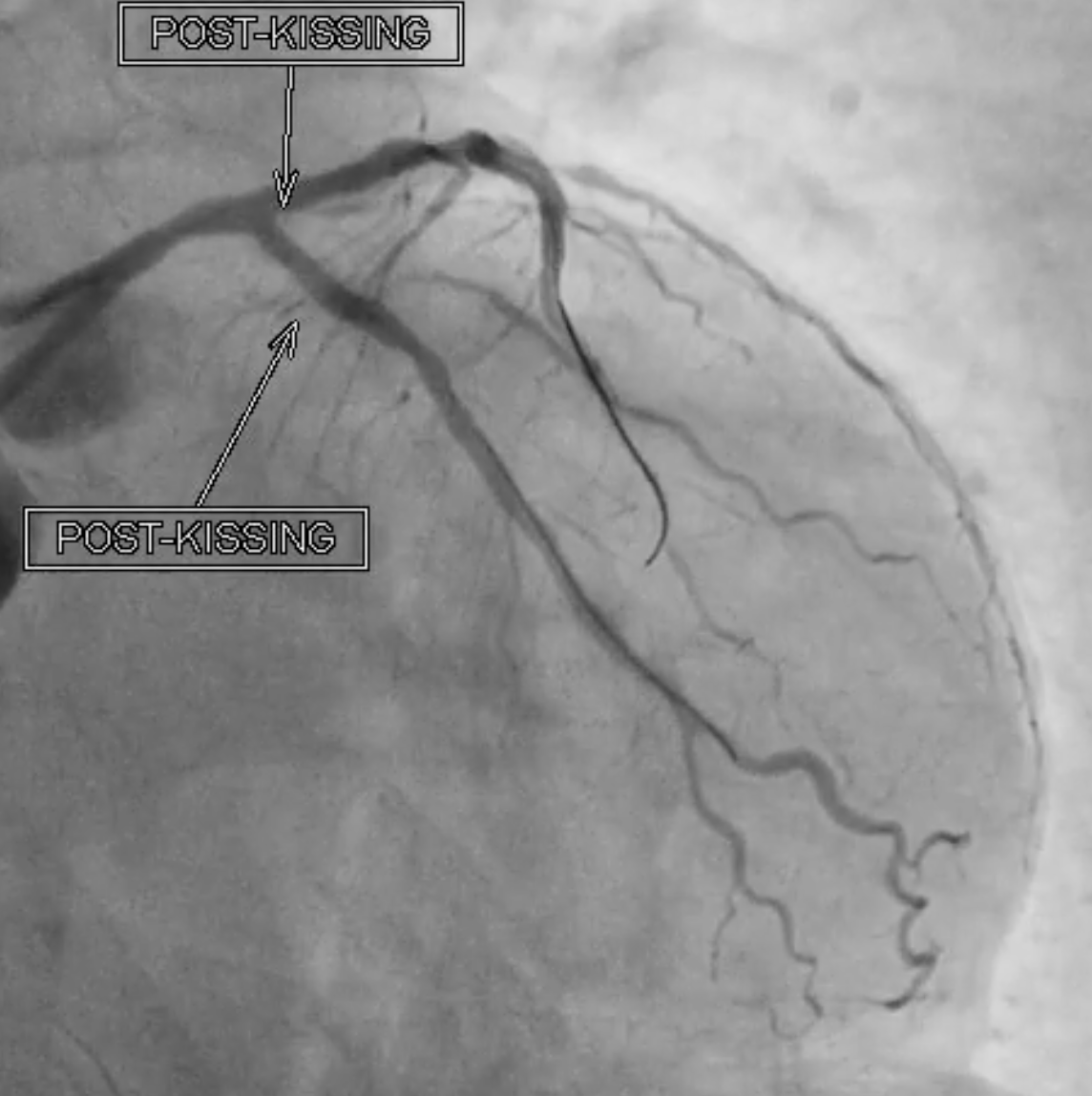
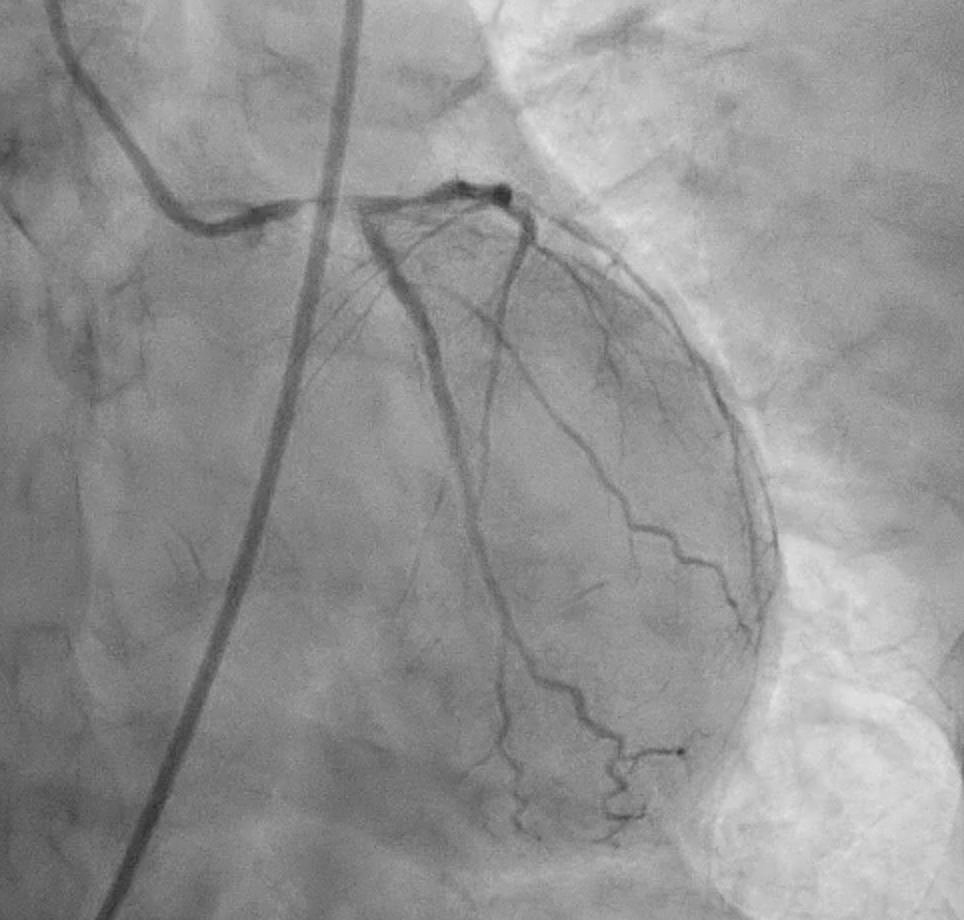
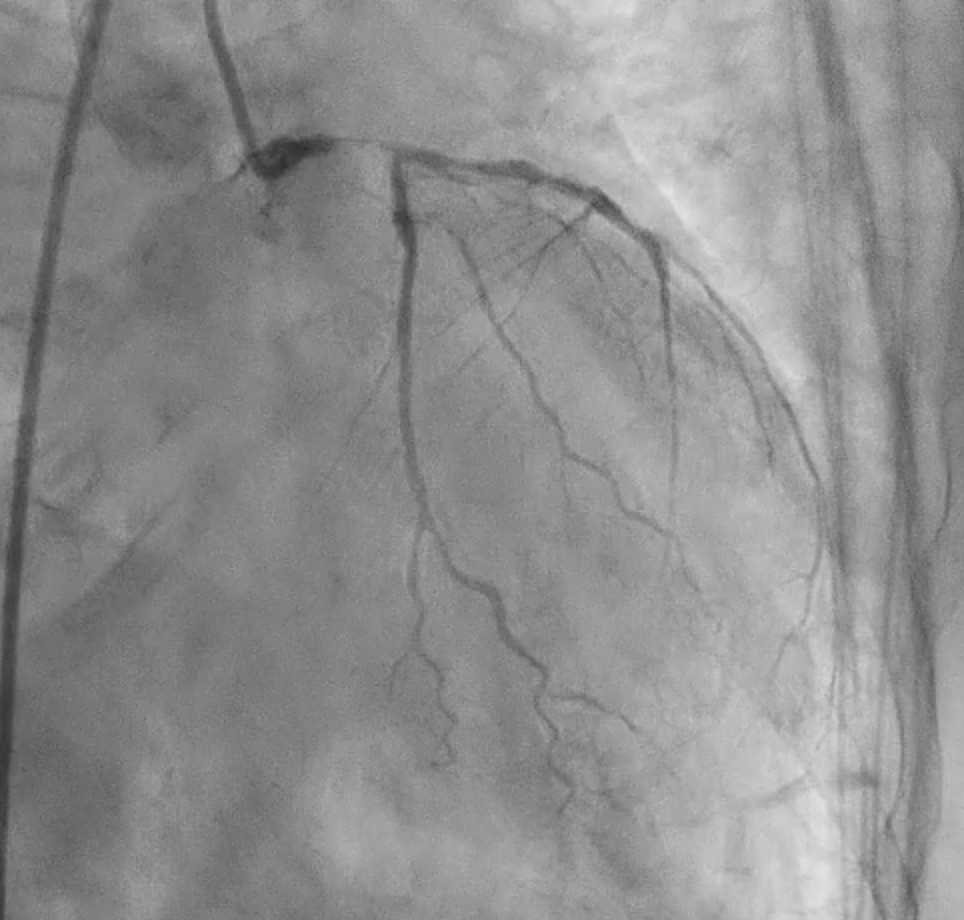
