Lots of interesting abstracts and cases were submitted for TCTAP 2026. Below are the accepted ones after a thorough review by our official reviewers. Don’t miss the opportunity to expand your knowledge!
CASE20251106_017
Endovascular Repair of Infrarenal Abdominal Aortic Aneurysm With Left Iliac Stenosis and Tortuous Anatomy: Pre-EVAR PTA and Ballerina (Crossed-Limb) Configuration for Optimal Device Delivery
By Kevin Francio, Rendra M. Putra, Nadya Luthfah, Raden M. Budiarto, Johanes Nugroho E. Putranto
Presenter
Kevin Francio
Authors
Kevin Francio1, Rendra M. Putra2, Nadya Luthfah1, Raden M. Budiarto1, Johanes Nugroho E. Putranto1
Affiliation
Soetomo General Academic Hospital, Indonesia1, Universitas Airlangga, Indonesia2
View Study Report
CASE20251106_017
Endovascular - Thoracic & Abdominal Aortic Interventions
Endovascular Repair of Infrarenal Abdominal Aortic Aneurysm With Left Iliac Stenosis and Tortuous Anatomy: Pre-EVAR PTA and Ballerina (Crossed-Limb) Configuration for Optimal Device Delivery
Kevin Francio1, Rendra M. Putra2, Nadya Luthfah1, Raden M. Budiarto1, Johanes Nugroho E. Putranto1
Soetomo General Academic Hospital, Indonesia1, Universitas Airlangga, Indonesia2
Clinical Information
Relevant Clinical History and Physical Exam