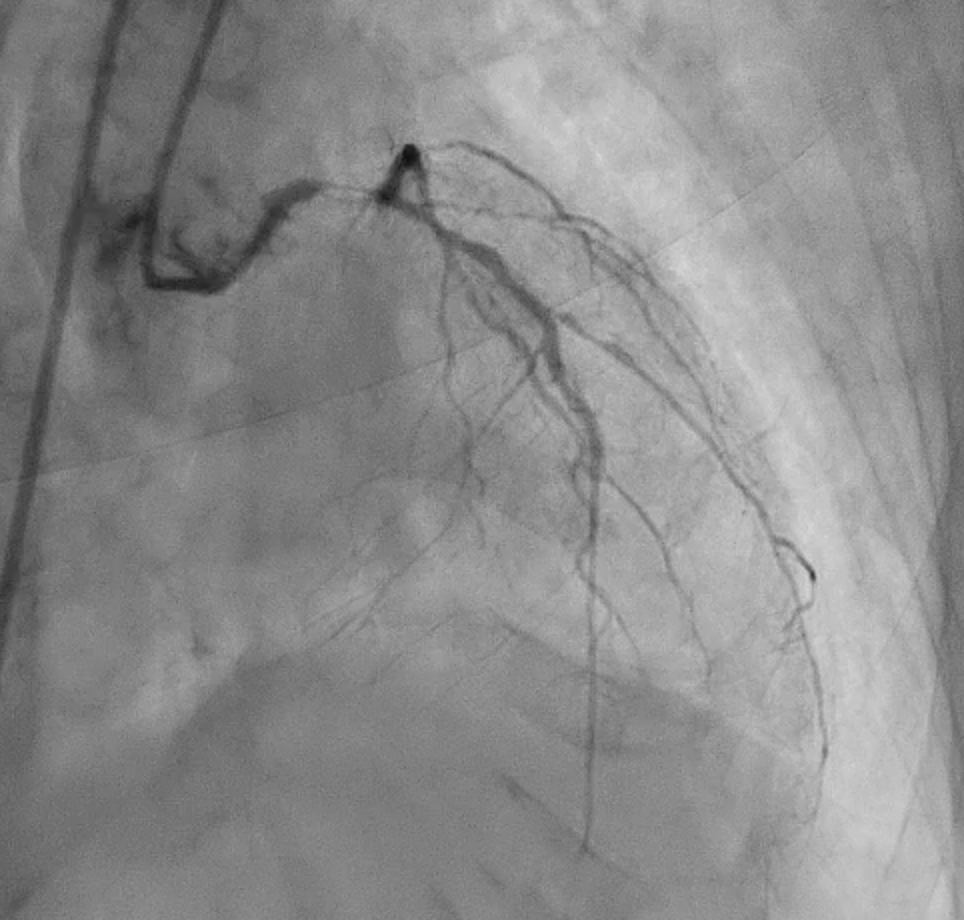
Severe CAD with LM + 3-vessel disease. dLM and shaft: critical stenosis; pLAD: critical stenosis; mLAD: s/p DES with stent underexpansion and proximal stent-edge restenosis; pLCX: s/p DES with proximal stent-edge restenosis; mRCA: 50% stenosis. SYNTAX score: 44.
CAG(6).mp4
CAG(8).mp4
CAG(10).mp4
Interventional Management
Procedural Step
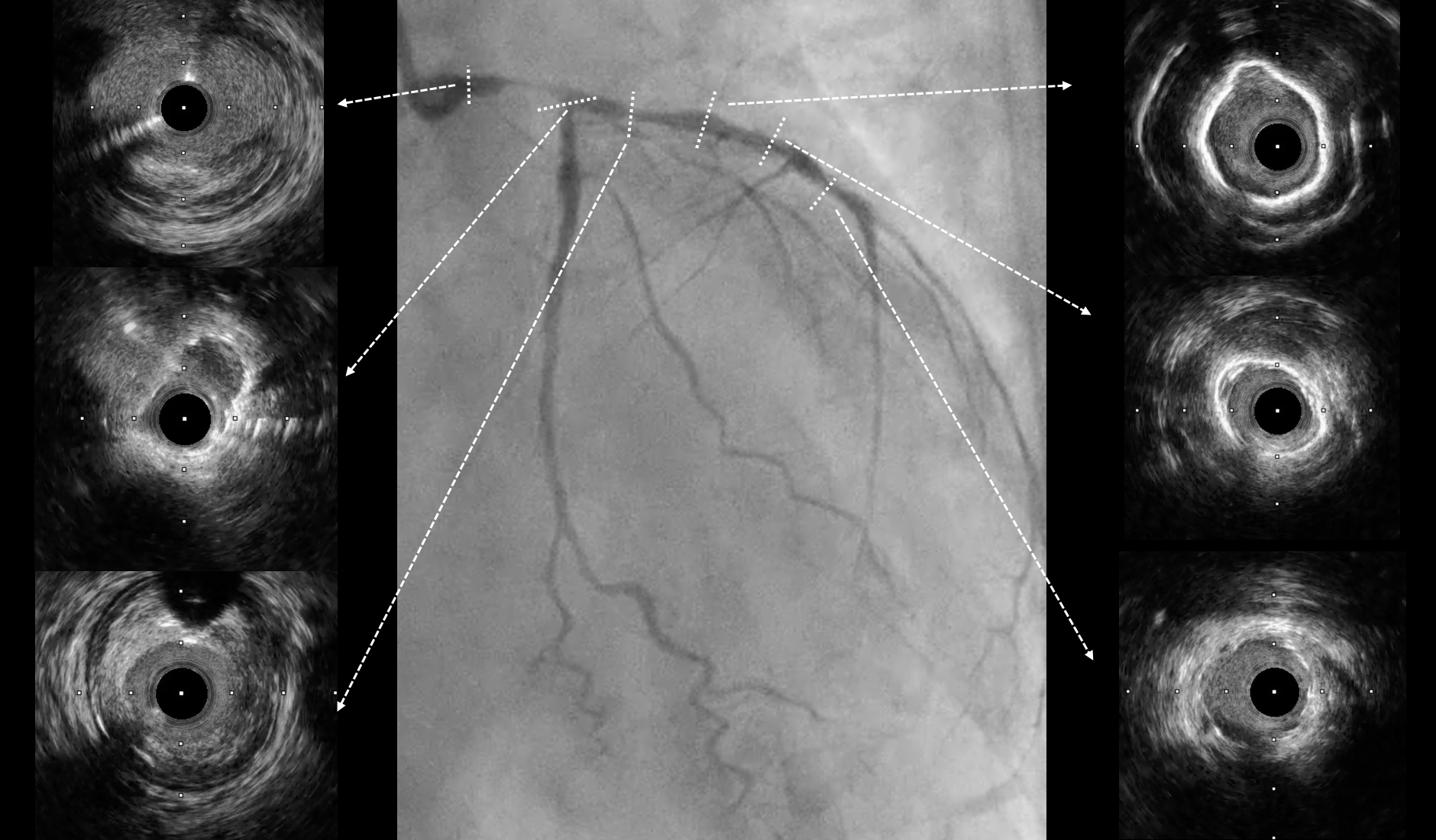
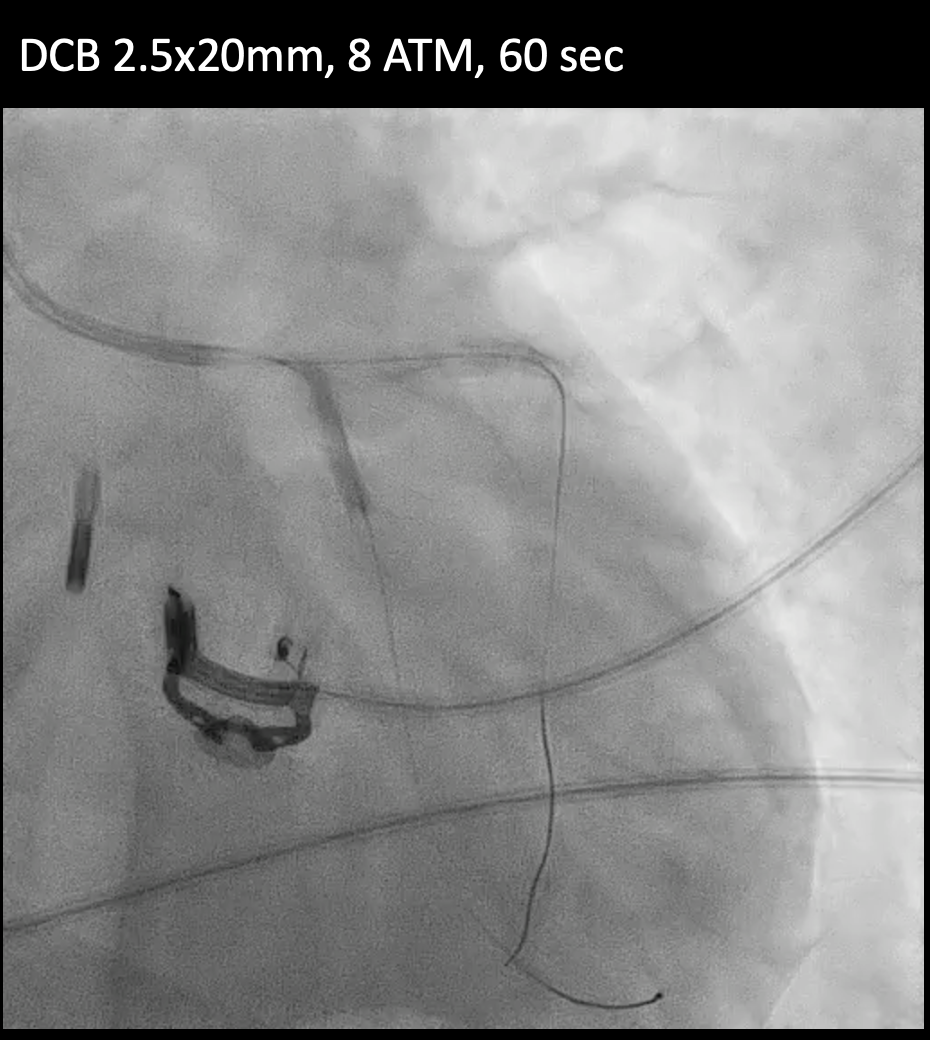
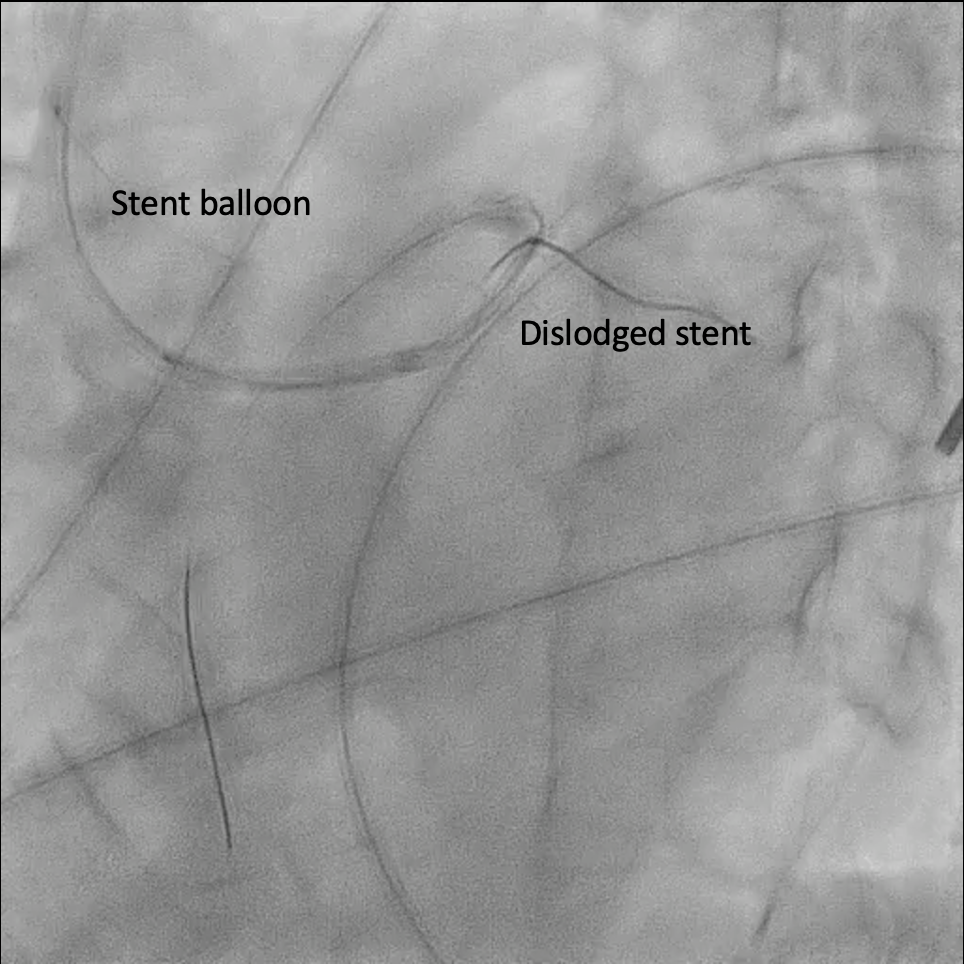
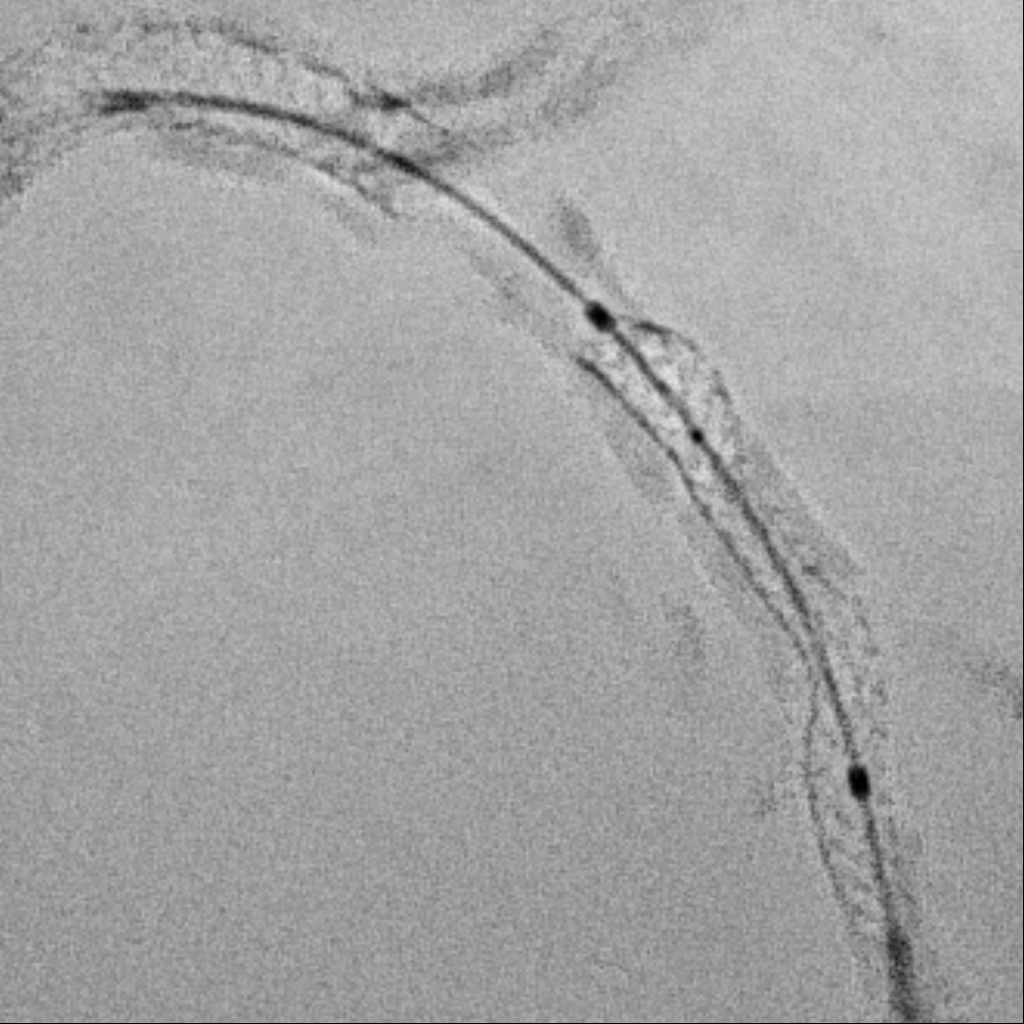
Under IABP (left femoral), PCI via right brachial with 6 Fr EBU 3.5. Runthrough to LAD, Sion Blue to LCX. Predilation of LM/pLAD with 2.0×20 mm balloon; IVUS pullbacks. Further dilatation with 2.5×20 mm NC for mLAD underexpansion, pLAD, and LM. oLCX de novo