An 86-years-old woman presented with abdominal discomfort and a mass-like sensation. Abdominal ultrasound revealed an abdominal aortic aneurysm (AAA), which was confirmed by CTA. She was hemodynamically stable with no signs of rupture. Physical examination showed peripheral pulses palpable bilaterally, and the case was planned for elective endovascular aneurysm repair (EVAR) under general anesthesia.

Relevant Test Results Prior to Catheterization
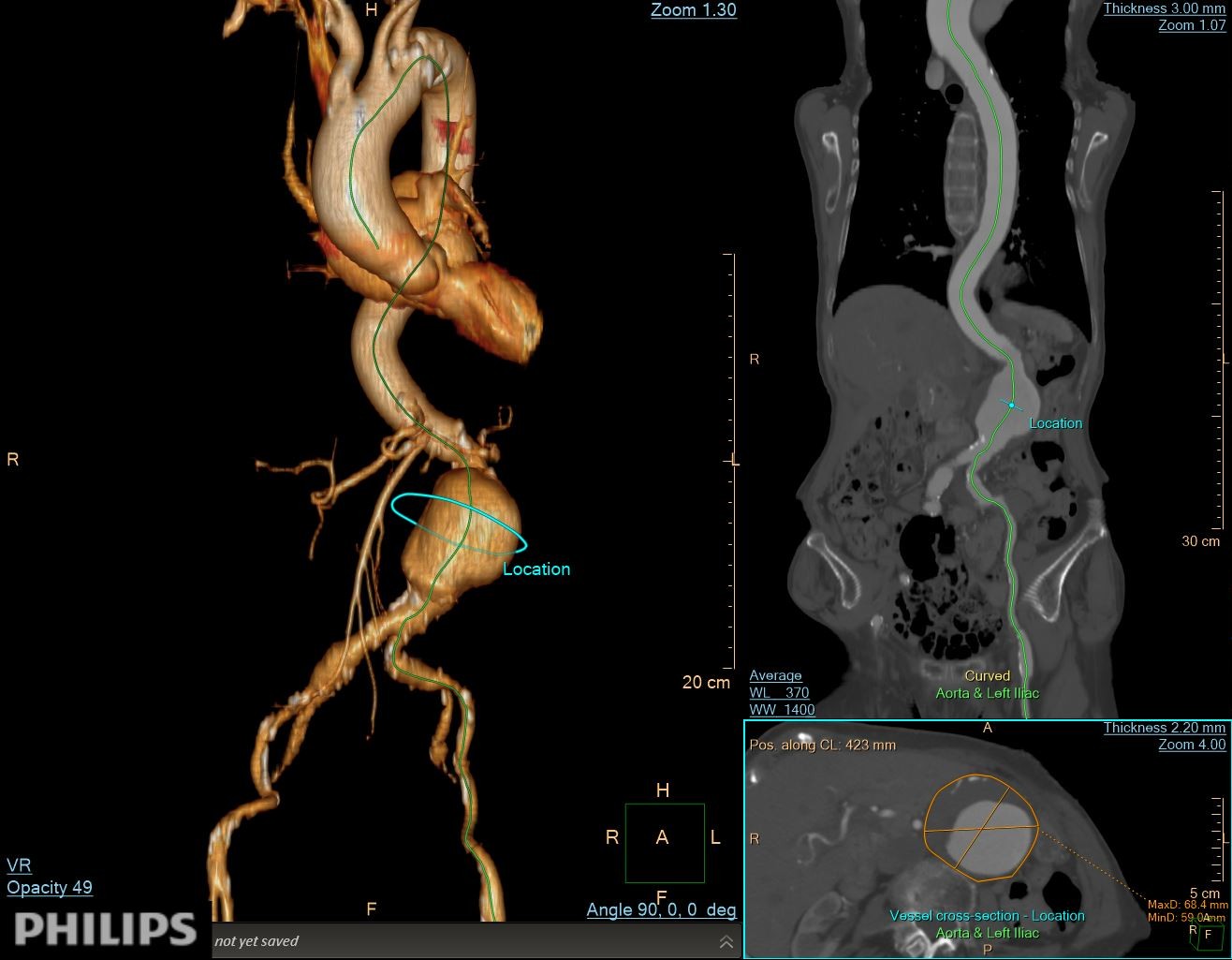
CTA demonstrated a fusiform infrarenal AAA measuring 65–68 mm with partial mural thrombus but a thrombus-free proximal neck. The neck measured 19 mm in length, tapering from 19 to 17 mm with mild (≈46°) angulation and partial mural calcification. Diffuse aorto-iliac calcification was noted with >70% stenosis and tortuosity of the left common iliac artery, while the right iliac axis appeared relatively straight. RCFA and LCFA diameters were 9.4 mm and 7.6 mm.
Relevant Catheterization Findings
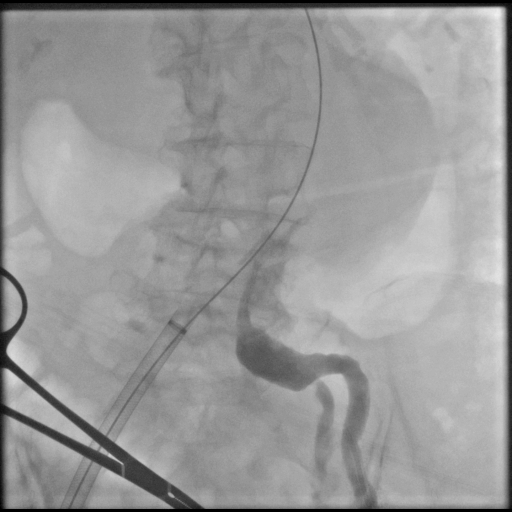
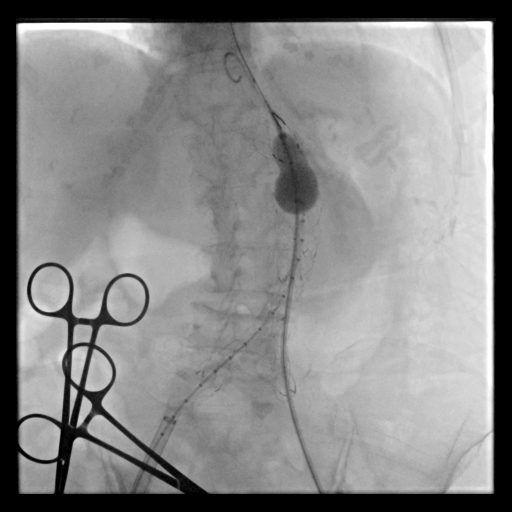
Under general anesthesia, bilateral common femoral arteries were accessed percutaneously under ultrasound guidance, and the pre-close technique with Perclose ProGlide (Abbott Vascular, USA) was applied. Angiography confirmed a large infrarenal AAA and left common iliac artery with severe stenosis (>70%) and marked tortuosity, while the right iliac was relatively straight. Guidewire advancement through the left side was difficult due to narrowing and vessel curvature.