and pLCX edge ISR predilated with 2.5×20 mm NC; LCX ISR treated with DCB 2.5×20 mm. Szabo technique attempted for LM–LAD with a 3.0×24 mm DES; the undeployed stent dislodged during repositioning and was deployed at the dislodgement site. IVUS showed 2–3 struts protruding into the aorta from the LM ostium and incomplete pLAD coverage. Post-dilation with 3.5×20 and 2.5×20 mm NC; DCB 3.0×20 mm for pLAD uncovered plaque and mLAD proximal edge ISR. Final CAG: TIMI 3 flow.At 3 months, staged PCI via right radial with 6 Fr EBU 3.5. Sion Blue ES to distal LAD. IVUS: mLAD stent underexpansion (MSA <2.0 mm²); wire not through struts. IVL 3.5×12 mm initially could not cross LM; after guide exchange (JL 3.5, then EBU 3.0/3.5), IVL advanced to mLAD and delivered 100 shocks, producing a ring crack and area gain. Further dilation with 3.0×20 and 3.5×20 mm NC. IVUS: pLAD type B dissection without flow limitation. DCB 3.5×40 mm to p–mLAD. LM ostial stent further dilated with 3.5×20 mm. Final CAG: TIMI 3 flow.
CAG(38).mp4
CAG(61).mp4
IVL(61).mp4
Case Summary
Timing matters as much as technique—operator fatigue and suboptimal midnight conditions can silently amplify risks in complex PCI. Past success can bias current judgment; repeating a previously effective technique may overlook new anatomical nuances. Guiding catheter engagement is double-edged: while it enhances support, it compromises precision at the ostium. Preparation should anticipate rare complications, not just manage common ones.