 06 Aortography Pre.mp4
06 Aortography Pre.mp4
01 LCIA Angio Pre PTA.mp4
Interventional Management
Procedural Step
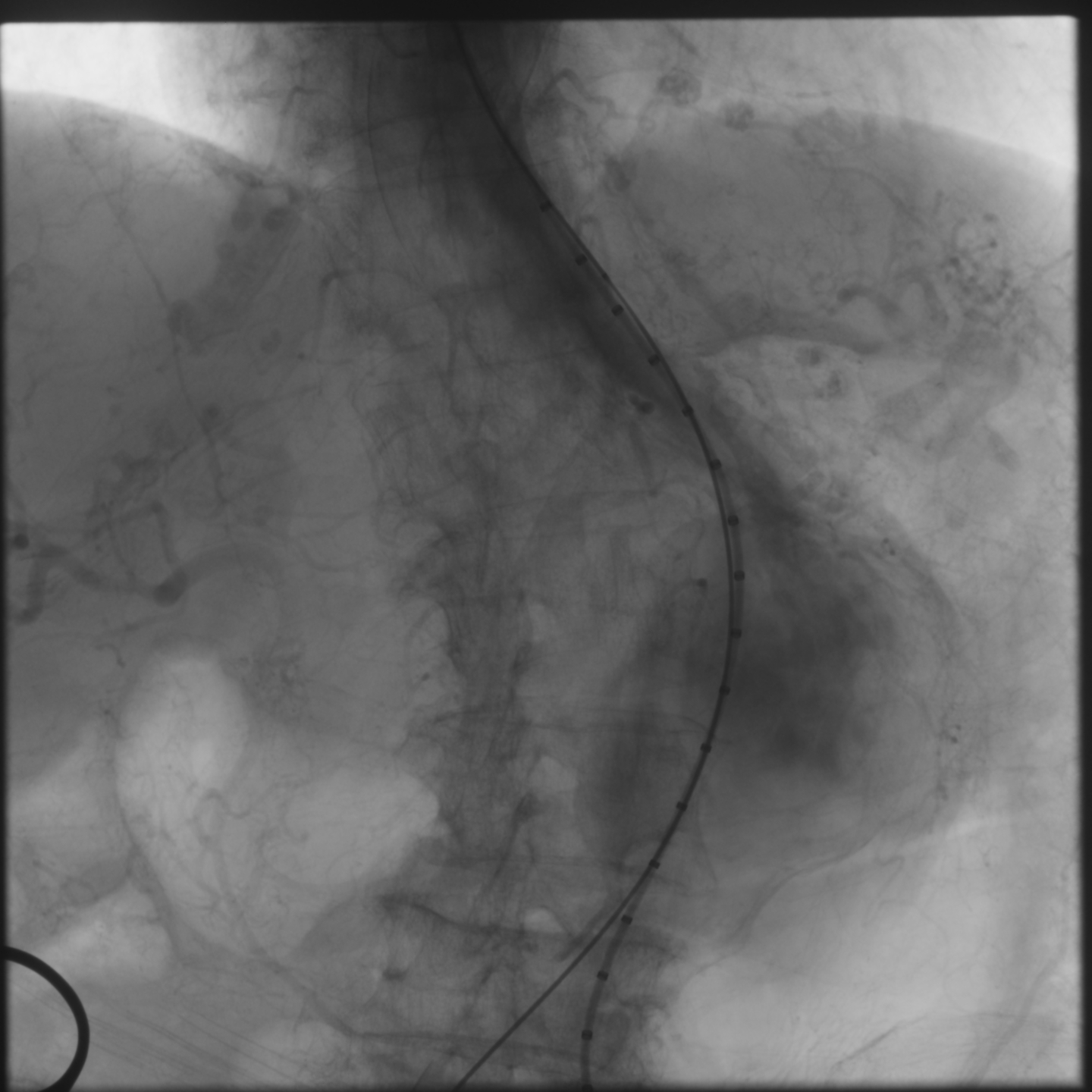
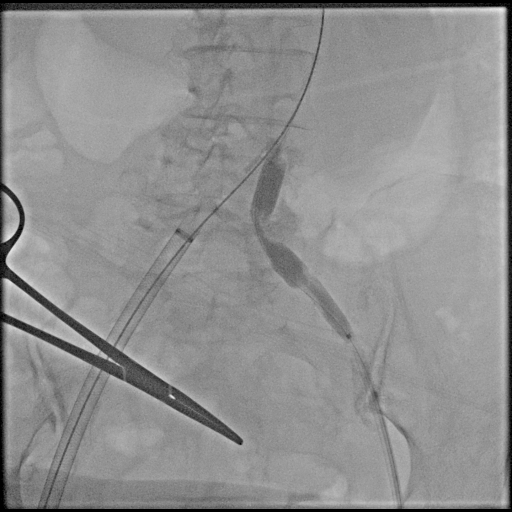
Percutaneous transluminal angioplasty (POBA) was performed on the proximal left common iliac artery using a 10 × 80 mm Mustang balloon (Boston Scientific, USA) inflated and showing a balloon-waist formation consistent with a tight, fibrotic lesion. After gradual dilation up to 6 atm, the waist resolved and the lumen expanded, allowing smooth wire and sheath passage. The SEAL NOVUS stent-graft system (S&G Biotech, Korea) was used, with the main body (24 × 50 mm) introduced via the right common femoral artery. Two flared iliac limbs, 12(18) × 100 mm on the left and 12(16) × 80 mm on the right, were deployed in a ballerina (crossed-limb) configuration to accommodate left-sided tortuosity and prevent kinking. During contralateral limb cannulation, angiography was performed within the main body to confirm the wire course inside the graft before advancing the sheath. Completion angiography demonstrated a Type Ia endoleak, treated with proximal neck flaring using a Coda LP balloon (Cook Medical, USA) under a rapid inflation–deflation technique to optimize sealing and prevent graft migration. Final angiography showed excellent proximal seal and bilateral flow, and follow-up CTA confirmed durable aneurysm exclusion without endoleak.
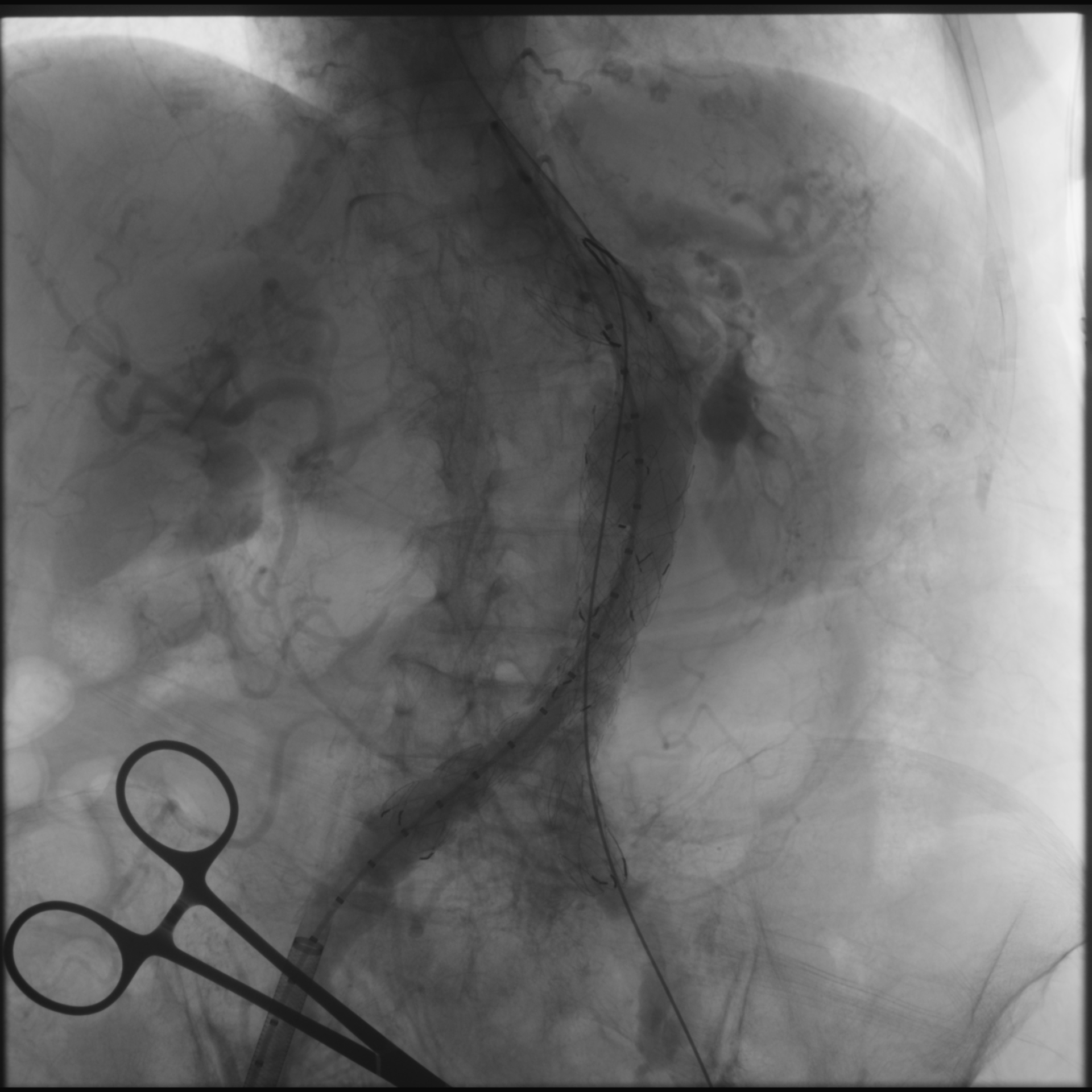
24 Aortography post EVAR Delayed.mp4
03 LCIA Balloon Inflating 1.mp4
20 Coda LP Balloon 1.mp4
Case Summary
In EVAR cases with asymmetric iliac anatomy, pre-EVAR PTA of stenotic and tortuous vessels can significantly improve device deliverability and procedural safety. The ballerina configuration offers a practical solution for optimizing limb orientation and seal integrity. Meticulous stepwise management, including angioplasty-assisted access and intrastent angiographic confirmation of true graft lumen position, ensures safe delivery and accurate graft placement. Early recognition of access complexity and readiness to modify configuration intra-procedurally can enhance outcomes and expand EVAR feasibility in challenging anatomies.